The Molecular Detection of mecA Genes of Staphylococcus Aureus
Antibiotic resistance is common among pathogenic bacteria associated with community acquired and nosocomial infections. Methicillin-resistant Staphylococcus aureus (MRSA) infections have become a global health problem particularly in hospital setup causing simple skin infections to life threatening infections. The present study aimed to investigate the presence of mecA genes in MRSA from pigs, using Polymerase Chain Reaction. One hundred S. aureus isolates of blood samples from Pigs in Bariga, Lagos State were collected from Molecular Biology and Biotechnology Unit, Nigeria Institute of Medical Research. Methicillin resistance was determined by Kirby-Bauer’s disc diffusion method. The PCR was used for mecA gene detection from MRSA strains. Twenty-five pure Staphylococcus aureus isolates were identified based on cultural characteristics, biochemical reactions and positive slide coagulase test. Out of these, 11 (44%) strains were MRSA by phenotypic method. Amplification of mecA gene for all the 11 MRSA isolates was negative when visualized on 2% agarose gel electrophoresis. Eleven strains of MRSA were found among Staphylococcus aureus isolates of blood samples from Pigs. The MRSA phenotype observed in the isolates was not the classical mecA mediated resistance. Hence, it is highly recommended to consider alternative mechanisms for β-lactams resistance that may compete with mecA gene in the emergence of MRSA phenomenon in Nigeria.
Introduction
Staphylococcus aureus is one of the most frequent bacterial pathogens encountered in humans where it causes skin infections, soft tissue infections, osteomyelitis, bacteremia, septicemia and respiratory tract infections in the community, as well as postoperative and catheter- related infections in hospitals [1] Methicillin resistant S. aureus (MRSA) have become major public health problem worldwide [2]. The burden of MRSA continues to raise with a rate of 14% of all S. aureus strains from clinically significant samples in New South Wales, Australia [3]. The rising colonization rates lead to the increasing of infection rates in the community and in hospitals. The consequence to the health care system is longer hospital stays and greater costs, which approximately double the expenditure per patient [4]. The patient risks include significantly higher mortality and morbidity rates with invasive MRSA infection [5]. Within U.S. hospitals, nearly 60% of nosocomial S. aureus infections acquired in intensive care units are methicillin resistant [5]. Health care workers may carry MRSA on their hands or clothes following their contact either with asymptomatic carriers or patients who have clinical infection, which may then, unknowingly transmit the organism to other patients. The contaminated environmental surfaces also contribute to MRSA transmission. Thus, symptomatic patients constitute a small portion of the actual reservoir of MRSA within hospitals resulting in an iceberg phenomenon [6]. The worldwide emergence of community acquired methicillin resistant S. aureus (CA-MRSA) can have severe public health implications [7]. The differentiation between community- acquired MRSA and hospital acquired MRSA (HA-MRSA) is becoming difficult to understand, since CA-MRSA could spread into hospitals [8]. The risk of acquiring MRSA in the hospitals increased by severity of illness, length of stay, use of intravascular devices and the intensity of exposure to infected patients [9, 10, 11, 12]. Infection control measures include screening, and segregation of positive patients, eradication of carriage and good standards of general hygiene [13, 14, 15, 16, 17].
Molecular study of antibiotic resistance gene from Staphylococcus aureus its amplification and sequencing of mecA gene which is responsible for most of the β-lactams antibiotics resistance including methicillin will give insight on how to design new synthetic drugs to control community acquired infections of S. aureus.
Methods
Collection and Identification of Isolates
A total of one hundred isolates of S. aureus from blood samples of pigs in Bariga, Lagos State were collected from the Molecular Biology and Biotechnology division of the Nigeria Institute of Medical Research Yaba, Lagos State. The isolates were sub cultured on Brucella medium after which Gram staining was carried out to confirm that the isolates are pure.
Mannitol salt agar was then used as selective medium for secondary isolation of the staphylococci. Isolates were inoculated unto Mannitol Salt agar plates and incubated at 37 °C for 24 to 48 hrs. Plates were examined for growth of colonies with the characteristic golden coloration.
Biochemical test such as the coagulase test was performed to confirm S. aureus strains for twenty-five isolates. The isolates were characterized by their Gram stain characteristics, growth on Mannitol Salt Agar and slide coagulase tests to confirm the S. aureus isolates [18].
