Advances in the Preparation Techniques of Floating Microspheres with Exploration of AI Tool in Product Development
This review paper focuses on recent developments in gastroretentive drug delivery systems for controlled release oral drug administration. Gastric emptying’s variability presents challenges to drug delivery systems, making gastroretentive drug delivery systems increasingly popular for retaining drugs in the stomach and ensuring gradual release. Traditional oral delivery systems often fail to overcome gastrointestinal obstacles, resulting in incomplete drug release, decreased efficacy. Thus, achieving prolonged gastric residence times is crucial, particularly for drugs with upper small intestine absorption windows. Gastro retentive drug delivery system provide for prolonged drug release in the upper digestive system, improving bioavailability for drugs with narrow therapeutic windows, extending dosing intervals, and enhancing patient compliance. The purpose of this review is to discuss recent advancements in the preparation techniques for floating drug delivery systems and highlights the incorporation of AI-Enabled design and optimization in drug release behavior. These technologies enhance precision and efficiency in gastroretentive drug delivery systems development, promising further improvements in drug delivery effectiveness and patient adherence.
Introduction
The development of oral controlled-release (CR) dosage forms over the past three decades has been fueled by their therapeutic benefits, such as easy administration, patient compliance, and adaptability to formulation requirements [1]. However, these benefits are counterbalanced by physiological challenges, particularly the complex task of precisely controlling and detecting drug delivery systems inside the desired region of the GI tract (GIT). This is hindered by the variable nature of gastric emptying and motility. One of the challenges encountered involves effectively localizing the dosage form within the intended section of the gastrointestinal tract. Addressing this physiological hurdle has prompted exploration into numerous drug delivery systems designed to extend the duration of gastric retention (GRT) [2].
It offers a spectrum of therapeutic and biopharmaceutical benefits. These benefits include increased local drug action in the stomach, increased drug concentrations, improved patient adherence through dosage reduction, and increased bioavailability of medications with upper GIT absorption windows [3].
The dosage forms capable of sustained retention within the stomach are categorized as gastrointestinal drug delivery systems. Increases in drug bioavailability, a decrease in residual waste, and increased solubility for drugs with poor solubility in the high pH environment of the GIT are all benefits of prolonged stomach retention time. This has implications for the small intestines and stomach for targeted drugs delivery, offering new therapeutic application possibilities [4].
Achieving regulated retention of solid dosage forms within the stomach can be facilitated through various mechanisms. These encompass mucoadhesion, floatation, sedimentation, expansion and modified shape systems, and even the use of pharmacological agents capable of delaying gastric emptying (Figure 1). In light of these diverse approaches, it becomes evident that floating drug delivery systems stand out as a particularly promising avenue for the controlled release of drugs [5, 6, 7, 8].
In the creation of various intelligent drug release systems, critical considerations include the ability to adjust doses on demand, manage the rates of drug release, ensure targeted delivery, and maintain drug stability. When it comes to self-monitoring drug release systems, the application of appropriate algorithms becomes invaluable for precisely controlling both the quantity and duration of drug release. Consequently, the utilization of AI methodologies proves highly beneficial in forecasting the effectiveness of drug dosing and the drug delivery potential inherent in dosage forms for drug delivery this innovative approach harnesses AI algorithms and machine learning to analyze vast datasets, enabling the prediction of drug behavior under various conditions. Using simulations to test drug delivery and formulation, researchers can optimize these processes without having time-consuming trial-and-error experiments. This approach expedites drug development, lowers costs, and boosts overall productivity. Computational pharmaceutics operates across different scales, from molecular interactions to larger-scale behaviors, offering a comprehensive grasp of drug delivery mechanisms. AI aids in forecasting drug characteristics, release patterns, stability, and in vivo pharmacokinetics, facilitating proactive risk assessment and system refinement. Ultimately, AI minimizes the dependence on expensive experimentation and reduces the likelihood of unforeseen issues, making it an invaluable asset in modern drug delivery research [9, 10].

Basic GIT Physiology
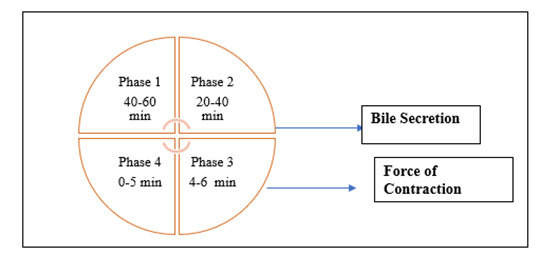
In anatomical terms, the stomach is partitioned into three distinct regions: the fundus, body, and antrum (pylorus). The fundus and proximal body function as reservoirs for non-digestible substances, while the antrum orchestrates a combination of movements, acting as a pump to facilitate gastric emptying through peristaltic action. Gastric emptying is observed during both fasting and feeding states; however, the dynamics differ significantly between these states. In the fasting state, recurring electrical events transpire every 2–3 hours, referred to as the Inter-Digestive Migrating Myoelectric Cycle (MMC).
- Basal Stage (Phase I): Lasting 40–60 minutes, this phase is characterized by sporadic contractions.
- Pre-Burst Phase (Phase II): Extending 40–60 minutes, this stage introduces action potentials and contractions, with their intensity and frequency progressively increasing.
- Burst Phase (Phase III): Spanning 4–6 minutes, this phase features short-lived, intense contractions, often termed the “housekeeper wave,” extending from the stomach to the small intestine.
- Transitional Phase (Phase IV): Occurring between cycles of Phase I and Phase III, this phase varies in duration from zero to five minutes, setting the stage for the ensuing cycle (Figure
Potential Drug Candidates for Gastro Retentive Drug Delivery System
- Some drugs have a limited window of absorption within the GI tract, like riboflavin and levodopa.
- Certain medications are primarily absorbed from the upper GI tract, including the stomach. Examples include calcium supplements, chlordiazepoxide, and cinnarizine.
- Some drugs exert their effects directly in the stomach, such as antacids and misoprostol.
- Drugs that degrade in the colon, like ranitidine HCl and metronidazole.
- Drugs which can disrupt the normal balance of colonic bacteria, like amoxicillin trihydrate.
- There are low-density formulations of dietary fiber that create buoyancy in gastric fluid.
- Drugs exhibit bio adhesion to the mucous lining of the abdomen.
- Slowing down the movement of the GI tract can affect drug absorption, either through co-administered drugs or additives [13].
Factors Influencing Gastric Retention
• Dosage characteristics encompassing density, dimensions, and structure.
- Food-related factors, including concurrent consumption, nutritional content, and meal frequency.
- Co-administration of medications with anticholinergic properties (e.g., atropine, propentheline), opioids (e.g., codeine), and prokinetic agents (e.g., metoclopramide, isapride).
- Biological influences like gender, posture, age, sleep patterns, body mass, physical activity, and underlying medical conditions (e.g., diabetes, Crohn’s disease) [14].
Approaches for Gastric Retention
Several methods were used to increase the gastric retention time (GRT) of the dosage forms (DF) in the stomach by applying a variety of concepts.
Floating System
Floating systems are characterized by their ability to float within the stomach’s contents due to their reduced density. This buoyancy enables them to remain above the gastric fluids. As a result, the system gradually releases its contents at a controlled pace, effectively prolonging the time it remains in the stomach. This approach leads to an extended gastroretention period and a consequent reduction in variations observed in plasma drug concentrations [15].
Bio-adhesive System
The bio/mucoadhesive approach functions as a strategy to enhance the duration of the drug delivery system within the stomach by adhering to the surface of gastric epithelial cells or interacting with mucins. The interaction between polymers and the mucous/epithelial surface can be categorized into three main groups [16].
- Moisture-driven flexibility.
