Understanding Glomangiopericytoma: A Case Report of a Rare Sinonasal Tumor
Introduction: Glomangiopericytoma (GPC) is a benign neoplasm of the sinonasal tract that consists of spindle-shaped to ovoid cells with lobular or nodular growth patterns. GPCs are low-malignant tumors due to limited mitotic activity and atypia, making them less aggressive. The etiology of GPC remains unknown but is associated with factors like steroid use, past trauma, pregnancy, and hypertension. GPC is more common in women and is usually diagnosed in the sixth and seventh decades of life. Case Presentation: This article presents a case of a 47-year-old woman with a history of type-2 diabetes and nasal obstruction who was diagnosed with glomangiopericytoma (GPC), a rare sinonasal tumor. Computed tomography revealed a vascular mass, and complete surgical resection was achieved via a trans-nasal approach. The diagnosis was confirmed through positive β-catenin staining and negative S100p and STAT6 with a low Ki67 proliferation index. The patient experienced post-operative pain, anosmia, and ageusia, which were treated successfully. This case highlights the clinicopathologic characteristics, clinical and therapeutic aspects, surgical interventions, and differential diagnosis of GPC, a rare disease with limited reports. Conclusion: Glomangiopericytomas are benign sinonasal tumors often mistaken for other neoplasms. Diagnosis is challenging but possible through excision or biopsy with histopathological examination. Endoscopic surgery with follow-up is the recommended treatment, with recurrence occurring up to 12 years post-surgery. CTNNB1 gene mutations and β-catenin nuclear expression are recent diagnostic markers. GPC has a high survival rate and low metastasis, but patients should be closely monitored. This case report underscores the importance of comprehensive diagnosis and management for these rare tumors.
Introduction
Glomangiopericytoma (GPC), previously known as hemangiopericytoma, is a rare and unusual type of neoplasm that affects the sinuses and paranasal area. This disease was first diagnosed by Stout and Murray in 1924, and since then, only limited cases have been reported in medical literature.
Glomangiopericytoma is classified as a low-malignant soft tissue tumour, which means that it is slow-growing and painless, and has a low potential to spread to other parts of the body. The nasal septum is the most common site for this tumour, followed by the paranasal sinuses and the sphenoethmoidal recess [1, 2].
This tumour can range in size from 0.5 to 14 cm, with the majority being around 5 cm in diameter [3]. It is typically reddish-polypoidal in appearance, and is diagnosed in women between the ages of 60 and 70, according to studies by Ghaloo SK, et al. [4]. The diagnosis of Glomangiopericytoma can be confirmed by positive actin and β- catenin immunostaining and negative CD34 and BCL2 immunostaining, as described by Saito Y, et al. [5].
One of the key challenges in the management of GPC is the limited knowledge about the disease, which can make diagnosis and treatment difficult. This lack of knowledge often leads to misdiagnosis, delayed treatment, and poor patient outcomes. However, a better understanding of GPC and its clinical presentation, along with advances in diagnostic techniques, can help healthcare providers to diagnose the disease more accurately and provide appropriate treatment.
Additionally, recent advances in endoscopic treatment have made complete surgical resection via a trans-nasal approach a more feasible option for patients with GPC. This type of surgery is less invasive and has a lower risk of complications compared to traditional surgical techniques, making it an attractive option for patients [3].
This article presents the case of a 47-year-old woman who was admitted with a vascular mass arising from the right sphenoethmoidal recess and extending to the choana. The case has been reported following the SCARE criteria and provides a comprehensive examination of the clinicopathologic characteristics, clinical and therapeutic aspects, surgical interventions, and differential diagnosis of Glomangiopericytoma. The study aims to shed light on this rare disease and provide valuable insights into its diagnosis and management [6].
