Diastrophic Dysplasia, a Rare Cause of Congenital Dwarfism
Diastrophic dysplasia (DTD) is a rare skeletal disorder in the spectrum of a specific gene mutation. The term “diastrophos” which means curved or bent in Greek wasfirst reported by Lamy, et al in 1960 from their observation of 3 patients. Since then, we have progressed significantly to understand the disease presentation and inheritance pattern over time. Inherited as an autosomal recessive disease, the clinical presentation varies with distinct limb and spine anomalies in newborn infants.
Introduction
Diastrophic dysplasia (DTD) is a rare skeletal disorder in the spectrum of a specific gene mutation. The term “diastrophos” which means curved or bent in Greek wasfirst reported by Lamy, et al in 1960 from their observation of 3 patients [1]. Since then, we have progressed significantly to understand the disease presentation and inheritance pattern over time. Inherited as an autosomal recessive disease, the clinical presentation varies with distinct limb and spine anomalies in newborn infants. Diagnosis rests on combination of these distinct clinical & radiologic features, confirmed by genetic testing.It has anuncommon association with Pierre Robin Sequence. We report one such rare association in a neonate diagnosed with diastrophic dysplasia.
Case
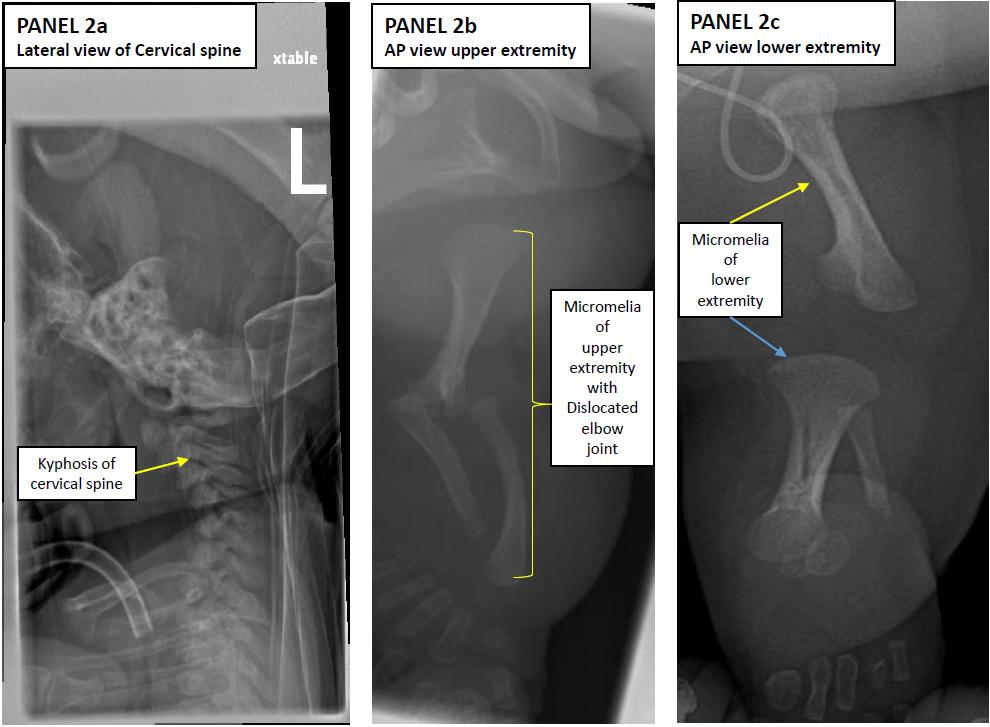
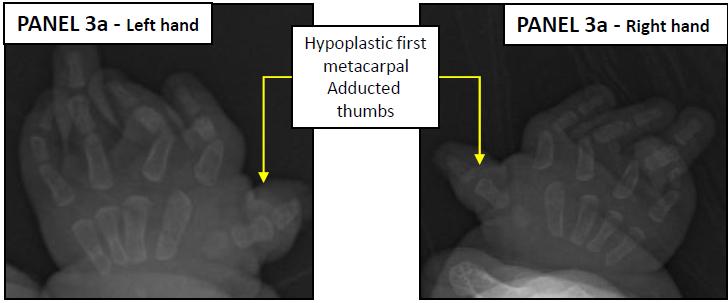
A 35 week late preterm female neonate was born to a 23 year old primi gravid mother by spontaneous vaginal delivery. Pregnancy was complicated by onset of preterm labor andfetal ultrasound showed shortened extremities, an abnormal spine and thickening from the neck down raising suspicion for dwarfism. Prenatal aneuploidy screen were all negative.Admission clinical exam showed micrognathia, glossoptosis and cleft palate (Pierre robin Sequence), short extremities, broad nasal bridge, small trunk, persistently abducted thumb (hitchhiker thumb) and a cystic lesion on the pinna. She was intubated by the anesthesiologist using a fiber optic laryngoscope on day of life one and a tracheostomy was placed on the fourth day of life to aid in mechanical ventilation. Echocardiography, renal and pelvic ultrasound were normal but skeletal survey showed features of diastrophic dysplasia which include cervical kyphosis, hind foot varus, foreshortening of extremities, small phalanges in hands and feet and hitchhiker thumb (Figures 1-3). Screening for mutation in SCL26A2 gene confirmed the diagnosis of DTD. She is currently doing well and being managed outpatient by various subspecialists.
