A Comprehensive SSA Report Current Status of Cancer Control in Belize
Background: Belizeans have been severely affected by cancer, noted by the rising mortality rates. Health disparities, health inequities and issues with systemic health access are some of the pre-existing problems. One of the significant issues in small countries is often the downplay of cancer control and the lack of a cancer continuum of care through a national cancer control plan. It has been estimated that over 80% of countries have developed national cancer control plans. However, the central issue that presented a significant barrier was the successful launch of implementing the plan. There is a great need to assess and evaluate those implementation barriers to overcome this impediment. Objective: 1. To determine what critical government plans and policies are in place to gear towards the country’s specific barriers to reducing cancer incidence. An assessment of the latter was conducted. 2. To determine whether the multisectoral approach was present within Belize’s governance structure for cancer control. Methodology: With the use of 2 approaches that were complementary to each other. 1st Approach: Questionnaire-grid: ‘snap-shot’ of the government responses to cancer in Belize. 2nd Approach: EOH’S APPROACH TO STAKEHOLDER ENGAGEMENT Detailed Case Study: Policy response to cancer explored via in-depth, semi-structured interviews EOH’S approach includes: 1. An inclusive approach 2. Materiality 3. Responding Interviews were conducted with key informants from a range of backgrounds: 1. Representatives of the private sectors 2. Specialists 3. Public sectors 3rd Approach: Archival Research to identify prior and current policy documents throughout the years within the MOHW. Together these approaches were cross-linked to enable a detailed analysis of formulated policy and mechanism of assessment of what type of cancer control/surveillance is being used in the delivery of health care for cancer in Belize. In addition, toevaluate if all policies were implemented and successfully launched. This will help to avoid redundancies in cancer control planning and to accelerate the process of launching respective cancer control mechanisms in Belize. Results: This article finds that twenty different types of plans and policies were found in efforts to contribute toward NCD control. Nevertheless, very few policies directly target cancer mortality and morbidity in Belize. There seem to have been issued in implementing these policies(failure to launch successfully) and some procedures that were not explicitly addressing the root issues of the prevalence of cancer. No cancer surveillance system was activated to measure the progress of all Belizeans with cancer. Thus, this is because no national cancer registry was functionally started to capture the various modalities, variables and risk factors of cancer. Conclusion: This stakeholder and situational analysis highlight the disparities in Belize’s healthcare system that disproportionately impacts Belizeans once diagnosed with cancer. This article elucidates the perspective of Belize’s national response to cancer. It highlights the deficiencies or barriers that inhibit successful cancer mitigation—recognizing a great need for cancer control mitigation in Belize through NCCP that provides a continuum of care. To address the country-specific cancer burden, reliable, evidence-based data is needed. Cancer surveillance is the most efficient way of achieving optimum cancer management in the delivery of the cancer healthcare system in Belize.