- Bond-based cohesion.
- Receptor-triggered connection.
Swelling and Expanding System
In these systems, the dosage form causes swelling on contact of gastric fluids, increasing its size and thereby preventing its rapid passage through the pyloric sphincter. The swollen form remains in the stomach, allowing for prolonged drug release and absorption. These systems rely on the ability of certain polymers to swell and hold fluids, creating a gel-like mass that slows down the emptying process.
High Density System
High-density formulations involve incorporating inert heavy materials (e.g., zinc oxide, barium sulfate, iron powder) into the drug delivery system. These materials make the formulation’s bulk density higher, making it heavier than stomach contents. As a result, the system remains in the stomach for an extended period, releasing the drug gradually [17].
Ion Exchange Resins
Ion exchange resins are employed to carry bicarbonate and adhere to negatively charged drug residues. These beads, containing the drug, are enclosed in a semi-permeable membrane to counteract the rapid dissipation of carbon dioxide. Once in the stomach’s acidic environment, an exchange of ions between chlorides and bicarbonates takes place. This reaction releases CO2 into the membrane, forming a temporary layer of resin beads. This layer causes the beads to rise above the stomach’s contents [18].
Osmotic Regulated System
Osmotic regulated systems encompass a drug delivery mechanism with controlled osmotic pressure. It is housed in a sustainable capsule supported by an inflatable floating component. After ingestion, the capsule immediately disintegrates in the stomach, leaving behind the osmotically controlled drug delivery device. Within this device, an inflatable support contains a liquid that transforms into gas at body temperature, inflating the polymer bag.
Magnetic System
DFs have a tiny internal magnet that keeps them in the gastric region, and a magnet is put in the abdomen over the location of the stomach [19].
Disadvantages
- Accurate placement of the external magnet is required.
- Potential challenges with patient adherence.
- Limited adoption in clinical practice.
Floating Drug Delivery System (FDDS)
Floating drug delivery systems, often termed hydrodynamic balance systems, possess lower density than the stomach’s fluid, allowing them to stay within the stomach for prolonged periods without influencing gastric emptying rate. The drug is gradually released from the system at a controlled rate. This approach leads to better control over the duration of the system’s presence in the stomach and maintains desired plasma drug concentrations. These systems remain floatable above stomach contents, enabling slow drug release and extending intestinal storage time, thus reducing fluctuations in plasma drug concentrations [20].
Floating drug delivery systems (FDDS) can be categorized into two main types:
- Effervescent Systems
- Non-Effervescent Systems
Effervescent System
This approach employs carbonates like sodium bicarbonate to trigger the in-situ generation of carbon dioxide (CO2). Organic acids, such as citric and tartaric acids, expedite this reaction, reducing the dosage form’s density and enabling it to stay afloat in the stomach. This method is divided into two main classes:
Volatile Liquid/Vacuum Type
Inflatable System
It involves a retrievable system containing a chamber filled with volatile liquids that undergo evaporation at body temperature. Upon introduction into the stomach, the chamber inflates, causing the system to float. The inflatable chamber is constructed from bio erodible polymers, like polyvinyl alcohol (PVA) and polyethylene. As it floats in gastrointestinal fluid, the polymer slowly dissolves, releasing the drug. Eventually, the inflatable section collapses [21].
Intragastric Floating System
This system integrates a vacuum-filled chamber along with a microporous compartment acting as a drug reserve. It achieves buoyancy within the stomach [22].
Intragastric-Osmotically Controlled System
Osmotic control is achieved through a biodegradable capsule containing an inflatable floating support coupled with an osmotically controlled drug delivery device [23, 24].
Gas Generating System
Gas-generating systems are prepared using effervescent compounds using hydrophilic polymers.
Floating Capsules
These formulations entail drug encapsulation within hydrophilic polymers such as ethyl cellulose or Eudragit RS-100 using effervescent agents like sodium bicarbonate or calcium carbonate. Moursy NM, et al. [25] developed hydrodynamically balanced capsules incorporating nicardipine hydrochloride and hydrocolloids. As the capsule’s shell dissolves upon contact with gastric fluid and swells, a gel-like barrier forms, allowing it to float in the stomach juice for an extended duration [25].
Floating Pills
Multiple unit floating dosage forms are crafted using an outer layer of hydrophilic polymer and an inner layer containing an effervescent agent. Upon coming into contact with gastric fluid, the hydrophilic polymer layer swells and initially sinks, while the effervescent agent reacts with the stomach contents, releasing CO2 and causing the system to float [26]. Meka L, et al. [27] designed captopril multiple-unit minitabs using a gas formation approach to enhance GRT and overall drug bioavailability. A multi-layer coating strategy involving inner seal coat, sodium bicarbonate effervescent layer, and outer gas-entrapped polymeric membrane extended the release duration of the drug [27].
Floating Systems with Ion Exchange Resins
These systems aim to prolong GRT using ion exchange resins. They comprise beads containing a drug-resin complex loaded with bicarbonate ions. These beads are coated with hydrophilic polymers. Upon coming into contact with gastric fluid, CO2 gas is generated, enabling the beads to float Pujara ND, et al. [28] developed a floating system based on ion exchange resin, utilizing beads full of bicarbonate and a negatively charged drug bound to the resin. This system shown in vitro floating times exceeding 24 hours and demonstrated increased retention compared to conventional formulations when tested in the stomach [28].
Non-Effervescent Systems
Non-effervescent floating systems involve a mechanism where the drug interacts with gastric fluid, causing it to undergo swelling while retaining its original shape. The density of the drug remains below one, enabling it to stay afloat within the gastric juice. These systems utilize matrix- forming polymers, gel-forming agents, or hydrocolloids with swellable properties to achieve the desired floating effect.
Colloidal Gel Barrier Systems
The initial hydrodynamically balanced system, devised by Sheth and Tossounian in 1975, involves drug- containing gel compositions within hydrochloride capsules or tablets. These systems encompass high levels of gelling agents like Hydroxyethyl Cellulose (HECs), Hydroxypropyl Methylcellulose (HPMCs), N-Acetyl Carboxymethyl Cellulose (NACMC) and other polymers such as polycarbophil, polyacrylates, and polystyrene. Upon exposure to gastric fluid, these hydrocarbon systems hydrate, forming colloidal gel barriers around the gel surface. The trapped air in the swollen polymer reduces density, ensuring buoyancy within the drug formulations [29].
Microporous Compartment System
This technique entails encapsulating the drug reservoir within a microporous compartment. The reservoir’s peripheral walls are hermetically sealed to prevent direct contact with the gastric mucosal surface. The diffused air- filled floating chamber in the stomach remains above the gastric contents, enhancing drug delivery efficiency. Gastric fluid enters via the pores, dissolving the drug, and facilitating continuous transport to the intestine for absorption.
Alginate Beads
Floating dosage forms, made from freeze-dried calcium alginate, are crafted into spherical beads around 2.5 mm in diameter. Sodium alginate solution is left in an aqueous solution of calcium chloride, resulting in precipitation of calcium alginate. These beads are solidified in liquid nitrogen and subsequently freeze-dried for about 24 hours at 40°C. This process forms a porous structure that can maintain buoyancy for over 12 hours.
Hollow Microsphere
Hollow microspheres are regarded as highly promising buoyant systems because of their distinct benefits of being a multi-unit system with favorable flow characteristics.
