Sonographic Eye on Dengue during Clinical Evaluation and Early Diagnosis in Children
The study was done during epidemic of dengue in South India tertiary paediatric Hospital during 2019, for a period of one month. Role of ultrasound in early identification of dengue and its complications along with clinical and laboratory investigations. Ultrasound was performed on 112 patients (14 years) referred from dept. of paediatrics for ultrasound with features of dengue and its complication and later confirmed the diagnosis with serology proven. 30 patients were serologically negative for dengue fever hence excluded from the study. Out of 92 serologically positive cases 31 cases visited hospital at early stage and undergone ultrasound during 2/3rd day and 5/7th day of fever. During 2/3rd day ultrasound showed as almost all showed gall bladder wall thickening and pericholecystic fluid (in different patterns), 32.5% had hepatomegaly, 16.12% had splenomegaly and 19.35% right minimal pleural effusion, 3.25% left plural effusion. Follow-up ultrasound on fifth to seventh day revealed ascites in 93.5%, hepatomegaly in 90.3%, right plural effusion 80.6%, left pleural effusion in 41.9% and pericardial effusion in 29%. Of the 61 patients who underwent the study on fifth to seventh day of fever for the first time almost all had gall bladder wall thickening, 95.0% had hepatomegaly, 27.8% had splenomegaly, 96.7% had ascites, 95.08% had right pleural effusion, 75.4% had left pleural effusion and 22.9% had pericardial fluid. To conclude, in an epidemic of dengue, ultrasound features of thickened gall bladder wall, pleural effusion heaptomegaly and ascites should strongly favour the diagnosis of dengue fever.
Introduction
Dengue fever is known for more than centuries in countries of South East Asia and Western Pacific regions Investigation Paper [1]. Up to 50-100 million infections are estimated to occur annually in all over 100 endemic countries putting half of world population at risk. This disease is mainly prevalent in India, Indonesia, Thailand, Myanmar, Bangladesh and Srilanka [1, 2, 3].
In early July 2019, there was an outbreak of dengue in Telangana, a part in Southern India. Since there is no single test that can be used to diagnose dengue with a reasonable degree of accuracy and reliability, the diagnosis is based on clinical appearance in combination with serology. Serology takes approximately 7 to 10 days to give a positive result. The purpose of our study was to analyses retrospectively on children with dengue (1-14 yrs.) clinical featured cases and correlation of ultrasound findings with dengue severity and early identifications [4].
Material and Methods
It’s a retrospective observational study (Consent not required), Children’s who came with fever, rash ,myalgia, head ache with clinical features of dengue to Dept. of Paediatric at tertiary govt hospital sent for sonography and serological investigations, and results are analysed.
As serology will take time ( positive after 7-10 day ), evaluation started with sonography of abderman under categories from the onset of fever children’s undergone scan 2/3rd day and 5/7th day, and children undergone scan/sonography of abderman at 5-7th day finding only.
Among 112 study sample population 31 cases with fever subsided and few left against medical advice.92 cases are thoroughly studied for sono and serological study (Table 1).
Sample of dengue suspected 112 cases with fever taken, out of them 30 cases are serologically negative, and 92 cases are serologically dengue positive cases are reported. Among 92 cases 31 cases reported hospital at early onset of fever hance they under gone scan/ sonography 2/3rd and 5/7th day and 61 cases came with some delayed onset of fever hance scan done at 5/7th day of fever and sonographic findings evaluated [5].
All the subjects (Children) are trans abdominal, tran thorasic sonographic examination with 3.5MHz and 5MHz probes in supine and sitting position. GB wall thickinening, pericholicystic collections, hepatomegaly, splenomegaly, right plural effusion, left plural effusion, ascites, pericardial effusions are evaluated accordingly (Figure 1).
Statistical Analysis
All the data was entered in a spread Microsoft excel sheet and data was entered and corrected. The corrected data was analyzed and evaluated using SPPS software version 20 for Windows 10. Qualitative variables such as presence of various ultrasound findings were expressed as percentages.
| Total sample | Children with serologically dengue positive | Children dengue like fever(false positive) | ||||||
|---|---|---|---|---|---|---|---|---|
| 112 | 92 | 31 |
Table 1: Total number of cases with serologically dengue positive.
