Lysinuric Protein Intolerance: A Treatable Cause of Developmental Delay with Multiple Complications
Background: Lysinuric protein intolerance (LPI) is a multi systemic disease with a variety of clinical symptoms. Early and aggressive treatment can significantly reduce the number of hyperammonaemic episodes and prevent mental disability. Case series: We report a case series from two siblings with LPI: The eldest boy presented at three and a half years of age with short stature, global developmental delay & a history of recurrent infections. His younger brother was identified in the newborn period with lethargy and weight loss. Basic metabolic screening showed hyperammonaemia, gross urinary excretion of lysine & to a lesser degree increased excretion of arginine, ornithine and orotic acid. Plasma amino acids showed either low or low normal lysine, arginine and ornithine. Results: Both cases were treated with protein restriction, nitrogen scavengers, citrulline and L-carnitine. They were provided with an appropriate oral and intravenous emergency regimen for use when unwell. At the last follow-up the eldest boy showed a marked improvement in his development, whilst the youngest infant has normal physical & mental development for age. Conclusions: Marked improvement in LPI patients can be achieved by strict diet and medication with early identification & treatment likely to lead to the best possible intellectual outcomes.
Case Report
Index case
A three and a half-year-old boy were investigated for global developmental delay, hyperactivity and short stature. He is the first of three siblings from consanguineous parents. The second son is unaffected and the third boy was diagnosed with LPI soon after birth.
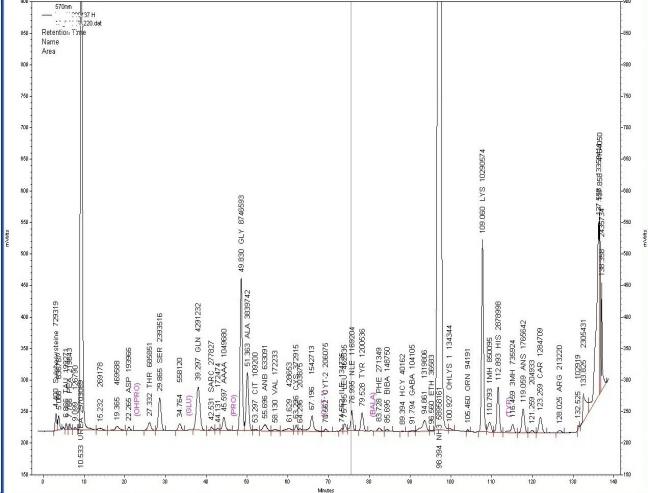
The index case attended a community developmental clinic where he was evaluated for global developmental delay. Following evaluation, a basic metabolic screening was undertaken which included plasma and urinary amino acids, organic acid and glycosaminoglycan. The plasma amino acids showed low lysine, ornithine, arginine and elevated glutamine (Table 1), with gross increased excretion of urinary lysine (Figure 1A). He was referred to a metabolic physician.
A full blood count, lymphocyte subsets, immunoglobulins, chest x-ray, DEXA scan and full biochemical evaluation was undertaken. Ammonia was 115μmol/L and there was gross urinary excretion of lysine. Urinary excretion of orotic acid was increased with plasma amino acids showing low lysine, arginine and ornithine (Table 1). Based on these result a diagnosis of lysinuric protein intolerance was made. Treatment included protein restriction to 1.5g/kg/day, sodium phenylbutyrate 250mg/kg/day, L-citrulline 100mg/kg/day and L-carnitine 20mg/kg/day. Low protein products were prescribed to provide calorie and variety in the diet. He was provided with an appropriate oral and intravenous emergency regimen for use when unwell.
