Tryptophan Metabolism and its Relation with CKD Patients
Signs and symptoms of chronic kidney disease (CKD) are usually not present during early stages of disease. If diagnosed early, the progression of CKD could be slowed down. Finding an early diagnostic or predictive marker is of great benefit for both nephrologists as well as patients. Recent development in metabolomics has shown a potential progress in finding a novel biomarker to predict disease progression. In recent years, tryptophan (TRP) metabolites have shown a possible role in CKD pathogenesis and progression of disease. There are accumulations of toxic TRP metabolites in CKD. This review presents possible role of TRP metabolites in CKD. However, for defining their role as a predictive biomarker more and large cohort studies are required.
Introduction
Various serious and chronic conditions like, neurological diseases [1, 2, 3], psychiatric disorders [1, 4, 5, 6, 7, 8, 9], the early onset of cardiovascular disease (CVD) [10, 11, 12, 13, 14], chronic kidney disease (CKD) and even renal allograft rejections [15] are associated with inflammation, oxidative stress and tryptophan (TRP) metabolism. An increase in symptoms of anxiety, depression and decrease in cognitive functions are often followed by the progression of CKD to end stage renal disease (ESRD) [16, 17, 18]. Because there is a flap in between the psychological symptoms and the symptoms of uremia, these are less commonly diagnosed in CKD patients. The frequencies of the hospitalization affected by these symptoms are high and so, they play an important role in the disease progression and mortality rates [19]. Since oxidative stress and inflammation are already noticeable in the moderate stages of CKD, an early intervention is needed [20]. These factors strengthen the TRP metabolism via the kynurenine pathway (KYN).
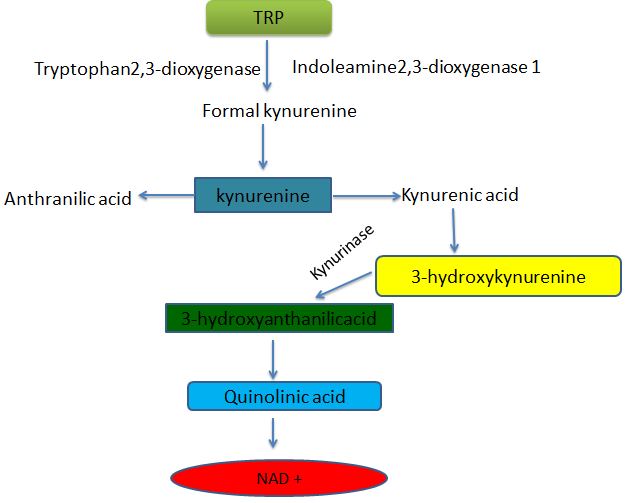
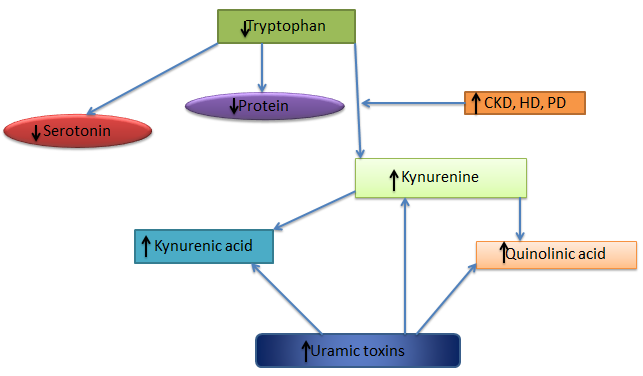
The synthesis of nictotinamide adenine dinucleotide (NAD) (Figure 1), a coenzyme essential for energy metabolism is carried out by an essential amino acid L-tryptophan (TRP) [21, 22]. Normally, the majority of free TRP (~95%) is metabolized forth the KYN pathway in the liver by the enzyme tryptophan 2,3-dioxygenase (TDO) which is highly expressed in the hepatic cells mostly controlled by TRP levels [23, 24, 25, 26]. In the case of inflammation such as chronic low-grade inflammation in old aged people or as in CKD (8) a significant translocation in KYN pathway occurs by an enzyme indoleamine 2,3-dioxygenase 1 (IDO1) mainly expressed extrahepatically induced by pro-inflammatory molecules particularly by the cytokine IFN-Ƴ promoting the production of a sensitive immune response marker neopterin [27]. Quinolinic acid (QA), 3-hydroxykynurenine and kynurenic acid (KYNA) etc. collectively called as kynurenines are eventually produced by KYN pathway and are normally eliminated via urinary excretion. Kynurenines play a vital role in controlling adaptive immunity and are involved in comorbid neuropsychiatric and atherosclerosis symptoms. Patients with CKD (Figure 2) are at high risk of KYN-related pathophysiologies [28]. TRP metabolites may trigger fatigue and promote atherosclerosis in CKD patients by activating oxidative stress and leukocyte activation in endothelial and vascular smooth muscle cells [29]. Hence, in this update article we tried to explain the role of TRP metabolites as predictive markers in patients with CKD.
