Clinical Findings of Hearing and Communication Disorders in Goldenhar Syndrome: A Case Report
Goldenhar Syndrome or Oculo-auriculo-vertebral Spectrum is a rare complex syndrome characterized by incomplete development of the ear, nose, soft palate, lip and mandible, leading to communication disorders. Such child requires constant monitoring on development of speech and language abilities as well as surgical management. In the present study, clinical findings of a female child with 1.4 year old having bilateral atresia and diagnosed with Goldenhar syndrome was discussed.
Case Report
A female baby with the age of 1.4 years diagnosed as Goldenhar syndrome reported to our institution with complaints of limited speech output and hard of hearing. The patient reported of congenital malformation of both the ears. On observation, the physical features such as flat nose, asymmetrical jaws and hypo-tonicity of all four limbs were evident confirming the syndrome for the baby. The baby was subjected to both Audio logical and Speech- Language assessment.
Hearing Assessment
The Goldenhar syndromeic child presents a unique opportunity for the audiologist. Normally, most patients with GS demonstrate a maximum conductive hearing loss. In our client, as the age of the child was 1.4 years, Behavioral Observation Audiometry (BOA) was performed using Audio screener developed by Ali Yavar Jung National Institute of Speech and Hearing Disabilities (Divyangjan) [AYJNISHD (D)]. The responses elicited at different frequencies using the BOA were recorded and listed in table 1:
| Behavioral | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Response | Administration of test – Pictorial | ||||||||||
| Frequencies | Threshold | ||||||||||
| elicited | representation | ||||||||||
| (Intensity) | |||||||||||
| 500 Hz | 70dB | Eye widening & Blinking | |||||||||
| 1 kHz | 60dB | ||||||||||
| 2 kHz | 70dB | ||||||||||
| 4 kHz | 70dB |
Table 1: Minimum behavioral threshold level of the child using BOA test. As the client has multiple symptoms, it was difficult to
Table 1: Minimum behavioral threshold level of the child using BOA test. As the client has multiple symptoms, it was difficult to observe the behavioral responses. The above listed responses were keenly observed while presenting pure tone in each of the frequencies to confirm the behavioral threshold. Because, the majority of Goldenhar syndrome client’s exhibit bilateral atresia leading to a maximum bilateral conductive hearing losses, identification of integrity of the cochlea is a major audio logic challenge. However, as professionals, it is critical to precisely demonstrate normal cochlear function in both the ears for surgical consideration and further decisive rehabilitative strategies including appropriate need and fitting of amplification. Ultimately, electrophysiological measures which included Auditory Brain-stem Response (ABR) are the one of the tool to identify the residual cochlear function especially for babies with bilateral atresia.