| Index Case | Second Case | |||||||||||||
| Pre-Treatment | Post-Treatment | Pre-Treatment | Post-Treatment | |||||||||||
| Growth Parameters | 12.5 (2nd centile) | 14.2 (2nd centile) | 2.75 (2nd centile) | 3.29 (2nd centile) | ||||||||||
| Weight (kg) | 89.0 (<0.4th centile) | 99.7 (2nd centile) | 45.0 (< 0.4th centile) | |||||||||||
| Height (cm) | 33.0 (2nd centile) | 52.2 (2nd centile) | ||||||||||||
| Head Circumference | - | - | 36.5 (9th centile) | |||||||||||
| Laboratory Results | ||||||||||||||
| Blood* | ||||||||||||||
| Ammonia | 115 (<50) | 23 | 126 (<150) | 23 | ||||||||||
| Glutamine | 1381 (550-830) | 711 | 1612 (487-1031) | 996 | ||||||||||
| Lysine | 39 (50-233) | 59 | 186 (105-315) | 133 | ||||||||||
| Arginine | <5 (0-160) | 16 | 28 (10-70) | 13 | ||||||||||
| Ornithine | <5 (40-160) | 16 | 23 (25-225) | 26 | ||||||||||
| Urine§ | ||||||||||||||
| Lysine | 396 (10-68) | - | 1648 (22-171) | 1878 | ||||||||||
| Arginine | 9 (0-9) | - | 183 (0-14) | 605 | ||||||||||
| Ornithine | <5 (0-7) | - | 84 (0-19) | 135 | ||||||||||
| Organic acid | 2-ketoglutarate, glutarate | - | 2-ketoglutarate, fumarate | - | ||||||||||
| Orotic acid | 9.6 (<3.5) | 1.0 – 3.3 | 10.8 (<3.5) | 1.2 |
This is the third son who was admitted on day 4 with weight loss (10%), poor feeding and lethargy. On admission ammonia was 126μmol/L. Pre-treatment samples showed elevated urinary excretion of lysine, arginine, ornithine and elevated plasma glutamine. Urinary orotic acid was also increased. On review of preliminary results the baby was immediately treated with oral sodium benzoate 250mg/kg/day, L-citrulline 100mg/kg/day and protein restriction. Natural protein, as breast milk or proprietary milk, was restricted to provide 1.5g/kg/day. A protein free product, Energivit ® (carbohydrate and fat formula) was given to appetite to make up energy and volume requirements. Ammonia and plasma amino acids were all normal prior to discharge. At the age of two years, he was developmentally appropriate with growth parameters along the 2nd percentiles. Diagnostic confirmation by molecular analysis of the SLC7A7 gene showed both boys to be homozygous for c. [722G>A]; p.[(Gly241Asp)]. Both parents have been shown to be carriers of this mutation.
Discussion
Lysinuric protein intolerance (LPI, OMIM # 222700) is frequently under or misdiagnosed due to its highly variable, often nonspecific phenotype and often subtle biochemical abnormalities [2]. LPI is relatively common in Finland, with a prevalence of 1/60,000. It is also found in Southern Italy, Northern Japan and sporadically all over the world [2, 3, 4, 5]. It is caused by mutations in the SLC7A7 gene, which encodes the yþLAT-1 protein, the catalytic light chain subunit of a complex belonging to the heterodimeric amino acid transporter family [1, 2, 3, 4]. The reduced activity of the transporter (SLC7A7) leads to reduced absorption of arginine, ornithine and lysine in the kidney and intestine [5, 6]. LPI is a multi organ disease with a variety of clinical symptoms. Protein malnutrition and lysine deficiency contribute to the patient’s failure to thrive, as deficiency of arginine and ornithine result in dysfunction of the urea cycle with resultant hyperammonaemia and its developmental sequelae [2, 5]. On weaning, patients usually display an aversion to high-protein foods and show delayed bone growth, osteoporosis, hepatosplenomegaly and muscle hypotonia [2, 4, 5]. These clinical features were all present in the index case. Some patients experience chronic congenital diarrhoea due to the osmotic effect of high concentration of amino acids in the intestine [7]. Immune dysfunction attributable to nitric oxide (NO) overproduction secondary to intracellular trapping of arginine (due to defective efflux from the cell) is also a major feature. This may be a crucial Pathophysiological explanation for many LPI complications including severe lung disease with pulmonary alveolar proteinosis, renal disease, hemophagocytic