The common methods used to create these microspheres involve uncomplicated procedures like solvent evaporation or solvent diffusion followed by evaporation. Polycarbonate, cellulose acetate, and calcium alginate are some types of polymers employed in crafting these hollow microspheres. The buoyancy of the system and the release of drugs from the dosage form are influenced by factors such as the quantity of polymers utilized, the ratio of plasticizer to polymer, and the specific solvent employed in the formulation. Microspheres are created by gradually introducing a drug-containing emulsion into a volatile solvent. As the solvent undergoes evaporation, gas forms within dispersed polymer droplets, creating an internal cavity within the microsphere. This process is also known as the emulsion solvent diffusion method. The floating duration of these microspheres is influenced by the type and quantity of polymer incorporated in the formulation [30].
Advantage of Floating Microsphere
Floating Drug Delivery System is advantageous for drugs meant for local action in the stomach.
- Enhanced bioavailability.
- Improved first-pass biotransformation.
- Sustained drug delivery, reducing dosing frequency.
- Targeted therapy for upper gastrointestinal ailments.
- Minimized fluctuations in drug concentration.
- Enhanced receptor activation selectivity.
- Reduced body counter-activity.
- Prolonged time over critical drug concentration.
- Site-specific drug delivery.
- Minimized adverse effects in the colon.
- Reduced concentration-dependent adverse effects.
- Flexibility in drug formulation design.
Disadvantage of Floating Microsphere
- These systems are not appropriate for drugs with solubility or stability issues inside the gastrointestinal tract (GIT).
- For instance, drugs like nifedipine, which are well- absorbed throughout the GIT and subject to initial metabolism, might not be a preferred choice
- Drugs that cause irritation to the stomach lining are also unsuitable candidates
- Compounds that are sensitive to stomach acidity and may undergo degradation in the acidic stomach environment should not be considered for incorporation into this system
- Administering the dosage form with a full glass of water (approximately 200–250 ml) is recommended.
- These systems do not provide added advantages compared to conventional dosage forms for drugs that are absorbed effectively within the GIT [31, 32].
Method of Preparation of Hollow Microsphere
The following methods are employed for the preparation of a floating microsphere drug delivery system.
- Emulsion solvent evaporation technique
- Emulsion cross-linking technique
- Emulsion-solvent diffusion technique
- Emulsification heat stabilizing technique
- Multiple emulsion methods
- Coacervation phase separation technique
- Spray drying technique.
- Polymerization technique
- Ionic gelation technique
- Hydroxyl appetite (HAP) microspheres in sphere morphology
- Hot melt microencapsulation technique
Emulsion Solvent Evaporation Technique
The polymer used for coating was dissolved in an organic solvent that was not compatible with the liquid used for production. The primary substance (which could be soluble or insoluble in water) was dissolved or dispersed within the coating phase through agitation. This solution was then applied onto the liquid production phase to create microcapsules of the desired size. When the mixture was heated to eliminate the solvent, the polymer contracted around the central core. Scenarios in which core material’s coating dissolved in the polymer solution, the resulting microcapsules belonged to the matrix type [33]. This method had already been performed. As shown in Figure 3. A similar method was developed by Mateović-Rojnik T, et al. [34] using an acetone/liquid paraffin solvent system through emulsification and solvent evaporation. This approach highlights the importance of temperature in influencing physicochemical properties of microspheres. Elevated temperatures expedited solvent removal by reducing inner- phase solvent viscosity and increasing total permeability. Higher temperatures also led to quicker hardening of emulsion droplets, preventing stirrer shear forces from affecting them. At 40°C, solvent removal occurred rapidly, resulting in a high particle distribution. Conversely, lower temperatures allowed for more thorough emulsification, yielding uniformly sized, small droplets [34]. Kumar S, et al. [35] have investigated the effect of solvent ratio on the preparation of rosuvastatin floating microspheres by this method using ethyl cellulose as the polymer and dichloromethane and methanol as the organic solvents. The solvent ratio, ranging from 1:1 to 2:1, had a significant impact on microsphere characteristics. A 1:1 solvent ratio produced the smallest and most uniform microspheres with the highest buoyancy. Conversely, a 2:1 solvent ratio resulted in larger, irregular microspheres with lower buoyancy. The authors determined that the optimal solvent ratio for preparing buoyant rosuvastatin microspheres was 1:1, yielding small, uniform, and buoyant microspheres [35].
![Figure 3: A similar method was developed by Mateović-Rojnik T, et al. [34] using an acetone/liquid paraffin solvent system through emulsification and solvent evaporation. This approach highlights the importance of temperature in influencing physicochemical properties of microspheres. Elevated temperatures expedited solvent removal by reducing inner- phase solvent viscosity and increasing total permeability. Higher temperatures also led to quicker hardening of emulsion droplets, preventing stirrer shear forces from affecting them. At 40°C, solvent removal occurred rapidly, resulting in a high particle distribution. Conversely, lower temperatures allowed for more thorough emulsification, yielding uniformly sized, small droplets [34]. Kumar S, et al. [35] have investigated the effect of solvent ratio on the preparation of rosuvastatin floating microspheres by this method using ethyl cellulose as the polymer and dichloromethane and methanol as the organic solvents. The solvent ratio, ranging from 1:1 to 2:1, had a significant impact on microsphere characteristics. A 1:1 solvent ratio produced the smallest and most uniform microspheres with the highest buoyancy. Conversely, a 2:1 solvent ratio resulted in larger, irregular microspheres with lower buoyancy. The authors determined that the optimal solvent ratio for preparing buoyant rosuvastatin microspheres was 1:1, yielding small, uniform, and buoyant microspheres [35].](/fulltextimages/11263/fig_3.png)
Emulsion Cross-Linking Technique
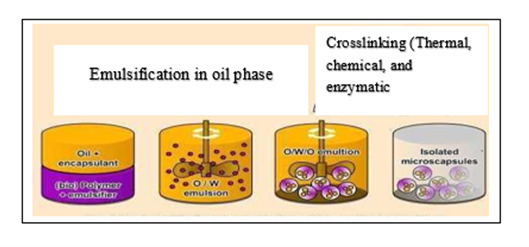
The emulsion crosslinking method for encapsulation involved creating water-in-oil (W/O) emulsions by combining coating solutions with crosslinking agents. This process was used to form microcapsules with controlled particle sizes. Initially, the main ingredient was emulsified with a coating solution and added to the oil phase, resulting in oil-in- water-in-oil (O/W/O) emulsions. Crosslinking agents were then added dropwise to harden the coating layer, and the continuous phase could consist of various combinations of paraffin, petroleum ether, or vegetable oils such as corn oil, sunflower oil, soybean oil, cottonseed oil, or sesame oil.
Using vegetable oil as the continuous phase was advantageous due to its safety, non-toxicity, and inherent stability, often without requiring additional surfactants.
An example of this technique was demonstrated by Jayanudin J, et al. [36] who encapsulated red ginger oleoresin using chitosan coating in corn oil as the continuous phase. The process involved dispersing red ginger oleoresin in chitosan solution to make an emulsion, which was then combined with corn oil to create a second emulsion. Glutaraldehyde saturated toluene (GST) was introduced dropwise along with a 25% (v/v) glutaraldehyde solution. This method allowed for effective encapsulation with specific core and coating materials [36].
Emulsion-Solvent Diffusion Technique
Kawashima Y, et al. [37] has proposed a method where Polyvinylalcohol-120-containing water was given a medication solution, and the mixture was agitated at 300 rpm. Solvent diffusion caused the drug solution droplets to solidify in the aqueous phase. The hardened droplets of dichloromethane evaporated, leaving a hole filled with water. The microspheres were further filtered, cleaned, and dried for two hours at 40 or 120°C. The Microballoons were created when the drying process left a hollow cavity inside the microsphere [37]. Rohilla S, et al. [38] have investigated how stirring speed affects particle size using a similar method for preparation of hollow microspheres. At low stirring speeds, the polymer coalesced and aggregated to form tougher globules, whereas at higher speeds, the microspheres broke down to form irregular particles. The solvent diffuses intermittently across the aqueous phase at 40 °C, giving enough time for the production of droplets and the hardening of hollow microspheres. The longer the stirring period, the more time the solvent will have to diffuse, improving yield. For this study, they discovered that a stirring rate of 350 rpm, a stirring time of 2 h, and a system temperature of 40 °C were the ideal circumstances for hollow microspheres preparation [38].