The click stimulus was presented at 11.1/sec rarefaction, through calibrated TDH 39 Headphones for Air conduction (AC) stimulation to measure the auditory threshold function and integrity. The time window set was 12.5 msec with the filter settings of 100 to 3000 Hz. The intensity was decreased from 90 dBnHL in 10 dB step till the elicitation of V peak. Followed by the AC stimulation, a standard calibrated bone vibrator (Radio ear B-70A) was used to elicit Bone conduction stimulation. This is compulsory required for babies with bilateral atresia to identify the residual cochlea function. The ABR used for testing was 02 channel diagnostic equipment, Interacoustic Eclipse EP 15 Version: 4.3.0.17. The electrode placement and the ABR threshold level along with waveform are depicted in Figure 1.
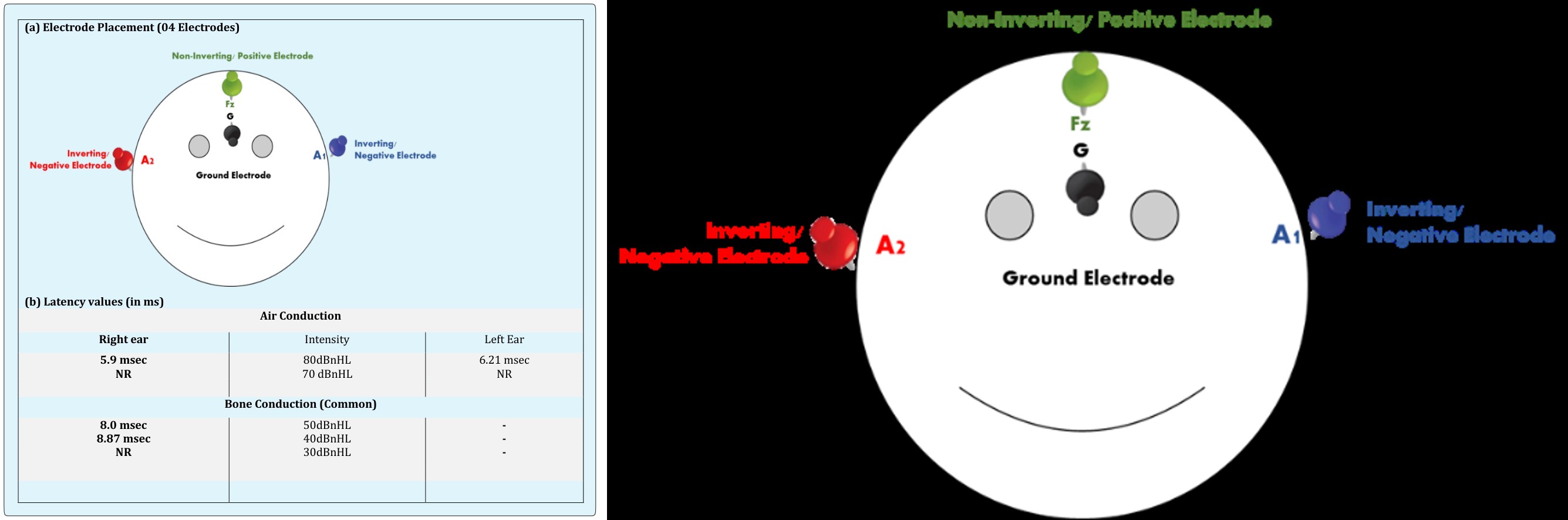
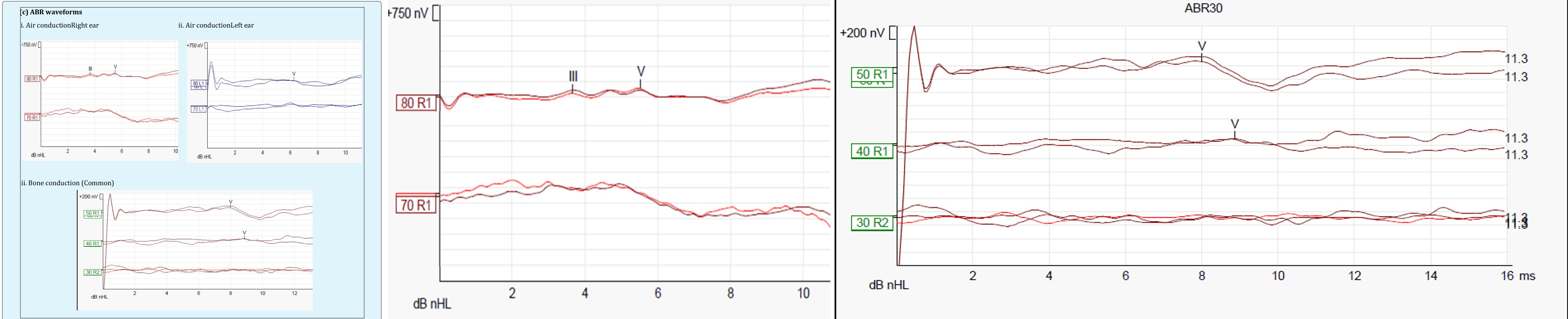
i. Air conductionRight ear ii. Air conductionLeft ear
Figure 1: (a) Electrode Placement for recording Air conduction and Bone Conduction ABR; (b) Latency (in ms); & (c) Waveform of Air conduction & Bone conduction. Threshold sensitivity for both AC and BC are estimated as the lowest replicable wave V peak component. Masking was not performed due to bilateral aural atresia and hence, the integrity of individual cochlear function was not established. The minimum level where response were elicited was 80 dBnHL for AC and 40 dBnHL for BC indicating normal cochlear functioning i.e. moderately severe conductive hearing loss. The findings of the ABR play an important role in the audio logic and surgical management for our GS patients. All audio logical assessments were carried out in ANSI (S3.1.1999) specified environment.
The purpose of the speech and language evaluation is to assess the child’s communication skills. Formal assessments, behavioral observation of the child, parental reporting and background information were carried out to determine the speech and language problem.
Oro-motor & Structural Analysis
On general examination, no evident deformity was noticed for the child except flat nasal bridge and hypotonic of all four extremities. On intra-oral examination, the child was presented with hypoplasia of mandible (asymmetrical jaws), and high arched palate without any cleft/other abnormalities. However, functionality was not tested due to the low mental age of the child to perform the requested task.
Receptive & Expressive Language Analysis
The child has poor speech-language and motor developmental milestones. The child was able to vocalize, and had differential cry with 2 syllable babbling. However, the child was able to response to the visual language of good bye and recognizes his name. Receptive Expressive Emergent Language Scale (REELS) by Bzoch and League [7] was administered to the child to identify the child’s receptive age and expressive age and the result revealed the child’s age of 7-8 months and 6-7 months respectively. As this speech disorder might be due to many associated conditions such as hearing loss and/or abnormalities seen in any of the Oro-motor structures, the development of speech and language abilities depends on the correction of such structural anomalies. Further examination on articulation, phonology, resonance, functional language system, auditory discrimination for perception and production of speech is required. However, major speech-language approach should be focused on receptive and expressive morph-syntactic abilities and linguistic conceptualization and organization for the treatment of phonological disorders.
