Meconium Periorchitis - An Unusual Cause of Scrotal Mass in a Neonate
Meconium periorchitis (MPO) is an uncommon entity associated with meconium peritonitis where the meconium gained access to the tunica vaginalis, results in meconium periorchitis. The typical presentation is a soft hydrocele at birth which becomes harder over weeks span due to calcification of meconium. A lack of awareness about this disease entity may lead to scrotal exploration. It can resolve spontaneously without compromising the testicle. Scrotal ultrasound is the mainstay of imaging. We report a case of a meconium periorchitis and review the relevant literature.
Introduction
Meconium periorchitis is an uncommon condition which is the result of healed meconium peritonitis occurring in late fetal life or in the early postnatal period. Meconium reaches the paratesticular soft tissues via a patent processus vaginalis can cause sterile inflammation of the paratesticular tissues [1]. Subsequent fibrosis and calcification may then lead to firm to hard mass that mimics a testicular or paratesticular tumour [2]. Clinical manifestations of Meconium peritonitis may vary from incidental finding of diffuse intraabdominal calcifications, bowel obstruction, ascites with abdominal distension and high mortality. Meconium has also been demonstrated thoracic cavity, pelvic soft tissues and even in scrotum. Both the masses and the calcifications associated with meconium orchitis have the tendency to resolve spontaneously without compromising the testicle. It mimics a scrotal mass, and without knowledge of this entity, it may lead to unnecessary surgical exploration. Meconium periorchitis can be suspected based on radiologic evaluation with ultrasound that will show the presence normal testis with extra-testicular echogenic foci. Abdominal plain may also demonstrate diffuse intraabdominal calcifications. As most extra-testicular lesions are benign, whereas most intratesticular lesions are malignant. Finding of the normal testis differentiate it from scrotal tumors.
A 5-day-old healthy term boy who was delivered normally was admitted to our department with left scrotal swelling. Antenatal period of pregnancy was uneventful, with a single prenatal ultrasound in last trimester, which was normal. There was no history of delayed passage of meconium or abdominal symptoms after reviewing the medical records. The baby appeared active and was feeding fine. On local examination, left scrotal swelling was noted with absence of any erythema or redness. On palpation, the swelling was painful and firm.
Transillumination test showed translucence in some areas, suggesting hydrocele and opaque areas with firm consistency suggesting a scrotal mass. The scrotal mass was localized, not clearly separable from the testis. Right testis was normally descended and normal. The scrotal ultrasound demonstrated a normal left testis with normal size, shape, and echogenicity. There was an extra-testicular mass of approximately 2.2x2.1x1.9 cm dimension distinctly separated from the ipsilateral testis with scattered calcification. Small hydrocele was also present Figure 1.
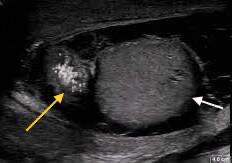
Figure1: The scrotal ultrasound demonstrated a normal left testis with normal size, shape, and echogenicity (white arrow). There was an extra-testicular mass distinctly separated from the ipsilateral testis with scattered calcification (yellow arrow). Small hydrocele was also present.
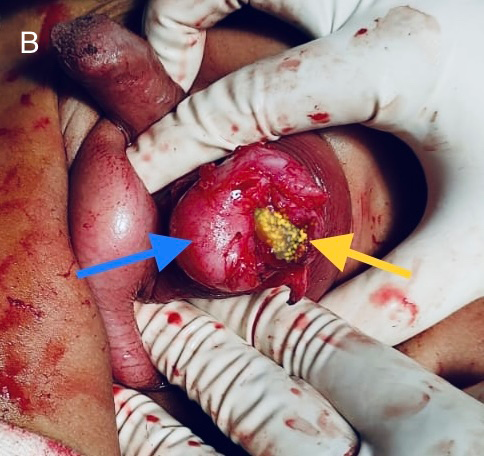
Clinical laboratory studies, including routine blood parameters, C‐reactive protein and procalcitonin, were within normal limits. X‐ray of the abdomen and chest were normal. The patient underwent a scrotal exploration, well circumscribed, firm paratesticular mass greenish in colour, which was adherent to the tunica vaginalis but separated from the testis (Figure 2) Careful dissection was done until the entire mass could be removed without causing any damage to testis. The scrotal wound was closed.
Postoperative period was uneventful, and baby was discharged on third post-operative day. Histopathological examination shows fibro connective tissues with abundant mucoid degeneration and focal areas of calcification. Features are consistent with MPO. The patient was reviewed in out- patient with scrotal ultrasound that was found to be normal.