Background Information
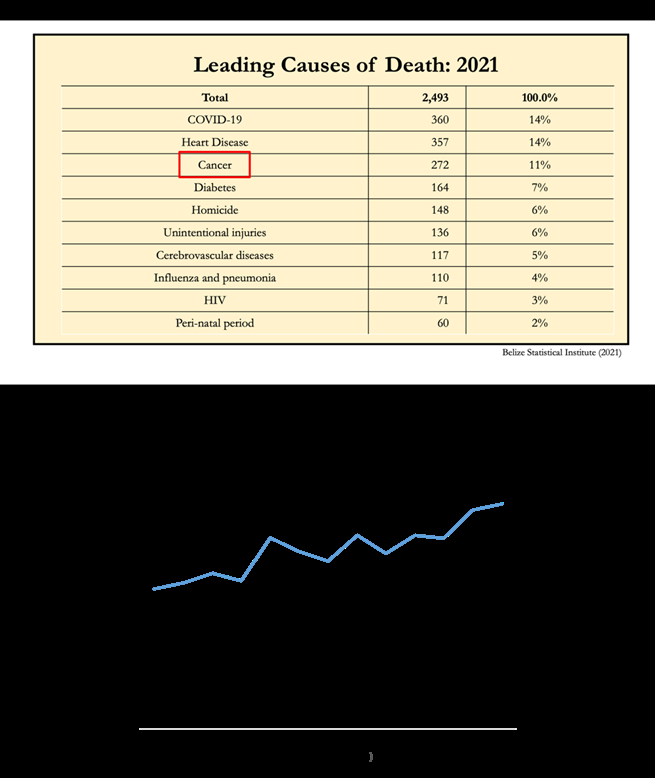
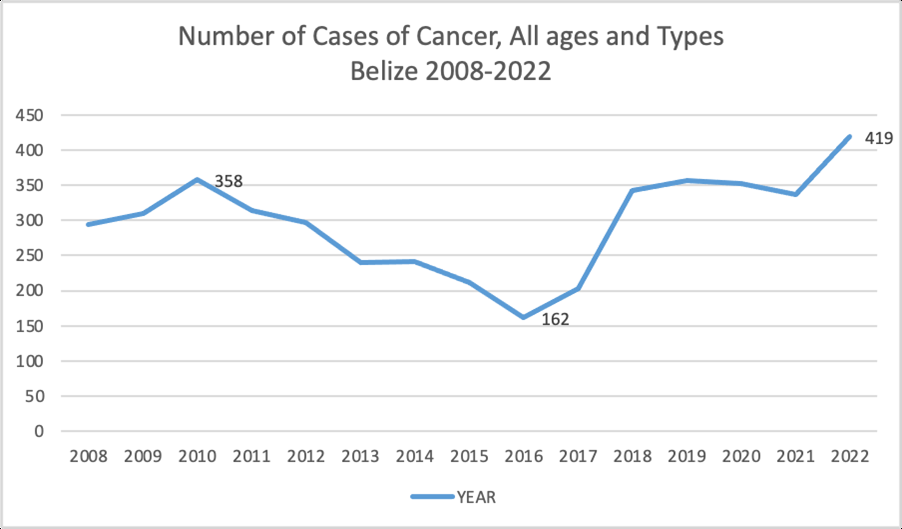
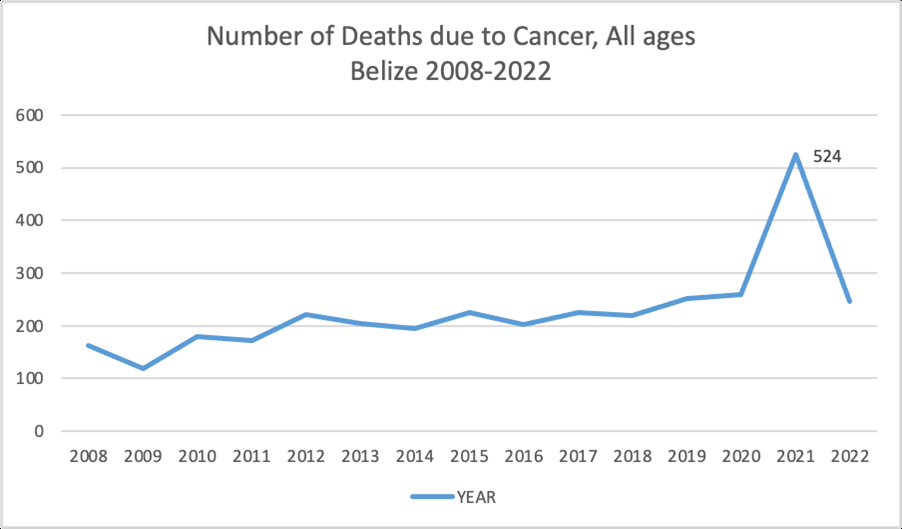
Cancer is one of the four top NCDs that continues to increase in incidence rate and mortality rates have plummeted [1]. Cancer is not the only problem in developed nations but also in the developing world, where cancer control can be overburdened [2]. In Belize, as seen in Figure
1, cancer mortality rates in Belize have been increasing throughout the years. There is a great need to have cancer control in Belize. With the steady rise in cancer mortality, there needs to be an acceleration of mitigating this pressing burden in Belize.