Patient Information
The patient is a 47-year-old married woman who is on homoeopathic medications for Type-2 diabetes. She presented with a two-year history of right nasal obstruction, gradual onset, worsening with cold exposure and occasional watery nasal discharge from the right side. She has a history of mouth breathing and two episodes of epistaxis, with the most recent being 4 months prior. The patient also reports constant discomfort, dull pain in her head and bilateral ears, with no associated reduced swelling, allergies, or ear/nose/ throat symptoms.
Diagnostic Assessment and Interpretations
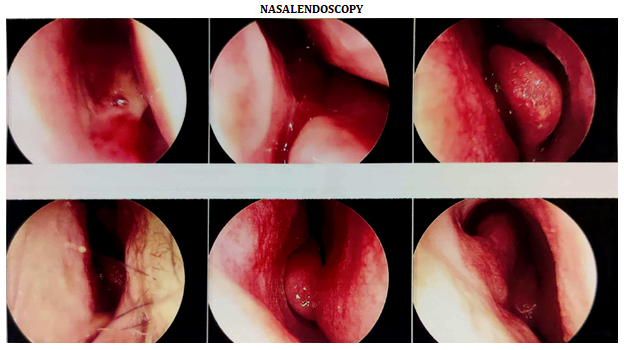
ACT scan of the patient’s sinuses showed a mass in the right nasal cavity that was determined to be a benign neoplasm (tumor) of spindle cells. Endoscopic view of tumor reveals pink or reddish-colored growths arising from the blood vessels, indicating the presence of a discernible mass or lesion (Figure 1). This observation may suggest an atypical vascular network that facilitates the tumor’s growth and development. The patient underwent surgery to remove the mass and the biopsy results confirmed the diagnosis as “Right Nasal Cavity-Sinonasal Glomangiopericytoma.” The cells were positive for β-catenin and negative for S100p and STAT6, with low levels of cell growth (<1% Ki67).
Interventions
The patient was advised to follow a “Diabetic Diet” and to irrigate their sinuses regularly with saline to prevent infections (Table 1). Nasal spray may be used after endoscopic excision to reduce inflammation and swelling in the nasal tissue, improve the healing process, and help prevent recurrence of nasal polyps or other conditions that may have been the cause of the excision. They were also given prescribed medications and instructed to report any symptoms, such as pain, swelling, or bleeding, to the healthcare provider. After the successful endoscopic endonasal surgery, the patient was stable at the time of discharge.
| Drugs | Frequency | Duration |
|---|---|---|
| T. Augmentin (625mg) | 1/1/2001 | 5 Days |
| T. Pan (40mg) | 1-0-0 | 5 Days |
| T. Odimont LC | 0-0-1 | 2 Weeks |
| Fluticone FT Nasal Spray | 2 PUFF-0-0 | 1 Month |
| Nasoclear Nasal Wash | 1-0-1 | 1 Month |
| T. Signoflam | 1-0-1 | 3 Days + SOS |
Table 1: Discharge drug advice.
Follow-Up and Outcomes
The patient’s first follow-up revealed pain at the incision site, loss of smell (loss of smell) and taste (loss of taste). However, in the most recent check-up, she was asymptomatic and a nasal endoscopy showed no signs of recurrence. The patient’s health status was improved.
Discussion
Glomangiopericytoma (GPC) is a rare type of benign tumour that is found in the sinonasal tract. This tumour is composed of spindle-shaped to ovoid cells that have a lobular or nodular growth pattern, as observed in histological studies Obeidin F, et al. [7]. According to Stout and Murray, glomangiopericytomas are characterized by a proliferation of bland and uniform spindle cells that are closely packed together and grow into the surface respiratory epithelium. The tumour cells are separated from the capillaries by a distinct vascular network, creating large vascular spaces [1].
GPCs are considered to be benign tumours, meaning that they are non-cancerous and do not spread to other parts of the body. Despite this, they can cause significant symptoms, including nasal obstruction, epistaxis, watery discharge, difficulty breathing, facial pain, anosmia, headache, and sinusitis [8]. The exact cause of GPC is still unknown, although it has been associated with the use of steroids, past trauma, pregnancy, and hypertension.