Discussion
The first description of meconium periorchitis was made by Olnick and Hatcher in 1953 [3]. The clinical diagnosis of meconium periorchitis is most often suspected in the presence of scrotal swelling with firm to hard mass associated with diffuse intraperitoneal calcifications. Sometimes intraperitoneal calcifications may not be visible. Initially the scrotal effusion is soft and transforms within a few weeks into mass of a solid consistency. The presence of calcifications on plain abdominal X-rays and finding of a normal ipsilateral testis with echogenic extra-testicular mass on ultrasound is the key element of the diagnosis [2, 3, 4] which, according to Friedman et al. [5] to avoid surgical exploration. Other locations, notably thoracic, extra peritoneal, inguinal and vulvar, have been reported sporadically [6, 7].
Meconium is the greenish, viscous intestinal content of the distal small bowel present after the fourth month of fetal life. Meconium peritonitis occurs when a bowel wall rupture during late fetal life or early postnatal life allows meconium to enter the peritoneal cavity. If the ruptured bowel wall heals, there may be no evidence of the cause or the site of perforation but will be visible as diffuse calcifications on abdominal radiograph. When this meconium traverses through patent processus vaginalis, it incites an inflammatory reaction within the scrotal sac that may result in MPO and the mass‐like lesion.8 Suspicion of neoplasia, although uncommon in this period of life, may be caused by a scrotal mass or sonographically detectable calcifications. However, we must not omit the existence of calcifications linked to other causes, in particular testicular teratoma, gonadoblastoma and Leydig and Sertoli cell tumors. [10]. In the case of meconium periorchitis, the testicle itself is healthy. In case of doubt, exploration is necessary with examination of the calcified mass.
A conservative attitude is recommended by most authors, especially since the long-term evolution of these periorchitis can lead to the spontaneous resolution of the calcified scrotal masses [11, 12]. In case of MPO, surgical exploration is indicated to confirm the diagnosis when abdominal calcifications are not present; a scrotal tumor is suspected when there is progressive enlargement of the testis as in our case where abdominal radiography and ultrasonography did not show abdominal calcification and therefore scrotal exploration was performed. Review of previous studies indicated that despite the benign nature of MPO, unnecessary orchidectomies were performed in 18% of the cases2 because of confusing presentation mimicking scrotal tumour.
Isolated calcifications in the scrotum without peritoneal involvement are seen in neoplasms such as teratoma, gonadoblastoma, rhabdomyosarcoma, metastatic neuroblastoma, lymphoma and pseudotumor. The visualization of the normal testicle on ultrasonography differentiates meconium periorchitis from scrotal tumors. The diagnosis of MPO should be considered as one of the causes of scrotal masses in infants and young children and this may obviate unnecessary orchidectomy.
Conclusion
When we encounter any case of neonate or infant with firm to hard extra-testicular scrotal mass with calcifications and presence of normal ipsilateral testis, in that case it is important to consider MPO as one of the aetiologies of congenital scrotal mass, thereby avoiding unnecessary orchidectomies.
References
-
Kalra P, Radhakhrishnan J (2006) Meconium periorchitis. Urology 68(1): 202.
-
Dehner LP, Scott D, Stocker JT (1986) Meconium periorchitis A clinicopathologic study of four cases with a review of the literature. Hum Pathol 17(8): 807-812.
-
Olnick HM, Hatcher MB (1953) Meconium peritonitis. JAMA 152(7): 582-584.
-
Ring KS, Axelrod SL, Burbige KA, Hensle TW (1989) Meconium hydrocele an unusual etiology of a scrotal mass in the newborn. J Urol 141(5): 1172-1173.
-
Friedman AP, Haller JO, Goodman JD (1983) Sonography of scrotal mass in healed meconium peritonitis. Urol Radiol 5(1): 43-46.
-
Mitsudo SM, Boley SJ, Rosenzweig MJ (1983) Extraperitoneal pelvic meconium extravasation in a newborn infant. J Pediatr 103: 598-600.
-
Farelly G, Fitzgerald R, Mathews T (1983) Meconium thorax. J Pediatr Surg 18: 623-624.
-
Sung T, Riedlinger WFJ, Diamond DA, et al. (2006) Solid extratesticular masses in children radiographic and pathologic correlation. AJR Am J Roentgenol 186(2): 483-490.
-
Thompson RB, Rosen DI, Gross DM (1973) Healed meconium peritonitis presenting as an inguinal mass. J Urol 110: 364-365.
-
Fries JW, Talbot BS (1955) scrotal calcification due to meconium peri tonitis. J Urol 73(6): 1059-1068.
-
Kenney PJ, Spirt BA, Ellis DA, Patil U(1985) Scrotal masses caused by meconium peritonitis prenatal sonographic diagnosis. Radiology 154(2): 362-363.
-
Fair KP, Cho MH (1997) Pathological case of the month. Arch Pediatr Adolesc Med 151(8): 853-854.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?