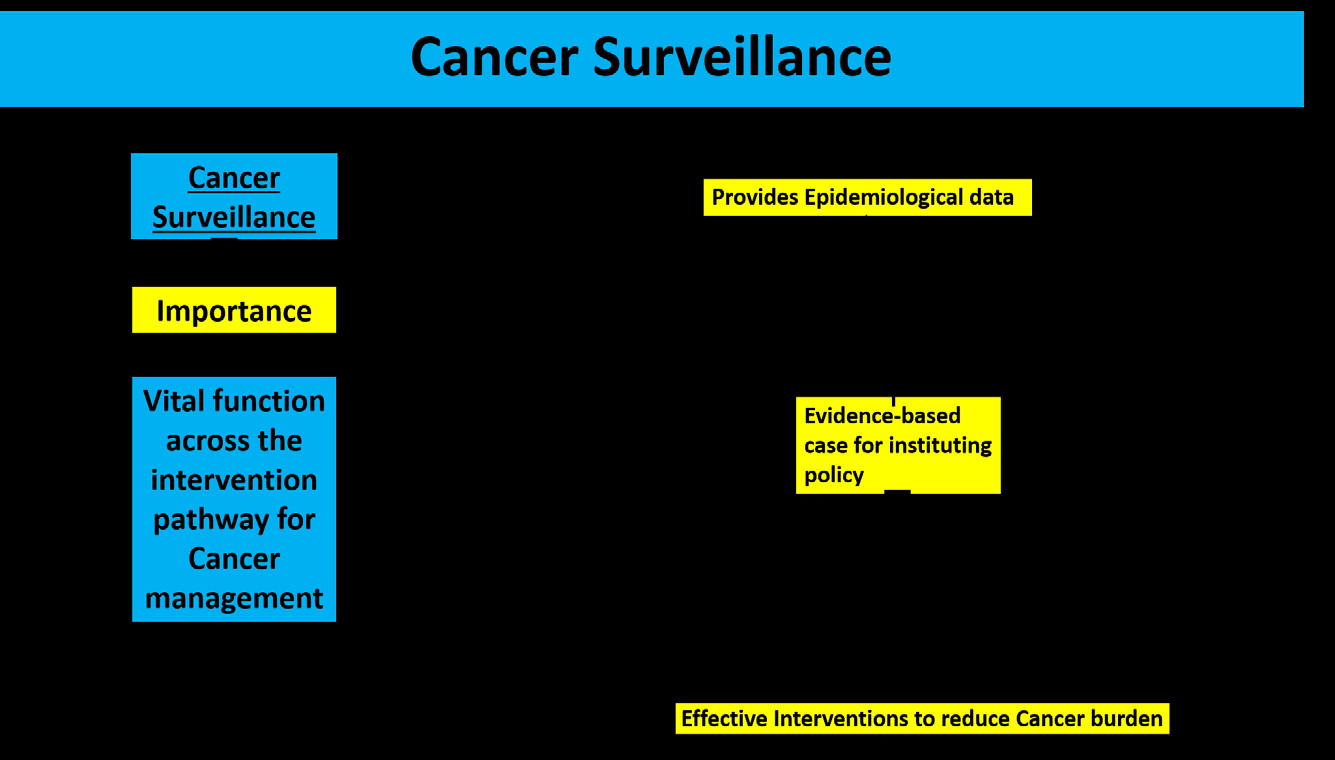
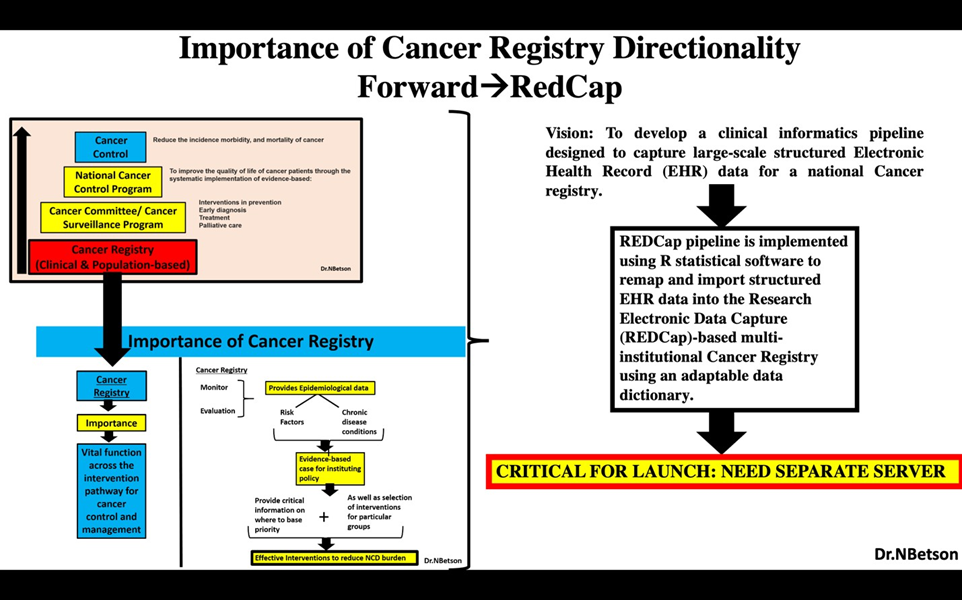
In small Caribbean islands, one of the major issues in cancer control is the downplay of the issue, or often, it is overlooked [3]. A critical component to avoid the downplay of cancer control is fortified cancer surveillance [4]. There are two crucial components of Cancer Surveillance: monitoring and evaluation [5]. Cancer surveillance is the most efficient way of achieving optimum cancer management in the delivery of the cancer healthcare system in Belize. Cancer Surveillance provides the epidemiological framework and evidence-based data for instituting policies to mitigate the cancer burden [6]. The evidence-based data gathered from cancer surveillance can provide critical information on where to base priority as well as a selection of interventions for particular groups (Figure 2). One of the prominent contributing factors that cause the increase in mortality rates of cancer in Belize is that the majority of the cases are diagnosed in the late stages when metastasis has occurred. If cancers are diagnosed early enough before metastasis occurs, the mortality rates can significantly decrease via treatment options such as [7]:
- Surgically removing mass
- Chemotherapy
- Radiation therapy
- Shrinkage of the cancer cells Consequently, this is why cancer surveillance in Belize is very fundamental.