The diagnosis of GPC can be challenging due to its similarity to other lesions, such as angiofibroma, solitary fibrous tumour, sinonasal leiomyoma, and lobular capillary perivascular hyalinization. While imaging techniques, such as CT and MRI, can provide information about the tumour size and characteristics, a definitive diagnosis is usually made through histopathological analysis after complete excision or biopsy [7, 9, 10, 11].
Recent studies have identified the role of beta-catenin signaling in the pathogenesis of GPC. Aberrant activation of this pathway has been shown to promote tumor cell proliferation, angiogenesis, and invasion, leading to poor prognosis in affected individuals [12]. One study published in the Journal of Clinical Pathology analyzed 13 cases of GPC and found that all cases were positive for smooth muscle actin (SMA). The authors noted strong staining of SMA in the pericytes surrounding blood vessels, suggesting a potential diagnostic utility of this marker in GPC [13].
In a case report published in the Journal of Medical Case Reports, a patient with a GPC was found to be positive for CD34. The authors noted that CD34 is a useful marker for identifying tumors with a perivascular growth pattern, such as GPC [14].
Another study published in the International Journal of Clinical and Experimental Pathology found that Ki-67, a marker of cell proliferation, was significantly higher in cases of GPC that recurred. This suggests that Ki-67 may be a useful marker for predicting the aggressiveness of GPC and identifying patients who may benefit from more aggressive treatment [15].
Endoscopic surgery is considered to be the best treatment modality for GPC due to its excellent prognosis. This type of surgery allows for complete surgical resection through a trans-nasal approach, and advances in endoscopic treatment have made it a popular choice for managing this type of tumour. Wide excision is thought to increase survival duration, while incomplete excision may cause recurrence [5].
GPCs are considered to be low-malignant tumours with a low rate of metastasis, estimated to be in the range of 5-10%. This is because they are atypical in nature and have limited mitotic activity, making them less aggressive and less likely to spread to other parts of the body [3, 16].
Glomangiopericytoma is a rare tumor that requires increased reporting and awareness among medical professionals and patients. As a surgeon or physician, recognizing the unique features of this tumor is crucial to promote early diagnosis and treatment. However, due to its rarity, glomangiopericytoma may be easily misdiagnosed or overlooked, leading to delays in treatment and potentially worse outcomes for patients. Therefore, it is important to have a high index of suspicion for this tumor when evaluating patients with unexplained symptoms.
Conclusion
In conclusion, glomangiopericytomas are a type of benign tumor that occur in the sinonasal tract and can be mistaken for several other spindle cell and vascular neoplasms. GPC is frequently confused with other lesions such as angiofibroma, lobular capillary perivascular hyalinization, solitary fibrous tumour, and sinonasal leiomyoma. The diagnosis can be challenging, but it can be established through complete excision or biopsy with histopathological examination. The best treatment option for GPC is endoscopic surgery with scheduled follow-ups to monitor for recurrence, which has been shown to occur within the first 5 years after surgery and up to 12 years after initial excision. Most patients with glomangiopericytoma have a higher survival rate and low rates of metastasis, but they should be closely monitored due to the potential for significant symptoms. The CTNNB1 gene mutations and β-catenin nuclear expression have recently been identified as diagnostic markers in GPC. Glomangiopericytoma is a benign tumour with a high survival rate and a low rate of metastasis. Despite this favourable prognosis, further investigation is necessary to establish the relationship between surgical excision patterns and tumour recurrence rates. This case report highlights the importance of thorough diagnosis and management for these rare tumors.
Conflict of Interest
None of the authors have any conflict of interest to disclose.
Funding Sources
None
Disclaimer
All authors have seen and approved the manuscript, and contributed significantly to the work. The manuscript has not been previously published, nor is it being considered for publication elsewhere.