lymphohistiocytosis (HLH) with subsequent activation of macrophages (MAS), various auto-immune disorders and an incompletely characterized immune deficiency [2, 3, 5, 8]. The index case experienced pneumonia at a young age and frequent respiratory tract infections. The diagnosis of LPI is based on the combination of increased urinary excretion and low plasma concentrations of the cationic amino acids [2, 5, 6]. It is vital that both urine & plasma amino acids are quantitated so as not to miss the diagnosis. This is illustrated in the sibling of the index case where plasma arginine and lysine were within the normal range with only ornithine mildly reduced. However the urine amino acids showed marked excretion of lysine, arginine and ornithine. Patients are treated with low-protein diet and supplementation of L-citrulline, which is absorbed by neutral amino acid transporters and serves to correct the urea cycle dysfunction. Citrulline is partially converted to arginine and ornithine. It is proposed that citrulline increases the intracellular synthesis of arginine and may further stimulate the immune cascade in renal tubular, glomerular and mesangial cells, alveolar macrophages and pulmonary epithelial cells and the reticular endothelial system. Thus regularly monitoring of plasma ammonia, glutamine and urinary orotic acid should be undertaken. If hyperammonemia develops, more severe protein restriction with or without nitrogen scavengers must be used [2, 5]. By giving early and aggressive treatment, the number of hyperammonaemic episodes can be reduced significantly thereby preventing intellectual disability [1, 2, 6, 8]. Given the multi-systemic nature of this disorder, care should be taken to monitor for, and to treat early, manifestation of HLH, MAS, nephropathy and immune dysfunction. A multi- disciplinary team approach is required in order to treat these patients successfully [2, 3]. In summary, we described a case series of LPI patients with a range of non-specific symptoms. In order to avoid missing the diagnosis we recommend careful quantitative evaluation of both plasma and urine amino acids. Marked clinical improvement can be achieved by diet and medication which is best achieved through early detection and treatment. Surveillance for other LPI associated complications should be part of the management of these patients.
References
-
Font-Llitjos M, Rodrıguez-Santiago B, Espino M, Sillue R, Manas S, et al. (2009) Novel _SLC7A7_ large rearrangements in lysinuric protein intolerance patients involving the same AluY repeat. Eur J Hum Genet 17(1): 71-79.
-
De Baulny HO, Schiff M, Dionisi-Vici C (2012) Lysinuric protein intolerance (LPI): a multi organ disease by far more complex than a classic urea cycle disorder. Mol Genet Metab 106(1): 12-17.
-
Barilli A, Rotoli BM, Visigalli R, Dall’Asta V (2013) Alterations of arginine in Lysinuric Protein Intolerance (LPI) macrophages. FASEB Journal 27: lb475.
-
Santamaria F, Mirra V, De Stefano S, Andria G, Parenti G (2013) Respiratory manifestations in patients with inherited metabolic diseases. Eur Respir Rev 22(130): 437-453.
-
Nanto-Salonen K, Niinikiski H, Simel OG (2012) Transport defects of amino acids at the cell membrane: cystinuria, lysinuric protein intolerance and Hartnup disorder. In: Saudubray JM, et al. (Eds.), Inborn metabolic diseases Heidelberg: Springer Medizin, p. 366-368.
-
Mikolajek-Bedner W, Torbe A, Kwiatkowski S, Michalezyk M, Gizewka M, et al. (2013) Pregnancy delivery and puerperium in patient with lyxinuric protein intolerance-a case report. Ginekol Pol 84(7): 654-656.
-
Terrin G, Tomaiuolo R, Passariello A, Elce A, Amato F, et al. (2012) Congenital Diarrheal Disorders: An Updated Diagnostic Approach. Int J Mol Sci 13(4): 4168-4185.
-
Mannucci L, Emma F, Markert M, Bachmann C, Boulat O, et al. (2005) Increased NO production in lysinuric protein intolerance. J Inherit Metab Dis 28(2): 123- 129.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?