Discussion
Recent studies on TRP and KYN pathway in hemodialysis (HD) and peritoneal dialysis (PD) has shown a promising aspect of using TRP metabolites as inflammatory markers in CKD patients. Study conducted by Bipath Priyesh and Vijoen Margaretha suggested the significant role of TRP in ESRD. They showed the depletion of tryptophan and accumulation of kynurenine and quinolinic acid in the blood of HD patients [30]. Subrata Debnath, et al. concluded that CKD secondary to diabetes mellitus (DM) type 2 may be associated with accumulation of toxic TRP metabolites because of both impaired kidney function and inflammation. They highlighted the need for future studies with large cohort of patients to determine the accumulation of KYN directly contributes to progression of CKD and associated symptoms in DM type 2 patients [31]. Mutsaers, et al. reported that there is a direct connection between TRP metabolism and the circadian rhythm in patients with CKD. They concluded that altered tryptophan metabolism is considered an etiology for CKD- associated fatigue [29]. Studying the tryptophan metabolism and its relation to psychological and cognitive functioning in CKD disease Naam Karu, et al. found the association of indole 3 acetic acid and psychological measures as novel findings [32]. Kato A and his group studied the association of TRP metabolites with atherosclerotic parameters in HD patients. The study included 243 HD patients and it was found that TRP metabolites increases with time on HD, and is associated with advanced atherosclerotic changes in chronic HD patients [33]. In a study conducted on 20 PD, 19 HD and 21 kidney transplant patients by Nigar Yilmaz, et al. showed increased (IDO) levels compared to the control group. The concentration of kynurenine was significantly increased in the PD group compared to the other groups while oxidative stress was found to be related to IDO activity and was most increased in the patients on PD [34].
Symptoms of CKD are normally not visible during early stages. Significant loss of the kidney function is the first obvious sign of the kidney disease. If diagnosed in the very beginning, the progression of CKD can be controlled hence reducing the complications. The systematic review of metabolites like, amino acids, sugars, organic acids, etc. in biologic fluids or samples can be used as predictive biomarkers, generally termed as metabolomics or metabolite profiling [35]. In clinical research the value of metabolite profiling could be achieved when applied to large cohorts. This can be enhanced by assessment of the association of baseline metabolite levels with renal outcomes.
The longitudinal association of baseline levels of 217 metabolites with incident of CKD in eight years and over in 1434 participants were described in the Framingham Heart Study (FHS) [36]. Similarly Goek, et al. investigated longitudinal associations of baseline values of 140 metabolites over seven years in 1017 individuals in the KORA study [37]. Both of the studies identified markers of TRP metabolism are associated with the occurrence of CKD [38, 39, 40]. A total of 123 individuals in the FHS study and 106 individuals in the KORA study developed new-onset CKD. In both of the studies, kynurenine/tryptophan ratio was strongly associated with CKD risk, with an odds ratio (OR) of 1.36 per SD (p: 0.003, 95% confidence interval [95%CI], 1.11 to 1.66) after adjusting for eGFR and other CKD risk factors. Whereas in the FSH study, authors highlighted that KYN (OR per + 1 SD, 1.49; p<0.001, 95% CI, 1.25to 1.88) were related to the high risk of future CKD. These findings showed TRP metabolites can serve as predictive marker for incident CKD risk.
Conclusion
Healthy kidneys are important in TRP metabolism and TRP metabolites are eliminated in the urine. In diseased kidneys there are building up of several toxic metabolites including kynurenines collectively called as protein bound uremic toxins. Due to low TRP levels and accumulation of toxic metabolites patients on dialysis experience depression, sleep disturbances, anxiety, impaired cognitive function and other symptoms and complications. A large number of studies have shown the involvement of TRP metabolism in CKD. There is a need of large cohort study to prove its critical role in disease progression and as predictive biomarker.
References
-
Stone TW, Darlington LG (2013) The kynurenine pathway as a therapeutic target in cognitive and neurodegenerative disorders. Br J Pharmacol 169(6): 1211-1227.
-
Campbell BM, Charych E, Lee AW, Moller T (2014) Kynurenines in CNS disease: regulation by inflammatory cytokines. Front Neurosci 8: 12.
-
Heyes MP, Saito K, Crowley JS, Davis LE, Demitrack MA, et al. (1992) Quinolinic acid and kynurenine pathway metabolism in inflammatory and non-inflammatory neurological disease. Brain 115: 1249-1273.