Emulsification Heat Stabilizing Technique
BSA microspheres encapsulating propranolol Hydrochloride were produced through an emulsion-heat stabilization method. A 5% BSA solution containing 0.1% Tween 80 was combined with 4% propranolol Hydrochloride. The oil phase, comprising 30 ml maize oil, 10 ml petroleum ether, and 1% Span 80, was mixed, followed by the gradual addition of the aqueous phase to form an initial emulsion. This mixture was then added into preheated maize oil, resulting in microspheres that were later purified, vacuum dried, and stored. The microspheres had diameters of 1-25 μm, with over 50% of them being smaller than 5 μm. The
encapsulated drug accounted for about 9% w/w of the initial quantity, and surface drug was 25% of the total encapsulated amount [39].
Single Emulsion Method
The microspheres composed of a natural polymer were generated using the single emulsion method. Initially, the natural polymers were dispersed in water and then distributed in a non-aqueous substance like oil. Subsequently, the dispersed droplets underwent cross-linking either by utilizing a chemical cross-linking agent or through the application of heat. Glutaraldehyde and formaldehyde are examples of chemical agents employed for cross-linking purposes [40, 41, 42].
Multiple Emulsion Method
The double-emulsion solvent diffusion method is notably recognized for encapsulating water-soluble drugs within water-insoluble polymers, which is crucial for controlled drug delivery. This technique ensures high entrapment efficiency by employing a hydrophobic processing medium, preventing the migration of hydrophilic drug molecules. While microencapsulation approaches have been widely utilized for lipophilic drugs, this method addressed the challenge of low loading efficiency seen with hydrophilic drugs (Figure 4) [43].
Coacervation Phase Separation Technique
The technique coacervation phase separation involves a systematic progression characterized by the ensuing sequential steps:
- Dispersal and Coating: The core material is dissolved in a solution of coating polymer.
- Coating Process: The coating is achieved by regulated physical mixing of the coating solution and core material within the liquid manufacturing vehicle phase.
- Coating Solidification: The coating polymer is solidified using various methods.
Thermal Change: The polymer is dissolved in cyclohexane with stirring at 80°C. The drug is added, and the temperature is reduced by placing it in an ice bath to obtain microspheres. The product is washed with cyclohexane and air-dried.
Non-Solvent Addition: The polymer is dispersed in toluene with polyisobutylene, shaken for 6 hours, and then the drug is added. The resulting solution is added to benzene with continuous stirring. The microcapsules are washed with n-hexane and air-dried.
Polymer Addition: Microspheres were formed by dispersing polymer (ethyl cellulose) in toluene, adding methylene blue as the core material. Coacervation is achieved by adding liquid polybutadiene. Strengthening the polymer coating is done by adding a non-solvent (hexane). The resulting product is washed and air-dried.
Salt Addition: An oil-soluble vitamin in corn oil is combined with a gelatin solution at 50°C. Coacervation is induced by adding sodium sulfate, resulting in a uniform gelatin coating. The microspheres are collected, washed, cooled, and dried.
Polymer-Polymer Interaction: A homogeneous polymer solution is prepared by mixing equal amounts of aqueous gum Arabic and gelatin solutions. The mixture is diluted and adjusted to pH 4.5, then heated to 40–45°C. Coacervation occurs due to interactions between the oppositely charged macromolecules. The liquid core material is added, mixed well while maintaining warmth, and then the mixture is cooled to 25°C. Further cooling to 10°C solidifies the coating [44, 45].
Spray Drying Technique
This method was employed to fabricate microspheres composed of polymer blends containing ketoprofen as the medication. The process involves dispersing the core material into a liquid coating substance, spraying this mixture externally, allowing the coating to solidify, and then rapidly evaporating the solvent. For the formulation of drug-loaded microspheres, a solution containing poly(epsilon caprolactone), cellulose acetate butyrate (CAB), and ketoprofen was created and sprayed under distinct experimental conditions. While this technique is efficient, the rapid drying process could potentially lead to the loss of crystallinity [46].
Polymerization Technique: Polymerization techniques are primarily categorized into two methods:
- Normal polymerization
- Interfacial polymerization.
Normal polymerization can be further divided into:
- Bulk polymerization.
- Suspension/pearl polymerization,
- Emulsion polymerization.
Bulk Polymerization: It involves heating monomers along with initiators or catalysts, allowing simultaneous drug loading; however, it’s not suitable for thermolabile drugs.
Suspension or Pearl Polymerization: It involves heating a monomer mixture at lower temperatures, dispersing drug- loaded droplets in an aqueous phase to create microspheres. Emulsion polymerization occurs in the presence of an initiator in the aqueous phase, yielding high polymer formation.
Interfacial Polymerization: This involves two immersed liquid phases of reactive monomers in, creates a polymer film covering the dispersed phase; it’s a process that employs different monomers dissolved or dispersed in distinct phases to create the polymer film [47, 48].
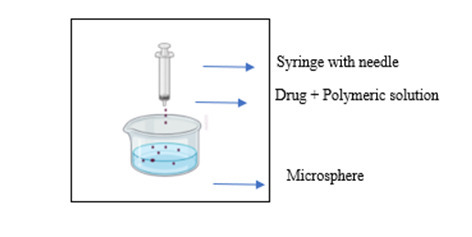
Ionic Gelation Technique
In this technique, the polyelectrolyte cross-links with counter ions to form a gel matrix. This method is often used to encapsulate a wide range of drugs. Polyelectrolytes like sodium alginate, known for their ability to coat the drug core and slow down release, contain specific anions in their chemical structure. These anions create a meshwork structure when they bind with polyvalent cations, leading to gel formation. To prepare microspheres, a solution loaded with the drug and polymer is dripped from a syringe into an aqueous solution containing polyvalent cations (Figure 5) [49].
Hydroxyl Appetite (HAP) Microspheres in Sphere Morphology
This approach was utilized to generate microspheres exhibiting unique spherical shapes. The process involved forming an oil in the water (o/w) emulsion followed by solvent evaporation. The organic phase was initially dispersed within the aqueous surfactant phase, creating an o/w emulsion where tiny droplets were enveloped by surfactant molecules, preventing their merging. Through gentle stirring, the solvent DCM was allowed to evaporate, causing the individual droplets to solidify independently and ultimately form microspheres [50].
Hot Melt Microencapsulation Technique
This method holds significant value due to its comparative analysis of indomethacin microparticles with different coatings, chitosan, and gelatin, produced through the hot-melt encapsulation technique using poly (epsilon- caprolactone) (PCL). The study’s findings highlight the reproducibility of the method in terms of yield and size distribution, essential in pharmaceutical applications. The method’s ability to control drug release kinetics, as demonstrated by the distinct release phases observed in both coated and uncoated microparticles, offers valuable insights for designing controlled drug delivery systems. Additionally, the utilization of natural coating materials like chitosan and gelatin provides a practical approach to mitigating burst release, a common challenge in drug delivery, while maintaining the sustained release phase unaffected. This contributes to the advancement of drug delivery strategies by potentially enhancing therapeutic outcomes and reducing side effects.