Antimicrobial Susceptibility Test
Susceptibility test was done for all the isolates obtained against the following antibiotics: Methicillin, Oxacillin and Vancomycin (Oxoid, UK) by modified Kirby-Bauer technique. Nutrient agar medium containing 5% of sodium chloride was prepared, distributed in 20ml aliquots into bottles and sterilized at 121°C for I5 mins [19]. Overnight cultures of the confirmed S. aureus isolates were emulsified in 3ml of Phosphate buffered solution (PBS) and turbidity adjusted to 0.5 McFarland were inoculated unto the NA plates by swabbing. The paper disk (methicillin (5 μg), oxacillin (1μg) and vancomycin (30μg), were placed on the dried agar plates and incubated for 18 hours at 35oC prior to determination of results. The zones of growth inhibition around each of the antibiotic discs were measured to the nearest millimeter. The diameter of the zone is related to the susceptibility of the isolate and to the diffusion rate of the drug through the agar medium. The zone diameters of each drug were interpreted using the criteria published by the Clinical Laboratory Standards Institute (CLSI) [20, 21]
Detection of mec A Genes by PCR and Bacterial Genomic DNA Extraction
Eleven MRSA isolates identified by phenotypic method were subjected to detection of mecA gene using PCR. An overnight culture in Brain Heart Infusion (BHI) broth was collected by centrifugation and processed according to the procedure of Arakere, et al. [22]. The isolated DNA was stored at -20 °C till further use.
PCR Protocol
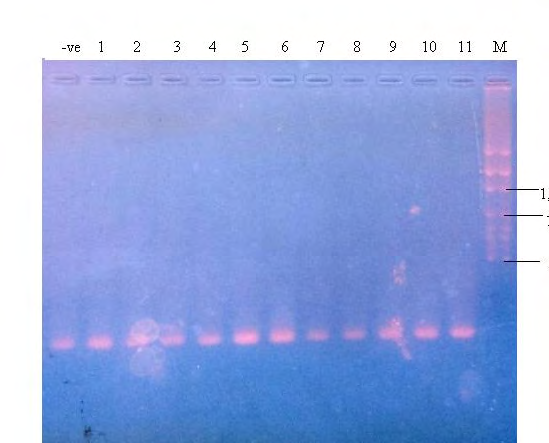
A three step PCR method reported by Oliveira, et al. [23] was carried out in a thermal cycler (Gradient thermocycler, Biologix, China) The primers used for amplification were; forward primer sequence mecA1 (AAAATCGATGGTAAAGGTTGGC) and reverse primer sequence mecA2 (5’AGTTCTGCAGTACCGGATTTTGC 3’). The conditions of PCR were as described by Murakami, et al. [24] which includes an initial denaturation at 94 °C for 5 min followed by 30 cycles of 94 °C for 60seconds, 62 °C for 30seconds, and 72 °C for 35seconds, annealing at 53 °C for 30seconds with a final extension at 72 °C for 10 min. The PCR product was finally visualized under UV transilluminator on 2% agarose and the image captured with 16MP Nikon Camera.
Results
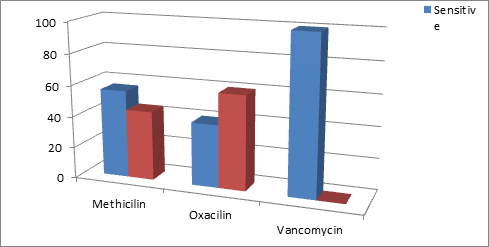
Out of a total of 100 isolates, 25 were pure Gram-positive cocci. of the total 25 S. aureus isolates studied, 11(44%) isolates were MRSA, 15 (60%) were resistant to Oxacillin and none was resistant to Vancomycin (inhibition zone of 12 mm or less by Kirby-Bauer’s disc diffusion method). The susceptibility pattern of the organism against the various antibiotics is shown in figure 1. 44% of the organisms were resistant with Methicillin while 56% were sensitive the antibiotic, 60% and 40% of the organisms were sensitive and resistant to Oxacillin respectively, while no strain was seen resistant to Vancomycin as they were all (100%) sensitive (Figure 1). PCR results indicated that 11 (44%) MRSA isolates were negative for mecA genes (absence of the corresponding band) (Figure 2).