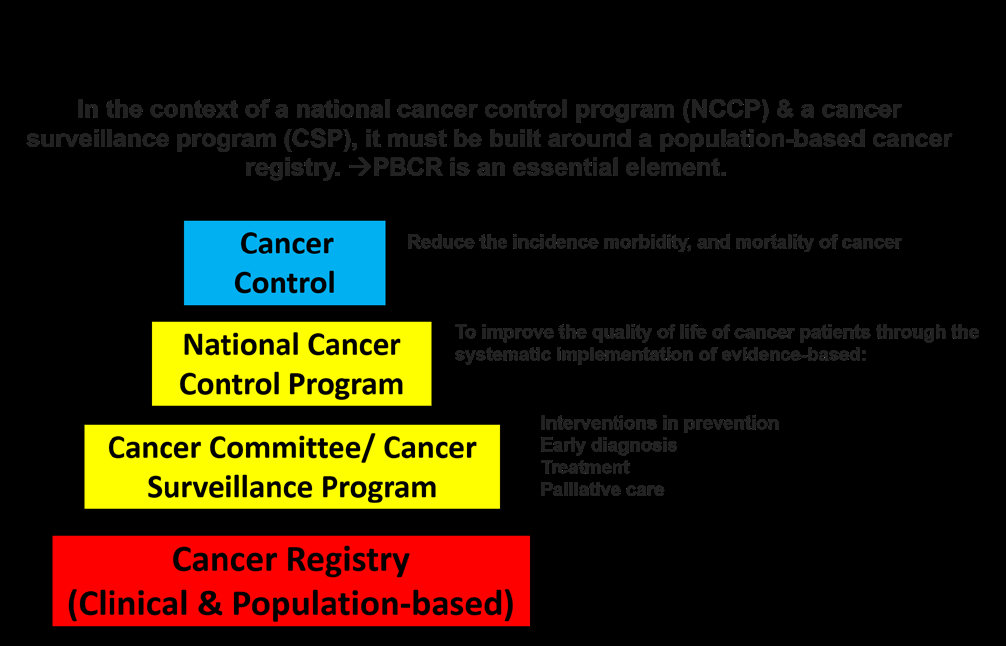
In addition, cancer surveillance will allow policymakers to intervene directly in the most vulnerable populations and communities within Belize via preventative methodologies. The development and implementation of cancer surveillance are only possible through having cancer registries: HBCR (hospital-based) and PBCR (population-based) [8]. Cancer registries, PBCR is the foundation to pivot any form of the cancer control unit [9]. PBCR is an essential element in the formulation of the following:
- Budget (Financing the delivery of care for cancer)
- Data Collection on Incident Cases, Mortality Cases, and sampling frame with geographic distribution on Morbidity Cases.
- Intervention Strategies
- Preventative Strategies
- Cancer Committee
- National Cancer Control Program
- Patient Care Programs and provide vital clinical variables
- Administrative Programs
- Cancer Research Programs Consequently, based on the last line of actions in Figure 3, PBCR is the foundation or the nucleus that allows all cancer control programs to function effectively.
PBCR will be able to geographically track all cancers in pre- defined areas, providing a better perspective on the incidence of cancers and where to intervene precisely. Thus, this will allow