AI-Enabled Design and Optimization in Drug Release
Artificial intelligence (AI) is revolutionizing the production of floating microspheres, introducing a new era of precision in pharmaceutical formulation. AI’s advanced algorithms and predictive capabilities enable researchers to tailor microsphere properties with unmatched accuracy. From selecting optimal materials and designing controlled- release mechanisms to predicting in vivo behavior, AI-driven approaches promise to significantly enhance the efficiency of drug delivery systems, especially in scenarios where floating microspheres play a crucial role.
In the following study Artificial neural networks (ANNs) are a type of machine learning algorithm used to model complex relationships between variables. The in vitro aspirin release pattern from alginate-based floating microspheres was predicted using ANNs. The findings revealed that ANNs were more accurate than RSM, a traditional statistical method, in predicting the release profile. This suggests that ANNs could be used to design more effective floating microspheres for drug delivery. Multivariate methods which are statistical techniques that can be used to analyze the relationships between multiple variables both ANNs and factorial models were used to analyze the effects of three factors (external phase pH, initial loading of verapamil Hydrochloride, and concentration of polymer) on the properties of verapamil Hydrochloride microspheres. The results showed that ANNs were better at predicting the properties of the microspheres than the factorial model. This suggests that ANNs could be used to optimize the formulation of floating microspheres [51].
Galata DL, et al. [52] the researchers conducted an assessment of three AI algorithms to predict the dissolving characteristics of hydrophilic matrix sustained-release tablets. The study involved data analysis and forecasting of dissolution profiles using Artificial Neural Networks (ANN), an Ensemble of Regression Trees, and Support Vector Machines (SVM).
Furthermore, the study incorporated data from Process Analytical Technology (PAT) and Critical Material Attributes (CMAs) as input information to establish a database for modeling purposes. Notably, the Particle Size Distribution (PSD) emerged as a crucial factor influencing the accuracy of the predictive model. The evaluation of these models indicated that among all the algorithms considered, the Artificial Neural Network (ANN) demonstrated the highest level of accuracy in predicting the tablet dissolution characteristics [52].
Petrović J, et al. [53] assessed the estimation of drug release in matrix tablets through the use of different modeling techniques, including an Elman dynamic neural network, decision trees, and multilayer perceptrons. These models were applied to various types of tablet matrices containing either polyethylene oxide polymer or glyceryl palmitostearate, which were formulated under different compression forces. The input variables considered in the study encompassed the Critical Material Attributes (CMAs) and other tablet properties such as tensile strength and porosity. To optimize the neural networks, Monte Carlo was employed as an optimizer, and the models’ accuracy was evaluated by calculating the difference (f1) and similarity (f2) metrics. The study’s findings revealed that among the models tested, the Elman dynamic neural network, as a subset of Recurrent Neural Networks (RNN), performed the most effectively and delivered precise predictions regarding drug release. Table 1 presents a comprehensive list of commonly explored AI models in pharmaceutical product development [53].
| Al Machine Learning Models | Description/ Usage |
|---|---|
| Genetic Algorithms | Genetic algorithms are optimization methods that draw inspiration from the mechanisms of natural selection and genetics. These algorithms find application in optimizing various aspects of pharmaceuticals, including the composition of formulations, the profiles for drug release, and the parameters of manufacturing processes, all with the goal of attaining specific characteristics in dosage forms [54]. |
| Artificial Neural Networks (ANNs) | Artificial neural networks (ANNs) have been utilized to both model and enhance the kinetics of drug release via diverse types of dosage forms. They play crucial role in identifying the most effective formulations and forecasting the release patterns of active pharmaceutical ingredients (APIs) across various scenarios and conditions [55]. |
| Support Vector Machines (SVMs) | SVMs have found application in the optimization of dosage forms by predicting and modeling connections between formulation variables. These variables encompass factors like the composition of excipients, processing parameters, and the profiles of drug release. SVMs contribute to the enhancement of formulation design possibilities [56]. |
| Particle Swarm Optimization (PSO) | PSO is an optimization technique that operates at the population level and has been employed in the optimization of dosage forms. It has been utilized to enhance various aspects of pharmaceutical formulations, including the distribution of particle sizes, dissolution profiles, and other critical formulation parameters [57]. |
| Artificial Intelligence-based Expert Systems | Expert systems employ artificial intelligence techniques, such as rule-based systems and fuzzy logic, to emulate the decision-making processes of human experts. They find application in the optimization of dosage forms by systematically considering a wide array of formulation and process variables [58]. |
| Monte Carlo Simulation | The techniques Monte Carlo simulation have been instrumental in the optimization of drug product performance. These methods take into account the presence of uncertainties and variations in formulation and process parameters, ultimately contributing in the development of resilient and effective formulation and process designs [59]. |
| Computational Fluid Dynamics (CFO) | CFO simulations facilitate the optimization of fluid flow and mixing in the manufacturing processes of dosage forms, including granulation, coating, and drying. These simulations are instrumental in the creation of efficient and uniform manufacturing processes [60]. |
| Response Surface Methodology (RSM) | It is an statistical approach employed to enhance the optimization of dosage form formulations. It achieves this by creating models and conducting analyses to examine the intricate relationship between various variables and their impact on the responses of the formulation. RSM plays a crucial role in both comprehending and optimizing the parameters involved in formulation development [61]. |
| Artificial Neural Network- Genetic Algorithm (ANN-GA) Hybrid Models | In the realm of dosage form optimization, hybrid models that merge Artificial Neural Networks (ANN) with Genetic Algorithms (GA) have been applied. These hybrid models prove effective in navigating the expansive formulation space to pinpoint optimal solutions and anticipate the characteristics of the formulation with precision [62]. |
| Multivariate Analysis Techniques | Multivariate analysis techniques, including Principal Component Analysis (PCA) and Partial Least Squares (PLS), have found utility in the realm of dosage form optimization. These methods assist in the identification of crucial formulation variables, dimensionality reduction, and the enhancement of formulation performance [63]. |
Table 1: List of commonly explored Al models in pharmaceutical product development.
Evaluation of Floating Microsphere
Particle Size
Pandey N, et al. [64] has used Optical microscopy was used to determine the microspheres’ size and form of the particles. The size of each microsphere was determined using a stage micrometer and an ocular micrometer that had been previously calibrated while the microspheres were being inspected under a microscope. Each mixture produced about 100 microspheres, which were counted and quantified. It is already known that when microspheres are smaller than 500
nm, the floating ability is lowered, and the drug release rate is higher [64].
Percent Compressibility index
The Compressibility index (CI) is significant because it has an impact on how the microspheres float. In gastric juices, microspheres with a high CI are more likely to sink whereas those with a low CI are more likely to float. This is because the high CI microspheres sink more readily since they may be compressed more readily.
– 100 b b ρ ρ ρ × t where t ρ is the tapped bulk density and ñb is the initial bulk density [65].
Percent Yield
Percent yield represented the proportion of the intended microspheres that are successfully produced in relation to the theoretical maximum amount. The yield was calculated by the following equation.
% 100 weight of hollowmicrosphere yield weightof drug taken total polymer weight = × +
Drug Entrapment Efficiency
The amount of drug entrapped in the microspheres was calculated by a method called drug encapsulation efficiency. This procedure entails breaking up the microspheres and extracting the medication using a 0.1N HCl solution. The extracted drug is then measured using a spectrophotometer, and the amount of drug entrapped in the microspheres is calculated using the following formula [66].
100 Actual drug content Entrapment efficiency Therotical drug content = ×
Swelling Study
The assessment of a dosage form’s swelling characteristics can be measured by examining either its increase in weight or its absorption of water. This measurement is typically expressed in percentage increase in weight.