Discussion
There was a high proportion of isolates that were resistant to methicillin and this is very worrisome particularly as the isolates were obtained from pigs. A previous study in Netherlands reported 39% MRSA out of 540 pig isolates. Perhaps the low number of isolates used in the study could have accounted for the high proportion of MRSA [25]. Findings of mecA gene were the major evidence for the detection of MRSA isolates [26]. However, findings in this project suggests low burden of the mecA gene, this may open the door to search for other intrinsic factors that may compete with mecA gene in producing resistance phenomenon in regions with high prevalence of MRSA in pigs. Also, a previous study in Nigeria reported the complete absence of mecA genes as well as the gene product of PBP2a in isolates which were phenotypically MRSA suggesting a probability of hyper production of β-lactamase as a cause of the phenomenon [27]. Moreover, recently Ba and colleagues mentioned specific alterations in different amino acids present in protein binding proteins cascade (PBPs 1, 2, and 3) which may be the basis of resistance [28]. These alterations were found to include three amino acid substitutions which were identical and were present in PBPs 1, 2, and 3. The same amino acid was found to have two other different substitutions in PBP1, both the identical and different amino acid substitutions were observed in isolates from different multilocus types. These findings provided clear evidence that there were mechanisms other than the presence of mecA gene responsible for beta-lactam resistance of MRSA and that molecular methods alone were not enough for confirmed characterization of MRSA isolates, a point that should be under consideration by regional and reference laboratories.
Conclusion
The phenotypic methicillin resistance observed in the isolates may not be due to the production of the altered PBP2a encoded by the mecA gene, but other factors such as hyper production of β-lactamase. MRSA without mecA gene were also being implicated in the cause of some severe infections. This study indicates that MRSA could be much more frequent among persons having contact with pigs than among other persons outside hospitals [29].
In conclusion, these findings indicate increasing prevalence of MRSA in pigs. However, the absence of mecA gene in a considerable percentage of MRSA isolates requires investigating the alternative genetic possibilities related to the resistance phenomena. A concerted research in similar area of study using methods that simplifies extraction and amplification of target DNA is required in other parts of Nigeria. This is to provide a clearer and broader picture on the existence of MRSA isolates in Nigeria.
References
-
Didier G, Stephane B, John S, Weber P, Simon S, et al. (2004) Amoxicillin-Clavulanate Therapy Increases Childhood Nasal Colonization by Methicillin-Susceptible Staphylococcus aureus Producing High Levels of Penicillinase. Antimicrob Agents Chemother 48(12): 4618-4623.
-
Jarvis R, Jarvis AA, Chinn RY (2012) National prevalence of methicillin-resistant Staphylococcus aureus in inpatients at US health care facilities, 2010. Am J Infect Control 40(3): 194-200.
-
Nimmo R, Coombs W, Pearson C, O Brien G, Christiansen J, et al. (2006) Methicillin-resistant Staphylococcus aureus in the Australian community: an evolving epidemic. Med J Aust 184(8): 384-388.
-
Kim T, Oh I, Simor E (2001) The economic impact of methicillin resistant Staphylococcus aureus in Canadian hospitals. Infect Control Hosp Epidemiol 22(2): 99-104.
-
Kearns M, Seiders J, Wheeler R, Steward M, Freeman R (1999) Rapid detection of methicillin resistant staphylococci by multiplex PCK. J Hosp Infect 43(1): 33- 37.
-
Harbarth S, Martin Y, Rohner P, Henry N, Auckenthaler R, et al. (2000) Effect of delayed infection control measures on a hospital outbreak of methicillin- resistant Staphylococcus aureus. J Hosp Infect 46(1): 43-49.
-
Calfee D, Durbin J, Germanson P, Toney DM, Smith EB, et al. (2003) Spread of methicillin-resistant Staphylococcus aureus (MRSA) among household contacts of individuals with nosocomially acquired MRSA. Infect Control Hosp Epidemiol 24(6): 422-426.
-
Wannet W, Heck M, Pluister G, Spalburg E, De Neeling A, et al. (2004) Panton-valentine leucocidine positive MRSA in 2003. the Duch situation. Eur Surveillance 9(11): 28- 29.
-
Ibelings M, Bruining A (1998) Methicillin-resistant Staphylococcus aureus: acquisition and risk of death in patients in the intensive care unit. Eur J Surg 164(6): 411-418.
-
Law R, Gill O (1998) Hospital acquired infection with methicillin-resistant and methicillin sensitive staphylococci. Epidemiol Infect 101(3): 623-629.
-
Pujol M, Pena C, Pallares R, Ayats J, Ariza J, et al. (1994) Risk factors for nosocomial bacteremia due to methicillin resistant Staphylococcus aureus. Eur J Clin Microbiol Infect Dis 13(1): 96-100.
-
Merrer J, Santoli F, Vecchi C, Tran B, De Jonghe B, et al. (2000) Colonization pressure and risk of acquisition of methicillin resistant Staphylococcus aureus in a medical intensive care unit. Infect Control Hosp Epidemiol 21(11): 718-723.
-
Girou E, Pujade G, Legrand P, Cizeau F, Brun Buisson C (1998) Selective screening of carriers for control of methicillin-resistant Staphylococcus aureus (MRSA) in high-risk hospital areas with a high level of endemic MRSA. Clin Infect Dis 27(3): 543-550.