Discussion
DTD (OMIM # 222600), also known as disastrophic dwarfism is a rare form of dwarfism present at birth.Prevalence is estimated at 1-1.3/100,000, though in Finland, 1-2% of the general population are carriers with a prevalence ratio of 1 in 30,000 [2]. It is inherited in an autosomal recessive manner [3] with complete penetrance and affects males and females equally. Mutations intheSLC26A2 gene (also called diastrophic dysplasia sulfate transporter (DTDST) gene) located at chromosome 5q32-q33.1 are responsible for the clinical presentation [4]. The SLC26A2 gene is the only gene currently known to be associated with DTD. SLC26A2 encodes a sulfate transporter protein that is predominantly expressed in the cartilage. This transmembrane protein transports sulfate into chondrocytes to maintain adequate sulfation of proteoglycans. Undersulfation of proteoglycans affects the composition of the extracellular matrix and leads to impaired proteoglycan deposition which is necessary for proper enchondral bone formation [5, 6].This leads to the characteristic clinical findings - limb shortening (micromelia), joint dislocations of elbow, hips or knees, small first metacarpals, Hitchhiker thumb, spinal curvature abnormalities, kyphosis, interpeduncular narrowing of lumbar spine and ear anomalies [7, 8, 9, 10]. Cleft palate ormicrognathia have been widely reported in the literature as associated clinical features of DTD. However, there has been limited description of the entire Pierre Robin sequence as seen in our patient. Genetic testing of our patient revealed her to be heterozygous in the SLC26A2 gene for a sequence variant designated c835C>T which has been reported to be a cause of DTD [2, 11]. More than 20 SLC26A2 gene mutations have been identified in patients with DTD.
Mortality due to respiratory obstruction including laryngeal stenosis has been reported to be as high as 25% [12]. Early suspicion and intervention with a tracheostomy improved survival of our patient. Survivors are reported to be healthy with a normal intelligence, but suffer from complications related to spine and limb anomalies [13]. Growth failure is progressive & universal and the pubertal growth spurt is weak or absent leading to dwarfism. Prenatal testing using specific DNA markers in combination with ultrasound can be helpful in early suspicion and diagnosis, however in most cases the diagnosis is confirmed postnatally.
The differential diagnosis of congenital dwarfism is diverse and extensive. It can be broadly classified as proportionate or disproportionate and etiologies vary from endocrine, genetic to various types of skeletal dysplasias. Advancements in medical science and diagnostic testing has helped us appreciate the differential diagnosis better, however such testing is often time consuming and expensive. Thus knowledge of clinical presentation of such rare diseases helps the pediatrician be better prepared towards the immediate management of these patients and eventually coordinate long term care in conjunction with various subspecialists.
Figures

Pediatrics & Neonatal Biology Open Access
1. Lamy M, Maroteaux, P (1960) [Diastrophic nanism] Presse Med 68: 1977-1980.
2. Hastbacka J, Kerrebrock A (1999) Identification of the Finnish founder mutation for diastrophic dysplasia (DTD). Europ J Hum Genet 7(6): 664-670.
3. Maeda K, Miyamoto Y (2006) A compound heterozygote harboring novel and recurrent DTDST mutations with intermediate phenotype between atelosteogenesis type II and diastrophic dysplasia. Am J Med Genet A 140(11): 1143-1147.
4. Hastbacka J, de la Chapelle A (1994) The diastrophic dysplasia gene encodes a novel sulfate transporter: positional cloning by fine-structure linkage disequilibrium mapping. Cell 78(6): 1073-1087.
5. Corsi A, Riminucci M (2001) Agenesis of Cartilage Interterritorial Matrix as the Link between Gene Defect and Pathological Skeletal Phenotype. Arch Pathol Lab Med 125(10): 1375-1378.
6. Forlino A, Piazza R (2005) A diastrophic dysplasia sulfate transporter (SLC26A2) mutant mouse: morphological and biochemical characterization of the resulting chondrodysplasia phenotype. Hum Molec Genet 14(6): 859-871.
8. Horton WA, Rimoin D (1978) The phenotypic variability of diastrophic dysplasia. The Journal of Pediatrics 93(4): 609-613.
9. Matsuyama Y, Winter RB, Lonstein JE (1999) The spine in diastrophic dysplasia. The surgical arthrodesis of thoracic and lumbar deformities in 21 patients. Spine 24(22): 2325-2331.
10. Remes V, Tervahartiala P (2001) Thoracic and lumbar spine in diastrophic dysplasia: a clinical and magnetic resonance imaging analysis. Spine 26(2): 187- 195.
11. Hästbacka J, Superti-Furga A (1996) Atelosteogenesis type II is caused by mutations in the diastrophic dysplasia sulfate-transporter gene (DTDST): evidence for a phenotypic series involving three chondrodysplasias. Am J Hum Genet 58(2): 255-262.
12. Friedman S I, Taber P (1974) A lethal form of diastrophic dwarfism. Skeletal Dysplasias. Amsterdam Excerpta Medica (pub): 43-49.
13. Crockett MM, Carten MF (2000) J Pediatr Orthop 20(4): 437-441.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?