public health officials and policymakers to mitigate the cancer risk in Belize efficiently. It will give an evidence-based mechanism of assessment that will allow for an effective cancer control plan and monitoring of cancer incidence in Belize. In addition, PBCR will allow for generating those cross-talk mechanisms, risk factors correlation, proper health promotion, transparency in financial needs as it pertains to health care delivery for cancer, expose treatment deficiencies and determine intervention strategic strategies [9].
Active Governance and Leadership in Cancer Control
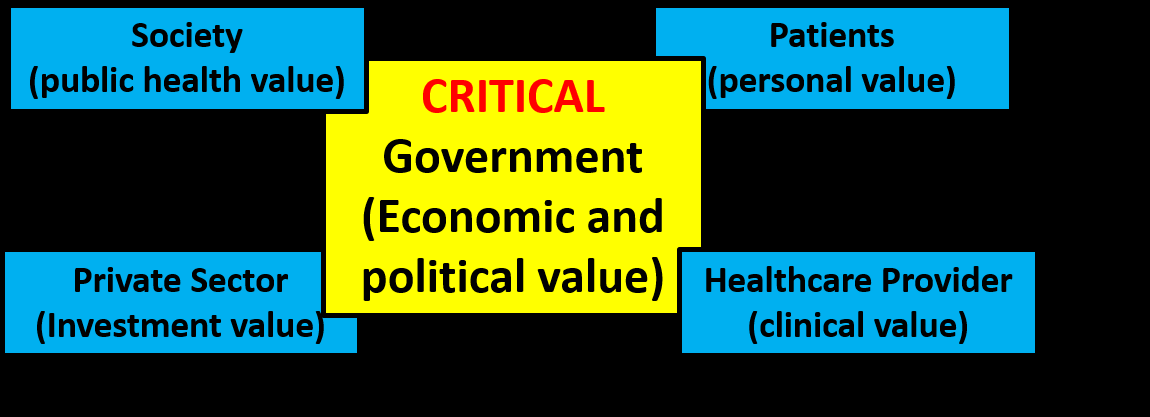
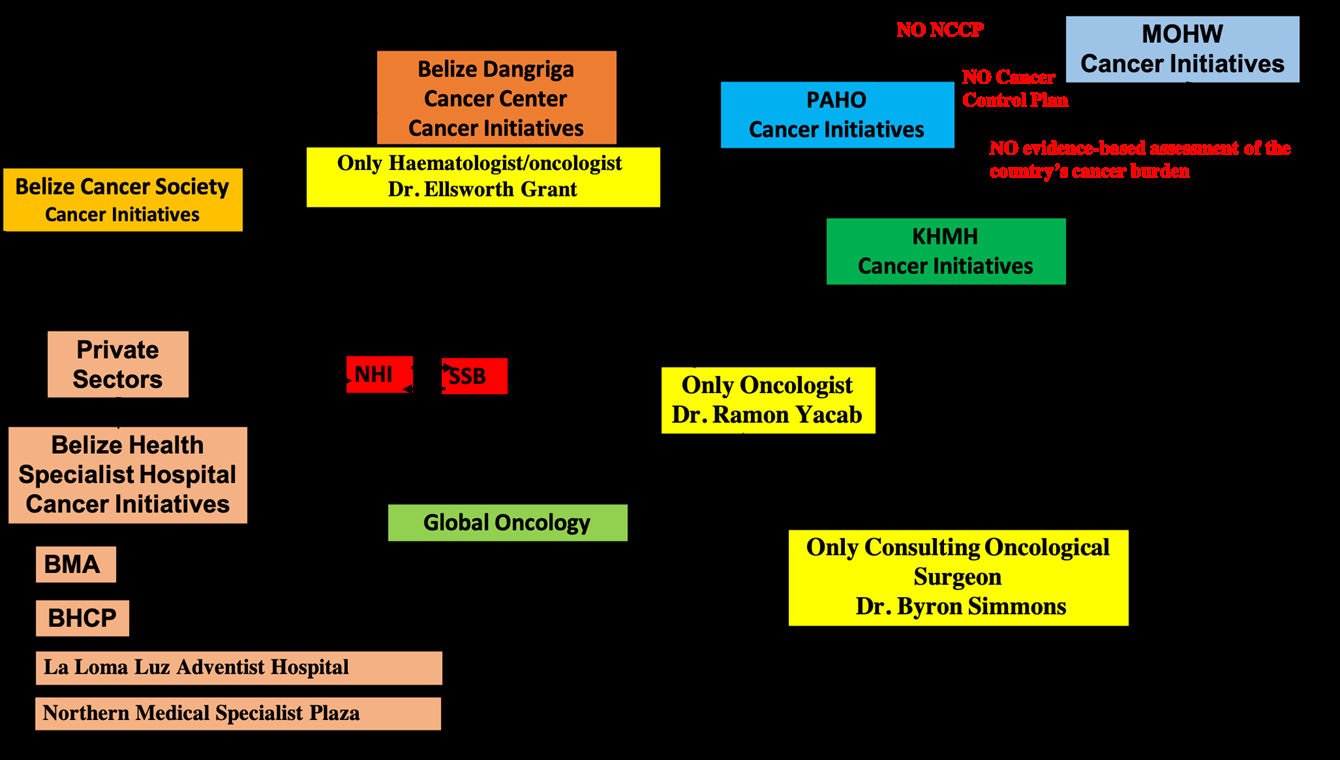
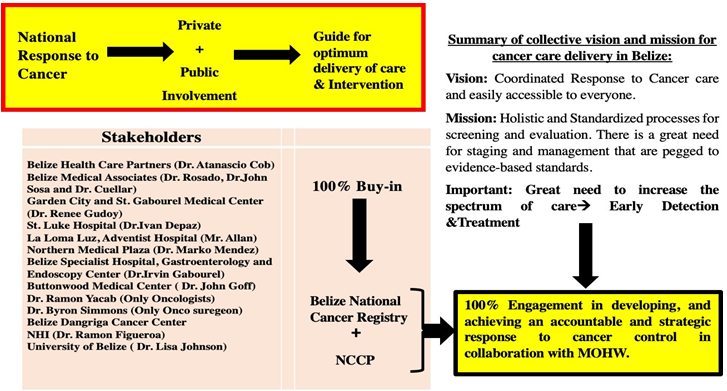
To achieve full success in Cancer Control, the government must be the central driving force and nucleus of the cross- talk between all vital stakeholders in mitigating cancer [10]. It is the role of the government to be actively involved in orchestrating joint and multisectoral collaboration to devise specific strategic planning to directly address the barriers and gaps in cancer control in Belize (Figure 4). Each stakeholder brings a different perspective on the critical value system in cancer control [11, 12]. For illustration:
- Government brings economic and political value.