Other Investigations
The child had undergone Chest radiography to rule out the abnormalities related to the respiratory mechanism and also Magnetic Resonance Imaging (MRI) of brain which showed normal study. Further, the child had undergone Karyotyping genetic testing to investigate the presence any genetic abnormality. The results of genetic study indicated normal female karyotype.
Discussion & Conclusion
Treatment of Goldenhar syndrome remains speculative and it usually varies with age, condition and systemic associations. Surgery of ear is usually recommended to those with atresia/Microtia and/or any other external/middle ear abnormalities without any neural damage, to regain the child’s hearing along with speech and Language therapy.
Several literature on Goldenhar syndrome had reported that most of the abnormalities prominently seen in external ear i.e. 70 – 80% (Microtia, Anotia, Pre-auricular appendages, Agenesis of ear lobe & external auditory canal). Abnormalities are also seen in ossicular chains, malformed ossicles, reduced oval window and also in oro- motor structures i.e. cleft lip and palate in few of the clients with Goldenhar syndrome [8, 9, 10]. Such abnormalities might be due to the blastogenesis dysfunction affecting the first and second pharyngeal arches that might hamper the development of external and middle ear structures during the embryonic growth period [11]. Observation of such abnormalities and the clinical findings in our client would require immediate attention for rehabilitation, as it may negatively affect a child's speech and interfere in their learning and social life. As the reconstruction surgery usually takes place in later stage of child’s life, Bone conduction hearing aids/BAHA shall be recommended for child’s early development of speech and language skills. Further, other correctable structures such as Jaw asymmetry and cleft lip and palate can be improved through reconstruction surgeries in the early teen age followed by plastic surgery. Often children with Goldenhar syndrome exhibit poor developmental and distinct delays in communicative, social, and cognitive development. By focusing on those areas, the clinician should cognize the developmental context of the child that could exhibits delay in language learning. Hence, proper and adequate diagnosis in the early years of child’s could help in execution of early auditory interventions as well as speech and language therapies, which ensures better quality of life to the patients.
Authors Contribution
Sabarish A, Performed analysis on clinical findings, & interpreted data, supervised development of work, manuscript evaluation and acted as Corresponding author; Arunraj K, Conception/design of the work, wrote manuscript, helped in data interpretation and Final approval of the version to be published; & Patil A & Bharath R, Data collection and administration of test tools.
References
-
Cohen MM, Rollnick BR, Kaye CJ (1989) Oculoauriculovertebral spectrum: An updated critique. Cleft Palate J 26(4): 276-286.
-
Sharma JK, Pippal SK, Raghuwanshi SK, Shitij A (2006) Goldenhar-Gorlin's syndrome: A case report. Indian J Otolaryngol Head Neck Surg 58(1): 97-101.
-
Mahore A, Dange N, Nama S, Goel A (2010) Facio- auriculo-vertebro-cephalic spectrum of Goldenhar syndrome. Neurology India 58(1): 141-144.
-
Gorlin RJ, Cohen MM, Levin KS (1990) Syndromes of the head and neck. 3rd (Edn.), Oxford, England, Oxford University Press, pp: 977.
-
Kapur R, Kapur R, Sheikh S, Jindal S, Kulkarni S (2008) Hemifacial-microsomia: A case report. Journal of Indian Society of Pedodontics and Preventive Dentist 26(5): 34-40.
-
Kulkarni V, Shah MD, Parikh A (1985) Goldenhar syndrome: A case report. Journal of Postgraduate Medicine 31: 177-179.
-
Bzoch KR, League R (1991) The Bzoch-League Receptive-Expressive Emergent Language Scale (REEL Scale)/Assessing Language Skills in Infancy. Retrieved from http://www.uakron.edu/chp
-
Skarżyński H, Porowski M, Podskarbi-Fayette R (2009) Treatment of otological features of the oculoauriculovertebral dysplasia (Goldenhar syndrome). Int J Pediatr Otorhinolaryngol 73(7): 915- 921.
-
Rosa RF, Silva AP, Goetze TB, Bier BD, Almeida ST, et al. (2011) Ear abnormalities in patients with oculo- auriculo-vertebral spectrum (Goldenhar syndrome). Braz J Otorhinolaryngol 77(4): 455-460.
-
Sleifer P, Gorsky Nde S, Goetze TB, Rosa RF, Zen PR (2014) Audiological Findings in Patients with Oculo- Auriculo-Vertebral Spectrum. Int Arch Otorhinolaryngol 19(1): 5-9.
-
Scholtz AW, Fish JH, Kammen-Jolly K, Ichiki H, Hussl B, et al. (2001) Goldenhar's Syndrome: Congenital Hearing Deficit of Conductive or Sensorineural Origin? Temporal Bone Histopathologic Study. Otol Neurotol 22(4): 501-505.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?