In- Vitro Release Studies
Pandya N, et al. [67] has studied the released rate of glipizide from floating microspheres was determined in a USP basket-type dissolution apparatus. The microspheres were placed in a hard gelatine capsule and immersed in 500 mL of simulated gastric fluid (SGF) containing 0.02% w/v of Tween 20. The dissolution fluid was kept at 37ºC ± 1ºC at a rotation speed of 100 rpm. Samples were extracted at 30 min intervals, filtered, and analyzed spectrophotometrically to determine the concentration of glipizide in the dissolution medium. The initial volume of the dissolution medium was sustained by introducing 5 mL of new dissolution medium following each withdrawal. All experiments were conducted in triplicate [67].
Parikh RK, et al. [68] highlighted a significant challenge in the dissolution testing of Gastro-Retentive Drug Formulations (GRDFs) when used with particularly weak basic drugs, which pertains to pH variations inside the gastrointestinal tract (GIT). To address this issue, they devised a complex multi-compartment transfer model utilizing the Rosette-Rice apparatus. This model comprises three compartments: gastric, intestinal, and absorption compartments. Within this apparatus, the drug can move freely from the gastric to the intestinal compartment, with a filter membrane separating the absorption and intestinal compartments. Additionally, it is possible to modify the pH levels of the adjacent environment by employing reservoirs that hold either 1 N hydrochloric acid (HCl) or borate buffer solutions. This innovative in-vitro system demonstrated potential advantages when evaluating controlled-release floating systems in comparison to conventional immediate- release tablets [68].
Eberle VA, et al. [69] proposed a concept they termed a “custom-built stomach model,” which aimed to address certain issues in drug formulation testing. In this setup, their objective was to attach the drug formulation (DF) to the paddle shaft, preventing constant exposure to air. The system consisted of Erlenmeyer flasks, each containing 400 ml of a solution, securely positioned within a water-bath shaker . Overall, this unique configuration demonstrated a more noticeable release rate for the drug in a test floating system when compared to a conventional USP II paddle equipment setup. Nevertheless, it’s important to consider that in the paddle system, the drug formulation could freely float on the surface of the medium [69]. In this region, the shear stress is minimal, providing valuable insights into the obtained results. It should be noted, however, that this artificial setup may yield more informative measurements but might not accurately reflect in-vivo behavior due to its limited physiological relevance [70, 71].
In-Vivo Studies
Klausner EA, et al. [72] introduced an innovative controlled-release gastroretentive drug delivery system (GRDDS) for Levodopa, utilizing extended and rigid polymeric membranes. On beagle dogs were administered by carbidopa and in vivo tests were carried out. After administering the drug’s formulation, X-ray imaging revealed that it was located in the gastrointestinal tract. Blood samples taken later were used to gauge drug levels in use. The optimized Levodopa GRDDS maintained sustained therapeutic levels (>500 ng/ ml) for more than 9 hours. This absorption time was much longer than that of oral solutions and non-GR controlled- release particles [72].
In the following study by Jain SK, et al. [73] they developed floating microspheres containing repaglinide, a hypoglycemic agent. These microspheres used Eudragit as a polymer and calcium silicate as a porous carrier. The stomach residence duration was determined using gamma scintigraphy after 6 hours utilizing organ distribution tests on Sprague-Dawley male rats and 99mTc-labeled floating microspheres given orally to albino rabbits. The abdomen and intestinal parts of the sacrificed animal were separated from the organs. The test substance had a consistent organ distribution, and its related bioavailability was 3.17 times greater than that of commercial tablets [73].
Human Study
Ranade AN, et al. [74] conducted a study in which they examined the use of ellagic acid and aloe vera gel powder in the form of bilayer floating tablets. These tablets were formulated by incorporating HPMC K15M and sodium bicarbonate with the aim of treating stomach ulcers. The researchers observed that these tablets demonstrated reduction up to 75% in ulcer development, which was significantly higher compared to the 57% ulcer inhibition achieved when ellagic acid was used alone. Notably, this improved effectiveness was achieved despite the tablets exhibiting a cumulative drug release of only 92% over a 4-hour period in the floating environment [74].
Application of Floating Microsphere
Sustained Drug Delivery These specialized systems can stay in the stomach for prolonged periods, gradually releasing drugs over time. They solve the issue of limited time drugs spend in the stomach along with the conventional controlled-release formulations. Their low density allows them to float on stomach contents, and their larger size prevents them from passing through the pyloric opening.
Specific Drug Delivery These systems are especially useful for drugs absorbed primarily from the stomach or the upper section of the small intestine. For instance, compounds like riboflavin and furosemide. Floating microspheres improved controlled release of drug in specific area resulting to increased drug concentrations in the stomach lining. This approach can help treat conditions like ulcers, gastritis, and esophagitis by targeting Helicobacter pylori in the submucosal tissue.
Enhanced Absorption Floating microspheres effectively used in delivering poorly soluble drugs. When a drug’s solubility decreases, the time available for it to dissolve becomes limited, impacting absorption. Hollow microspheres, especially for weakly basic drugs with low solubility in an alkaline environment, can prevent solubility from becoming the limiting factor in release. This approach benefits drugs efficiently absorbed through the stomach, like Verapamil hydrochloride, by modifying absorption profiles to enhance bioavailability.
As Carriers Floating multiarticulate systems can act as carriers for drugs targeted at particular absorption sites, such as antiviral, antifungal, and antibiotic agents like Sulphonamides, Quinolones, Penicillin’s, and more. These drugs are selectively taken up from certain regions of the gastrointestinal mucosa [75].
Vaccination Floating microspheres have the potential to act as carriers for vaccines or immunotherapeutic agents, facilitating controlled release and precise delivery to specific parts of the gastrointestinal tract or mucosal surfaces. This enhances the immune response.
Treatment of Inflammatory Bowel Disease (IBD) Floating microspheres can be utilized to administer anti-inflammatory medications to the affected regions of the gastrointestinal tract in individuals with conditions such as Crohn’s disease or ulcerative colitis. This approach may help in minimizing the side effects often linked with systemic drug administration.
Diagnostic Imaging Microspheres can be filled with contrast agents or imaging agents to enhance diagnostic imaging techniques like MRI or CT scans. These microspheres can be engineered to remain in specific regions of the digestive tract for improved imaging of gastrointestinal diseases.
Conclusion
In summary, floating microspheres are a promising new drug delivery system that can improve the gastric residence time of drugs. They can be employed for targeted drug delivery within distinct segments of the gastrointestinal tract, to reduce the side effects of drugs, and to treat a variety of conditions. It highlights recent advancements in floating microsphere preparation techniques and emphasizing the incorporation of AI-Enabled design and optimization in the drug delivery systems which facilitate the development of groundbreaking controlled and delayed release formulations for gastrointestinal use, thereby pushing the boundaries of pharmaceutical research and development.
Author Contribution
O. A. Kulkarni, Author Contributed for Data arrangement in this review article.
Dr. (Mrs.) D. A. Bansode, Corresponding Author contributed for data arrangement and outlook on whole review article.
Conflicts of Interest
There is no conflict to declare.
Acknowledgements
We are expressing gratitude towards Poona College of Pharmacy for this opportunity and providing all the necessary data sources required for this review article.
References
-
Awasthi R, Kulkarni GT (2016) Decades of research in drug targeting to the upper gastrointestinal tract using gastroretention technologies: where do we stand? Drug Deliv 23(2): 378-394.
-
Hafeez A, Maurya A, Singh J, Mittal A, Rana L, et al. (2013) An overview on floating microsphere: Gastro Retention Floating drug delivery system (FDDS). J phytopharm 2(3): 1-12.
-
Reinholz J, Landfester K, Mailänder V (2018) The challenges of oral drug delivery via nanocarriers. Drug Deliv 25(1): 1694-1705.
-
Davis SS (2005) Formulation strategies for absorption windows. Drug Discov Today 10(4): 249-257.