Among 31 cases presented to hospital early of fever are undergone sonography at 2/3rd day and 5/7th day, and following parameters are noted (Table 2 & 3).
| 2-3rd day of fever | 5-7th day of fever | |||||
|---|---|---|---|---|---|---|
| GB wall thickening, peri cholic collection | 31 (100%) | 31 (100%) | ||||
| Hepatomegaly | 10 (32.25%) | 28 (90.3%) | ||||
| Splenomegaly | 5 (16.12%) | 7 (22.5%) | ||||
| Right plural effusion | 6 (19.35%) | 25 (80.06%) | ||||
| Left plural effusion | 1 (3.22%) | 13 (41.9%) | ||||
| Ascitis | 3 (9.67%) | 29 (93.5%) | ||||
| Pericardial effusion | 0 (0%) | 9 (29.0%) |
Table 2: Sonography parameters in children evaluated at early onset of fever of in 31 children
| 5-7th day of fever | |||
|---|---|---|---|
| GB wall thickening, peri cholic fluid collection | 61 (100%) | ||
| Hepatomegaly | 58 (95.0%) | ||
| Splenomegaly | 17 (27.8%) | ||
| Right plural effusion | 58 (95.8%) | ||
| Left plural effusion | 46 (75.4%) | ||
| Ascites | 59 (96.7%) | ||
| Peri cardial effusion | 14 (22.9%) |
Table 3: Sonographic evaluation of 61 children at 5-7th day of fever.
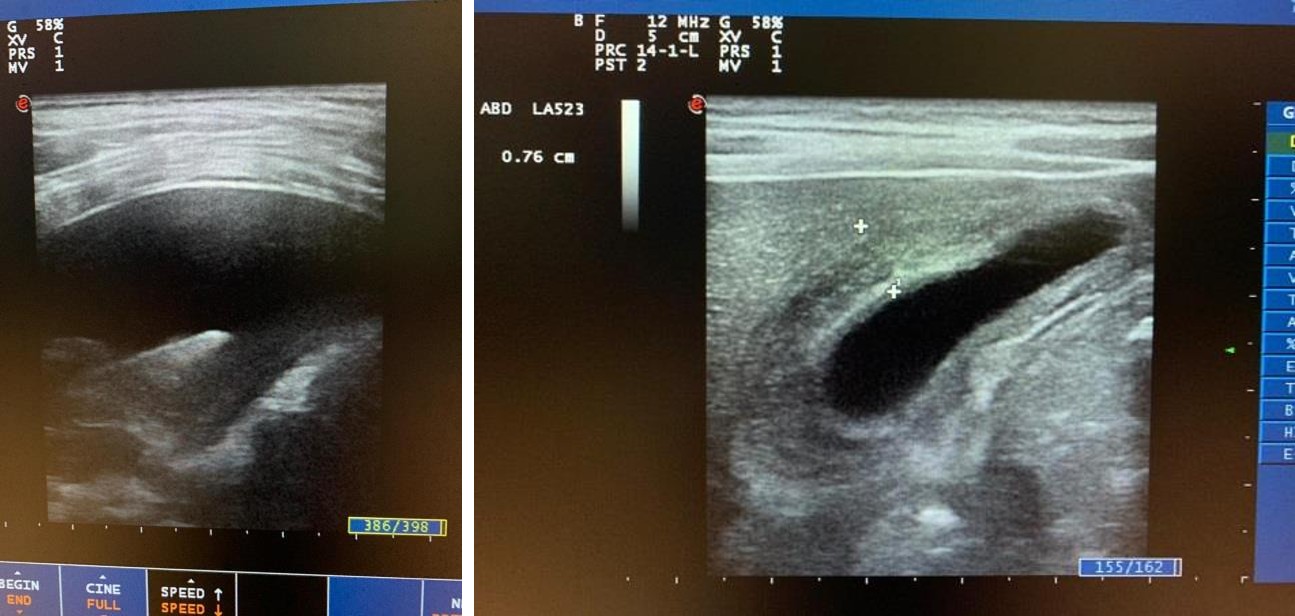
Figure 1 & 2: Showing right plural effusion, Gall bladder thickening in dengue positive cases.
Discussion
Dengue is the most common arboviral disease caused by flavi virus. Rapid globalisation, mechanical lifestyle modifications and poor water, sanitation management, lack of awareness in general public has contributed to significant increase in the risk of DF [6]. In the last 50 years, incidence has increased 30-fold with increasing expansion to new countries. DF is endemic in many tropical and subtropical regions, like Southeast Asia (including India) [7, 8]. Dengue was endemic in 23 states in 2011-12 in India [9]. In 2015, Delhi, India, recorded its worst outbreak since 2006 with over 15,000 cases [10].