-
Maes M, Leonard BE, Myint AM, Kubera M, Verkerk R (2011) The new ‘5-HT’ hypothesis of depression: cell- mediated immune activation induces indoleamine 2,3-dioxygenase, which leads to lower plasma tryptophan and an increased synthesis of detrimental tryptophan catabolites (TRYCATs), both of which contribute to the onset of depression. Prog Neuropsychopharmacol Biol Psychiatry 35(3): 702-721.
-
Myint AM, Kim YK (2014) Network beyond IDO in psychiatric disorders: revisiting neurodegeneration hypothesis. Prog Neuropsychopharmacol Biol Psychiatry 48: 304-313.
-
Oxenkrug G (2013) Serotonin-kynurenine hypothesis of depression: historical overview and recent developments. Curr Drug Targets 14(5): 514-521.
-
Dantzer R, O Connor JC, Lawson MA, Kelley KW (2011) Inflammation-associated depression: from serotonin to kynurenine. Psychoneuroendocrinology 36(3): 426-436.
-
Christmas DM, Potokar J, Davies SJ (2011) A biological pathway linking inflammation and depression: activation of indoleamine 2,3-dioxygenase.Neuropsychiatr Dis Treat 7: 431-439.
-
Capuron L, Schroecksnadel S, Feart C, Aubert A, Higueret D, et al. (2011) Chronic low-grade inflammation in elderly persons is associated with altered tryptophan and tyrosine metabolism: role in neuropsychiatric symptoms. Biol Psychiatry 70(2): 175-182.
-
Pawlak K, Domaniewski T, Mysliwiec M, Pawlak D (2009) The kynurenines are associated with oxidative stress, inflammation and the prevalence of cardiovascular disease in patients with end-stage renal disease. Atherosclerosis 204(1): 309-314.
-
Koenig P, Nagl C, Neurauter G, Schennach H, Brandacher G, et al. (2010) Enhanced degradation of tryptophan in patients on hemodialysis. Clin Nephrol 74(6): 465-470.
-
Saito K, Fujigaki S, Heyes MP, Shibata K, Takemura M, et al. (2000) Mechanism of increases in L-kynurenine and quinolinic acid in renal insufficiency. Am J Physiol Renal Physiol 279(3): 565-572.
-
Sallee M, Dou L, Cerini C, Poitevin S, Brunet P, et al. (2014) The aryl hydrocarbon receptor-activating effect of uremic toxins from tryptophan metabolism: a new concept to understand cardiovascular complications of chronic kidney disease. Toxins (Basel) 6(3): 934-949.
-
Pawlak D, Pawlak K, Malyszko J, Mysliwiec M, Buczko W (2001) Accumulation of toxic products degradation of kynurenine in hemodialyzed patients. Int Urol Nephrol 33(2): 399-404.
-
Brandacher G, Cakar F, Winkler C, Schneeberger S, Obrist P, et al. (2007) Non-invasive monitoring of kidney allograft rejection through IDO metabolism evaluation. Kidney Int 71(1): 60-67.
-
Kimmel PL, Cukor D, Cohen SD, Peterson RA (2007) Depression in end-stage renal disease patients: a critical review. Adv Chronic Kidney Dis 14(4): 328-334.
-
Hermann DM, Kribben A, Bruck H (2014) Cognitive impairment in chronic kidney disease: clinical findings, risk factors and consequences for patient care. J Neural Transm 121(6): 627-632.
-
McKercher C, Sanderson K, Jose MD (2013) Psychosocial factors in people with chronic kidney disease prior to renal replacement therapy. Nephrology 18(9): 585-591.
-
Weisbord SD, Mor MK, Sevick MA, Shields AM, Rollman BL, et al. (2014) Associations of depressive symptoms and pain with dialysis adherence, health resource utilization, and mortality in patients receiving chronic hemodialysis. Clin J Am Soc Nephrol 9(9): 1594-1602.
-
Oberg BP, McMenamin E, Lucas FL, McMonagle E, Morrow J, et al. (2004) Increased prevalence of oxidant stress and inflammation in patients with moderate to severe chronic kidney disease. Kidney Int 65(3): 1009- 1016.
-
Richard DM, Dawes MA, Mathias CW, Acheson A, Hill-Kapturczak N, et al. (2009) L-tryptophan: basic metabolic functions, behavioral research and therapeutic indications. Int J Tryptophan Res 2: 45-60.
-
Sainio EL, Pulkki K, Young SN (1996) L-tryptophan: biochemical, nutritional and pharmacological aspects. Amino Acids 10(1): 21-47.