-
Patel JK, Patel RP, Amin AF, Patel MM (2005) Formulation and evaluation of mucoadhesive glipizide microspheres. AAps PharmSciTech 6(1): E49-E55.
-
Khanage SG, Ptil VR (2017) Formulation and evaluation of Carisoprodol microsphere for sustained drug delivery. Caribb J Sci 5(1): 51-64.
-
Gupta RI, Prajapati SK, Pattnaik SN, Ganguli A, Mishra S, et al. (2012) Performance and evaluation of floating microspheres of famotidine and comparison of their physical properties. Int J Pharm Pharm Sci 4(5): 376- 382.
-
Bhavsar DN (2012) Advances in GRDDS: Raft forming system a review. Drug Deliv Therap 2(5): 123-128.
-
Vora LK, Gholap AD, Jetha K, Thakur RR, Solanki HK, et al. (2023) Artificial Intelligence in Pharmaceutical Technology and Drug Delivery Design. Pharmaceutics 15(7): 1916.
-
Jiang J, Ma X, Ouyang D, Williams III RO (2022) Emerging artificial intelligence (ai) technologies used in the development of solid dosage forms. Pharmaceutics 14(11): 2257.
-
Wilding IR, Coupe AJ, Davis SS (2001) The role of γ-scintigraphy in oral drug delivery. Adv Drug Deliv Rev 46(1-3): 103-124.
-
Feinle C, Kunz P, Boesiger P, Fried M, Schwizer W, et al. (1999) Scintigraphic validation of a magnetic resonance imaging method to study gastric emptying of a solid meal in humans. Gut 44(1): 106-111.
-
Singh BN, Kim KH (2000) Floating drug delivery systems: an approach to oral controlled drug delivery via gastric retention. J Control Release 63(3): 235-259.
-
Kavitha S, Peeyush KM, Anil B, Akanksha G, Navneet G, et al. (2015) Floating Microsphere as Gastro retentive Drug Delivery Systems. A Review World J Pharm Res 4(3): 668-684.
-
Sarojini S, Manavalan R (2012) An overview on various approaches to gastroretentive dosage forms. Int J Drug Dev Res 4(1): 1-13.
-
Gholap SB, Banarjee SK, Gaikwad DD, Jadhav SL, Thorat RM, et al. (2010) Hollow microsphere: A Review. Int J Pharm Sci Rev Res 1(1): 74-79.
-
Gadge G, Sabale V, Khade A (2019) Current Approaches on Gastro Retentive Drug Delivery System: An Overview. Int J Pharm Technol (IJPRT) 9(2): 16-28.
-
Atyabi F, Sharma HL, Mohammad HA, Fell JT (1996) In vivo evaluation of a novel gastric retentive formulation based on ion exchange resins. J Control Release 42(2): 105-113.
-
Arora S, Ali J, Ahuja A, Khar RK, Baboota S, et al. (2005) Floating drug delivery systems: A Review. Aaps PharmSciTech 6(3): E372-E90.
-
Babu SS, Suresh P, Khalilullah S, Nama S, Brahmaiah B, et al. (2013) Gastroretentive drug delivery system a review. Int J Pharm Pract Drug Res 3: 26-31.
-
Garg RG, Gupta GD (2008) Progress in controlled gastroretentive delivery systems. Trop J Pharm Res 7(3): 1055-1066.
-
Thapa P, Jeong SH (2018) Effects of formulation and process variables on gastroretentive floating tablets with a high-dose soluble drug and experimental design approach. Pharmaceutics 10(3): 161.
-
Nayak AK, Malakar J, Sen KK (2010) Gastroretentive drug delivery technologies: Current approaches and future potential. J Pharm Educ Res 1(2): 1-12.
-
Zhao Z, Wu C, Zhao Y, Hao Y, Liu Y, et al. (2015) Development of an oral push–pull osmotic pump of fenofibrate-loaded mesoporous silica nanoparticles. Int J Nanomed 10: 1691-1701.
-
Moursy NM, Afifi NN, Ghorab DM, El-Saharty Y (2003) Formulation and evaluation of sustained release floating capsules of Nicardipine hydrochloride. Die Pharmazie- Int J Pharm Sci 58(1): 38-43.
-
Pal P, Sharma V, Singh L (2012) A review on floating type gastro retentive drug delivery system. Int Res J Pharm 3(4): 37-43.
-
Meka L, Kesavan B, Chinnala KM, Vobalaboina V, Yamsani MR, et al. (2008) Preparation of a matrix type multiple- unit gastro retentive floating drug delivery system for captopril based on gas formation technique: in vitro evaluation. AAPS PharmSciTech 9(2): 612.
-
Pujara ND, Gokani RK, Paun JS (2012) Bilayer tablet-an emerging trend. Int J Pharm Res Dev 4(4): 103-104.
-
Gareeb MM, Radhi ZA (2014) Formulation and In-Vitro Evaluation of Trimetazidine Dihydrochloride Floating Beads. Int J Pharm Pharm Sci 6(2): 456-460.
-
Jyothi NVN, Prasanna PM, Sakarkar SN, Prabha KS, Ramaiah PS, et al. (2010) Microencapsulation techniques, factors influencing encapsulation efficiency. J Microencapsul 27(3): 187-197.
-
Taneja R, Kataria MK, Bilandi A, Gupta A, Gedar S, et al. (2013) Floating microsphere: a potential gastroretentive drug delivery system. Pharm Glob 4(4): 1-9.
-
Dey NS, Majumdar S, Rao MEB (2008) Multiparticulate drug delivery systems for controlled release. Tropical journal of pharmaceutical research 7(3): 1067-1075.
-
Srivastava AK, Ridhurkar DN, Wadhwa S (2005) Floating microspheres of cimetidine: Formulation, characterization and in vitro evaluation. Acta Pharmaceutica 55(3): 277-285.
-
Mateović-Rojnik T, Bogataj M, Bukovec P, Mrhar A (2005) Effect of preparation temperature in solvent evaporation process on Eudragit RS microsphere properties. Chem Pharm Bull 53(1): 143-146.
-
Kumar S, Nagpal K, Singh SK, Mishra DN (2011) Improved bioavailability through floating microspheres of lovastatin. Daru J Fac Pharm Tehran Univ Med Sci 19(1): 57-64.
-
Jayanudin J, Heriyanto H (2021) A review of encapsulation using emulsion crosslinking method. World Chem Eng J 5(2): 37-43.
-
Kawashima Y, Niwa T, Takeuchi H, Hino T, Itoh Y, et al. (1992) Hollow microspheres for use as a floating controlled drug delivery system in the stomach. J Pharm Sci 81(2): 135-140.
-
Rohilla S, Bhatt DC, Ahalwat S (2019) Effect processing variables on the characteristics of itraconazole hollow microspheres. Int J App Pharm 11(6): 108-115.
-
Verma NK, Alam G, Vishwakarma DK, Mishra JN, Khan WU, et al. (2015) Recent Advances in Microspheres Technology for Drug Delivery. Int J Pharm Sci and Nanotechnology 8(2): 2799-2813.
-
Saxena A, Gaur K, Singh V, Singh RK, Dashora A, et al. (2014) Floating microspheres as drug delivery system. Am J Pharm Pharm Sci 1(2): 27-36.
-
Gurung BD, Kakar S (2020) An overview on microspheres. Int J Health Clin Res 3(1): 11-24.
-
Dhadde GS, Mali HS, Raut ID, Nitalikar MM, Bhutkar MA (2021) A review on microspheres: Types, method of preparation characterization and application. Asian J Pharm Technol 11(2): 149-155.