References
-
Stout AP, Murray MR (1942) Hemangiopericytoma a vascular tumor featuring zimmermannʼs pericytes. Ann Surg 116(1): 26-33.
-
Rabia B, Kara Y, Vayisoglu MD, Ozgur C, Anil O, et al. Sinonasal Glomangiopericytoma.
-
Kazi AA, McDougal EM, Howell JB, Schuman TA, Nord RS, et al. (2022) Glomangiopericytoma: a case series with review of literature. Braz J Otorhinolaryngol 88(5): 817- 820.
-
Ghaloo SK, Dhanani R, Pasha HA, Wasif M, Fatima S, et al. (2020) Glomangiopericytoma: A rare tumour of sinonasal cavity. J Pak Med Assoc 70(12): 2469-2471.
-
Saito Y, Ohta N, Konosu-Fukaya S, Shoji F, Suzuki T, et al. (2019) Endoscopic treatment of sinonasal Glomangiopericytoma: A case report in light of the literature. Yonago Acta Med 62(2): 236-239.
-
Agha RA, Franchi T, Sohrabi C, Mathew G, Kerwan A, et al. (2020) The SCARE 2020 guideline: Updating consensus surgical CAse REport (SCARE) guidelines. Int J Surg 84: 226-230.
-
Obeidin F, Jennings LJ, Alexiev BA (2019) Sinonasal glomangiopericytoma: A clinicopathologic study. Pathol Res Pract 215(5): 983-987.
-
Chaouki A, Najib Z, Mkhatri A, Rouadi S, Mahtar M, et al. (2021) Glomangiopericytoma of the inferior nasal turbinate: A case report. Int J Surg Case Rep 79: 409-412.
-
Nunnery EW, Kahn LB, Reddick RL, Lipper S (1981) Hemangiopericytoma: a light microscopic and ultrastructural study. Cancer 47(5): 906-914.
-
Min HJ, Kim KS (2019) Sinonasal Glomangiopericytoma: A Case Report and Literature Review. Banglad J Med Sci 18(3): 651-655.
-
Dandekar M, McHugh JB (2010) Sinonasal glomangiopericytoma: case report with emphasis on the differential diagnosis. Arch Pathol Lab Med 134(10): 1444-1449.
-
Zhang L, Li Z, Li Y, Li C, Li D, et al. (2016) Expression and significance of β-catenin, TCF-4 and survivin in glomangiopericytoma. Oncology Letters 12(6): 4453- 4460.
-
Chetty R, Jain R, Serra S (2007) Glomangiopericytoma: an unusual tumour of the larynx. J Clin Pathol 60(10): 1157-1159.
-
Cho WY, Kim HK, Choi JH, Lee JH, Kim MS, et al. (2016) Glomangiopericytoma in the nasal cavity: a case report. J Med Case Rep 10(1).
-
Folpe AL, Fanburg-Smith JC, Miettinen M, Weiss SW (2001) Atypical and malignant glomus tumors: analysis of 52 cases, with a proposal for the reclassification of glomus tumors. Am J Surg Pathol 25(1): 1-12.
-
Park ES, Kim J, Jun SY (2017) Characteristics and prognosis of glomangiopericytomas: A systematic review. Head Neck 39(9): 1897-1909.
- Hydrogen Peroxide Scavenging by Methanolic Extracts of Coriander: An In Vitro Antioxidant Study
- Aromatherapy in Palliative Care: A Fragrant Quest for Relief
- Empowering Women, Securing Futures: Contraception’s Role in Socioeconomic Progress in India
- Effect of Crospovidone, Croscaramellose Sodium in Combination on the Drug Release of Anti diabetic Medication in Tablet Form
- Knowledge, Attitudes, Anxiety, and Preventive Behaviors Regarding Covid-19 Affliction among Healthcare Workers in Pakistan
- “Competitive Landscape and Brand Equivalents: Implications for ANDA (Abbreviated New Drug Application) Approval”