Even through Serological tests are still the mainstay for confirmation of diagnosis in dengue, but can delay the diagnosis. Hence, additional diagnostic modalities are often sought for early detection of dengue. The early ultrasonographic findings favoring the diagnosis of dengue have been reported in the literature with varying combination like our study as gall bladder wall thickening, ascites, pleural, pericardial effusions and organomegaly etc [11, 12, 13].
During first 2/3rd almost all the cases shows gall baldder thicking (100%), hepatomegaly (32.25%). Hepatomegaly is the one factor usually misleads in children, as each age group has different range, as a routine practice come as normal liver size ( irrespective of age of children), when the same patients follow up scan after 5-7th day shows consistent GB wall thickening with pericholic fluid collection (vary with seviority), more severity ascites, hepatomegaly, right effusion noted. There is no evidence of literature or reason why right plural effusion is more common in dengue, mostly assumed as anatomical advantage of left plura due to space occupying cardiac structures, less volume of lung, less volume pericapillary leak.
Similarly those children who undergone scan on 5-7th day are also showed similar findings. Hence it’s shows clinical features with as above sonographaic parameters helps early identification of dengue and prevents its complications as haemorrhage and shock.
Our study coincides with other studies, and also focusing a new factor as Hepatomegaly ,often missed in paediatric group as its range vary in each age group and gives sonographic eye to early evaluation of dengue in children [10, 14, 15, 16].
Acknowledgements
Authors thank the Faculty of Radio Diagnosis and Dept. of Pediatrics and Non-medical staff, Osmania Medical College, Hyderabad and Telangana.
References
-
WHO (1997) Dengue haemorrhagic fever; diagnosis, treatment, prevention, and control. Geneva: World Health Organization.
-
WHO (2008) Health Situation in South East Asian Region 2001-2007. New Delhi: Regional Office for SEAR.
-
WHO (1999) Health Situation in the South East Asia Region 1994–1997, New Delhi: Regional office for SEAR.
-
Pramuljo HS, Harun SR (1991) Ultrasound findings in Dengue haemorrhage fever. Pediatr Radiol J 21: 100- 102.
-
Santhosh VR, Patil PG, Srinath MG, Kumar A, Jain A, et al. (2014) Sonography in the diagnosis and assessment of dengue Fever. J Clin Imaging Sci 4(1): 14.
-
Joshi P, Rathnam VG, Sharma S (1997) USG findings in
-
WHO (2008) Dengue and Dengue Haemorrhagic Fever. Geneva: World Health Organization.
-
(2006) New Delhi: Ministry of Health and Family Welfare; Internet, Government of India. National Vector Bourne Disease Control Programme.
-
Singh B (2007) Dengue outbreak in 2006: Failure of public health system?. Indian J Community Med 32: 99-100.
-
Motla M, Manaktala S, Gupta V, Aggarwal M, Bhoi SK, et al. (2011) Sonographic evidence of ascites, pleura- pericardial effusion, and gall bladder wall edema as non-invasive, rapid diagnostic markers for dengue fever. Prehosp Disaster Med 26(5): 335-341.
-
Asghar J, Farooq K (2011) Radiological appearance and their significance in the management of dengue hemorrhagic fever. Pak J Med Health Sci 5(3): 685- 692.
-
Government of India (2010) Annual Report 2009- 2010. New Delhi: DGHS, Ministry of Health and Family Welfare.
-
WHO (1993) Monograph on Dengue/Dengue Haemorrhagic Fever, Compiled by Prasert Thongchroen Regional Publication. SEARO No.22.
-
Vedaraju KS, Kumar KRV, Vijayaraghavachari TV (2016) Role of Ultrasound in the Assessment of Dengue Fever. Int J Sci Stud 3(10): 59-62.
-
WHO (2000) Weekly epidemiological record. World Health Organisation 24: 193-196.
-
(2007) Jawetz, Melwick 24th (Edn.), McGraw Hill, Lange Publications. Adelberg's Medical Microbiology pp: 350-355. dengue haemorrhagic fever – our experience in the recent epidemic. Ind J Radiol Imag 7: 189-192.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?