-
Jelvehgari M, Dastmalch S, Nazila D (2012) Theophylline ethylcellulose microparticles screening of the process and formulation variables for preparation of sustained release particles. Iran J Basic Med Sci 15(1): 608-624.
-
Sudheer P, Kumar H, Thomas L, Nethravathi DR (2015) Floating microspheres an excellent approach for gastric retention. J Pharm Res 14(4): 71-80.
-
Dandagi PM, Mastiholimath VS, Gadad AP, Iliger SR (2007) Mucoadhesive Microspheres of Propranolol Hydrochloride for Nasal Delivery. Indian J Pharm Sci 69(3): 402-407.
-
Joshi V, Velhal A, Patil S, Redasani V, Raut P, et al. (2023) An Overview on Novel Drug Delivery System of Microsphere and its Types Materials Method of Preparation. Asian J Pharm Res Dev 11(4): 106-114.
-
Phalguna Y, Venkateshwarlu BS, Gudas GK, Debnath S (2010) HPMC microspheres of zidovudine for sustained release. Int J Pharm Pharm Sci 2(4): 41-43.
-
Ware M, Tiwari SP, Roy A, Satapathy T, Jo D, et al. (2013) New insights into gastro retentive floating drug delivery systems. World J Pharma Sci 3(1): 252-270.
-
Saini S, Asija R, Goyal A (2022) Floating Microsphere as Gastro Retentive Drug Delivery System An Updated Review. Trop J Pharm Life Sci 9(2): 21-29.
-
Sam MT, Gayathri DS, Prasanth V, Vinod B (2008) NSAIDs as microspheres. Internet J Pharmacol 6(1): 1-8.
-
Das S, Dey R, Nayak AK (2021) Artificial intelligence in pharmacy. Indian J Pharm Educ Res 55(2): 304-318.
-
Galata DL, Könyves Z, Nagy B, Novák M, Mészáros LA, et al. (2021) Real time release testing of dissolution based on surrogate models developed by machine learning algorithms using NIR spectra compression force and particle size distribution as input data. Int J Pharm 597: 120338.
-
Petrović J, Ibrić S, Betz G, Đurić Z (2012) Optimization of matrix tablets controlled drug release using Elman dynamic neural networks and decision trees. Int J Pharm 428(1-2 ): 57-67.
-
Bannigan P, Aldeghi M, Bao Z, Häse F, Aspuru GA, et al. (2021) Machine learning directed drug formulation development. Adv Drug Deliv Rev 175: 113806.
-
Sun Y, Peng Y, Chen Y, Shukla AJ (2003) Application of Artificial Neural Networks in the Design of Controlled Release Drug Delivery Systems. Adv Drug Deliv Rev 55(9): 1201-1215.
-
Sengupta S, Basak S, Peters RA (2018) Particle Swarm Optimization A survey of historical and recent developments with hybridization perspectives. Mach Learn Knowl Extr 1(1): 157-191.
-
Mukhamediev RI, Popova Y, Kuchin Y, Zaitseva E, Kalimoldayev A, et al. (2022) Review of Artificial Intelligence and Machine Learning Technologies Classification Restrictions Opportunities and Challenges. Mathematics 10(15): 2552.
-
Paul D, Sanap G, Shenoy S, Kalyane D, Kalia K, et al. (2021) Artificial intelligence in drug discovery and development. Drug Discov Today 26(1): 80-93.
-
Eberle LG, Sugiyama H, Schmidt R (2014) Improving lead time of pharmaceutical production processes using Monte Carlo simulation. Comput Chem Eng 68: 255-263.
-
Böhling P, Khinast JG, Jajcevic D, Davies C, Carmody A, et al. (2019) Computational fluid dynamics discrete element method modeling of an industrial scale Wurster coater. J Pharm Sci 108(1): 538-550.
-
Mahapatra AP, Saraswat R, Botre M, Paul B, Prasad N (2020) Application of response surface methodology RSM in statistical optimization and pharmaceutical characterization of a patient compliance effervescent tablet formulation of an antiepileptic drug levetiracetam. Future J Pharm Sci 6: 1-4.
-
Kundu P, Paul V, Kumar V, Mishra IM (2015) Formulation development modeling and optimization of emulsification process using evolving RSM coupled hybrid ANN GA framework. Chem Eng Res Des 104: 773- 790.
-
Shi G, Lin L, Liu Y, Chen G, Luo Y, et al. (2021) Pharmaceutical application of multivariate modelling techniques a review on the manufacturing of tablets. RSC advances 11(14): 8323-8345.
-
Pandey N, Sah NA, Mahara K (2016) Formulation and evaluation of floating microspheres of nateglinide. Int J Pharma Sci Res 7(11): 453-464.
-
El KAH, Sokar MS, Al GSS, Naggar VF (2001) Preparation and evaluation of ketoprofen floating oral delivery system. Int J Pharm 220(1-2): 13-21.
-
Chainesh S, Chintan A, Vinod R, Nirmal S, Sachin C, et al. (2012) An Overview on Gastro Retentive Floating Microspheres. Int J Pharm Res Technol IJPRT 2(2): 1-8.
-
Pandya N, Pandya M, Bhaskar VH (2011) Preparation and in vitro characterization of porous carrier based glipizide floating microspheres for gastric delivery. J Young Pharmacists 3(2): 97-104.
-
Parikh RK, Parikh DC, Delvadia RR, Patel SM (2006) A novel multi compartment dissolution apparatus for evaluation of floating dosage form containing poorly soluble weakly basic drug. Dissolut Technol 13(1): 14- 19.
-
Eberle VA, Schoelkopf J, Gane PA, Alles R, Huwyler J, et al. (2014) Floating gastroretentive drug delivery systems Comparison of experimental and simulated dissolution profiles and floatation behavior. Eur J P harm Sci 58: 34- 43.
-
Saab M, Issa M, Samy W, El MH (2016) Alternative approaches in formulating floating hollow tablets via sublimation technique A platform tailored drug release profile. Int J Pharm Sci 71(12): 701-708.
-
Abouelatta SM, Aboelwafa AA, El GON (2018) Gastroretentive raft liquid delivery system as a new approach to release extension for carrier mediated drug. Drug Deliv 25(1): 1161-1174.
-
Klausner EA, Lavy E, Friedman M, Hoffman A (2003) Expandable gastroretentive dosage forms. J Control Release 90(2): 143-162.
-
Jain SK, Awasthi AM, Jain NK, Agrawal GP (2005) Calcium silicate based microspheres of repaglinide for gastroretentive floating drug delivery Preparation and in vitro characterization. J control Release 107(2): 300- 309.
-
Ranade AN, Ranpise NS, Ramesh C (2014) Exploring the potential of gastro retentive dosage form in the delivery of ellagic acid and aloe vera gel powder for the treatment of gastric ulcers. Curr Drug Deliv 11(2): 287-297.
-
Rani R, Kumar M, Yadav N, Bhatt S, Malik A, et al. (2020) Recent advances in the development of floating microspheres for the treatment of gastric ulcers. Int J Adv Sci Technol 29(5): 3613-3627.
- Hydrogen Peroxide Scavenging by Methanolic Extracts of Coriander: An In Vitro Antioxidant Study
- Aromatherapy in Palliative Care: A Fragrant Quest for Relief
- Empowering Women, Securing Futures: Contraception’s Role in Socioeconomic Progress in India
- Effect of Crospovidone, Croscaramellose Sodium in Combination on the Drug Release of Anti diabetic Medication in Tablet Form
- Knowledge, Attitudes, Anxiety, and Preventive Behaviors Regarding Covid-19 Affliction among Healthcare Workers in Pakistan
- “Competitive Landscape and Brand Equivalents: Implications for ANDA (Abbreviated New Drug Application) Approval”