-
O Connor JC, Lawson MA, Andre C, Moreau M, Lestage J, et al. (2009) Lipopolysaccharide-induced depressive- like behavior is mediated by indoleamine 2,3-dioxygenase activation in mice. Mol Psychiatry 14(5): 511-522.
-
Byrne GI, Lehmann LK, Kirschbaum JG, Borden EC, Lee CM, et al. (1986) Induction of tryptophan degradation in vitro and in vivo: a gamma-interferon-stimulated activity. J Interferon Res 6(4): 389-396.
-
Werner Felmayer G, Werner ER, Fuchs D, Hausen A, Reibnegger G, et al. (1991) Induction of indoleamine 2,3-dioxygenase in human cells in vitro. Adv Exp Med Biol 294: 505-509.
-
Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, et al. (1999) A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. modification of diet in renal disease study group. Ann Intern Med 130(6): 461-470.
-
Taylor MW, Feng GS (1991) Relationship between interferon-gamma, indoleamine 2,3-dioxygenase, and tryptophan catabolism. FASEB J 5(11): 2516-2522.
-
Moffett JR, Namboodiri MA (2003) Tryptophan and the immune response. Immunol Cell Biol 81(4): 247-265.
-
Mutsaers HA, Masereeuw R, Olinga P (2014) Altered tryptophan metabolism and CKD-associated fatigue. Kidney Int 86(5): 1061-1062.
-
Priyesh B, Margaretha V (2010) Tryptophan and kyunurenine pathway in haemodialysis and peritoneal dialysis. Biomedical Research 21(3): 315-320.
-
Debnath S, Velagapudi C, Redus L, Thameem F, Kasinath B, Hura CE, et al. (2017) Tryptophan Metabolism in Patients With chronic Kidney Disease Secondary to Type 2 Diabetes: Relationship to Inflammatory Markers. Int J Tryptophan Res 10: 1-9.
-
Karu N, Mckercher C, Nichols D, Davies N, Shellie RA, et al. (2016) Tryptophan metabolism, its relation to inflammation and stress markers and association with psychological and cognitive functioning: Tasmania chronic kidney disease pilot study. BMC Nephrol 17(1): 171.
-
Kato A, Suzuki Y, Suda T, Suzuki M, Fujie M, et al. (2010) Relationship between an increased serum kynurenine/ tryptophan ratio and atherosclerotic parameters in hemodialysis patients. Hemodial Int 14(4): 418-424.
-
Yilmaz N, Ustundag Y, Kivrak S, Kahvecioglu S, Celik H, et al. (2016) Serum indoeamine 2,3 dioxygenase and tryptophan and kynurenine ratio using the UPLC-MS/ MS method, in patients undergoing peritoneal dialysis, hemodialysis, and kidney transplantation. Ren Fail 38(8): 1300-1309.
-
Rhee EP, Feldman HI (2014) Metabolite markers of incident CKD risk. Clin J Am Soc Nephrol 9(8): 1344- 1346.
-
Rhee EP, Clish CB, Ghorbani A, Larson MG, Elmariah S, et al. (2013) A combined epidemiologic and metabolomics approach improves CKD prediction. J Am Soc Nephrol 24(8): 1330-1338.
-
Goek ON, Prehn C, Sekula P, Romisch Margl W, Doring A, et al. (2013) Metabolites associate with kidney function decline and incident chronic kidney disease in the general population. Nephrol Dial Transplant 28(8): 2131-2138.
-
Wang Y, Liu H, McKenzie G, Witting PK, Stasch JP, et al. (2010) Kynurenine is an endothelium-derived relaxing factor produced during inflammation. Nat Med 16(3): 279-285.
-
Holmes EW (1988) Determination of serum kynurenine and hepatic tryptophan dioxygenase activity by high liquid chromatography. Anal Biochem 172(2): 518-525.
-
Mason M (1974) Effects of calcium ions and quinolinic acid on rat kidney mitochondrial kynurenine aminotransferase. Biochem Biophys Res Commun 60(1): 64-69.
- Origin, Evolution, and Functional Impact of Short Insertion- Deletion Variants in Human Genomes: A Review
- Harnessing Molecular Glues for Next-Generation Vaccine, Cancer and Cardiovascular Disease Drug Development: A Comprehensive Review
- Lateral Cervical Epidermal Inclusion Cyst in a Paediatric Patient: A Rare Case Report
- Malarial Plasmodium Falciparum with Hepatitis B and C Virus Infections among Blood Donors in Ife Central Local Government Area, Ile Ife, Osun State, Nigeria
- Withanolides and Withaferin A- What’s next in Ashwagandha Research
- Designing of Dual Pulse Photoacoustic Tomography for Imaging of Drug-Response and Tumor Growth