-
Lucet C, Chevret S, Durand Zaluski I, Chastang C, Régnier B, et al. (2003) Prevalence and risk factors for carriage of methicillin resistant Staphylococcus aureus at admission to the intensive care unit. Arch Int Med 163(2): 181-188.
-
Arnold S, Dempse J, Fishman M, McAuley PJ, Tibert C, et al. (2002) The best hospital practices for controlling methicillin resistant Staphylococcus aureus on the cutting edge. Infect Control Hosp Epidemiol 23(2): 69-76.
-
Hill A, Duckworth J, Casewell M (1988) Elimination of nasal carriage of methicillin resistant Staphylococcus aureus with mupirocin during a hospital outbreak. J Antimicrob Chemother 22(3): 377-384.
-
Rampling A, Wiseman S, Davis L, Hyett AP, Walbridge AN, et al. (2001) Evidence that hospital hygiene is important in the control of methicillin resistant Staphylococcus aureus. J Hosp Infect 49(2): 109-116.
-
Baird D (1996) Staphylococcus: cluster forming cocci. In: Collee G, et al. (Eds.), Practical Medical Microbiology, 14th (Edn.), Churchill Livingstone, Ltd., Edinburgh 2: 245- 261.
-
Cookson B, Phillips I (1990) Methicillin-Resistant Staphylococci. Soc Appl Bacteriol Symp Ser 19: 55-70.
-
Cheesbrough M (2006) District Laboratory Practice in Tropical Countries. Part 2, Cambridge University Press, UK, pp: 136-142.
-
Clinical Laboratory Standards Institute (2006) Performance Standards for Antimicrobial Susceptibility Testing; Sixteenth Informational Supplement. CLSI Document M100-S16. Wayne, PA 19087-1898, USA.
-
Arakere G, Nadig S, Swedberg G, Macaden, Amarnath K, et al. (2005) Genotyping of methicillin-resistant Staphylococcus aureus strains from two hospitals in Bangalore, South India. J Clin Microbiol 43(7): 3198- 3202.
-
Oliveira C, Lencastre H (2002) Multiplex PCR strategy for rapid identification of structural types and variants of the mec Element in methicillin- resistant Staphylococci aureus. Antimicrob Agents Chemother 46(7): 2155- 2161.
-
Murakami K, Minamide W, Wada K, Nakamura E, Teraoka H, et al. (1991) Identification of Methicillin-resistant Strains of Staphylococci by polymerase chain reaction. J Clin Microbiol 29(10): 2240-2244.
-
De Neeling AJ, van Leeuwen WJ, Petit PL, Schouls LM, Schot CS, et al. (1998) Resistance of S. aureus in Netherland. surveillance by an electronic network during 1989-1995. J Antimicrob Chemother 41(1): 93- 110.
-
Ahmed O, Elmekki A, Omer E, Elhassan M (2014) Molecular detection of Methicillin resistant Staphylococcus aureus in patients with urinary tract infections in Khartoum State. Journal of Science and Technology 15: 1-8.
-
Olayinka O, Olayinka A, Obajuluwa A, Onaolapo J, Olurinola P (2009) Absence of mecA gene in methicillin- resistant Staphylococcus aureus isolates. African Journal of Infectious Diseases 3(2): 49-56.
-
Ba X, Harrison M, Edward F, Holden MT, Larsen AR, et al. (2014) Novel mutations in penicillin-binding protein genes in clinical Staphylococcus aureus isolates that are methicillin resistant on susceptibility testing, but lack the mec gene. J Antimicro Chemother 69(3): 594-597.
-
Wertheim F, Verbrugh A, Boelens A, Voss A, Vandenbroucke-Grauls CM, et al. (2004) Low prevalence of methicilin resistant Staphylococcus aureus at hospital admission in Netherland. The value of search and destroy and restrictive antibiotic use. J Hosp Infec 56(4): 321-325.
- Origin, Evolution, and Functional Impact of Short Insertion- Deletion Variants in Human Genomes: A Review
- Harnessing Molecular Glues for Next-Generation Vaccine, Cancer and Cardiovascular Disease Drug Development: A Comprehensive Review
- Lateral Cervical Epidermal Inclusion Cyst in a Paediatric Patient: A Rare Case Report
- Malarial Plasmodium Falciparum with Hepatitis B and C Virus Infections among Blood Donors in Ife Central Local Government Area, Ile Ife, Osun State, Nigeria
- Withanolides and Withaferin A- What’s next in Ashwagandha Research
- Designing of Dual Pulse Photoacoustic Tomography for Imaging of Drug-Response and Tumor Growth