- Society brings public health values.
- The private sector brings investment value.
- Patients bring that personal value.
- Health Provider brings that clinical value.
The Rationale of the SSA
There was a great need to understand better the value and logistical frameworks in developing and launching the national PBCR in Belize. In addition, it is imperative to know the mechanism of action embedded in a cohesive system for delivering health care concerning cancer in Belize. It is imperative to gain insights and assessments from all stakeholders who directly engage in delivering the cancer health system in Belize. Essential questions in this determination are:
- Who are the different private sector stakeholders and NGOs?
- What are the relevant health sector planning and care delivery for cancer patients?
- What are their potential and active contributions to the country’s health system?
- What are the available policy options for engaging them to achieve national health goals?
- What are the assessment mechanisms for the optimum delivery of health cancer care?
- What is the involvement or cross-talk mechanism that the government has with the public health, cancer patients, private sector and health care provider?
Three significant steps are imperative in understanding the mechanism of cancer control with policies implemented in Belize to mitigate the rise in cancer. First, knowing the steps in cancer control planning, the various engagement opportunities, and mapping stakeholders by understanding the who, when, and how. Thirdly, getting a full grasp of the coordinated implementation fosters opportunities for meaningful partnerships. Fourth, how involved is the government in all this propriety of cancer control within the delivery of the health care system in Belize?
Aims and Methodology
Aim
1. To determine what critical government plans and policies are in place to gear towards the country’s specific barriers to reducing cancer incidence. An assessment of the latter was conducted. 2. To determine whether the multisectoral approach was present within Belize’s governance structure for cancer control.
Methodology
With the use of 2 approaches that were complementary to each other. 1st Approach: Questionnaire-grid: ‘snap-shot’ of the government responses to cancer in Belize. 2nd Approach: EOH’S Approach to Stakeholder Engagement Detailed Case Study: Policy response to cancer explored via in-depth, semi-structured interviews EOH’S approach includes:
- An inclusive approach
- Materiality
- Responding Interviews were conducted with key informants from a range of backgrounds:
- Representatives of the private sectors
- Specialists
- Public sectors 3rd Approach: Archival Research to identify prior and current policy documents throughout the years within the MOHW.
Together these approaches were cross-linked to enable a detailed analysis of formulated policy and mechanism of assessment of what type of cancer control/surveillance is being used in the delivery of health care for cancer in Belize. In addition to evaluate if all policies were implemented and successfully launched. This will help to avoid redundancies
Results/Findings
in cancer control planning and to accelerate the process of launching respective cancer control mechanisms in Belize. This SSA will give a better perspective of the national response to cancer in Belize and highlight the deficiencies or barriers that inhibit successful cancer mitigation (Figure 5). The federal response ideally is composed of five components to consider, such as:
- Barriers and Facilitators to policy success
- Multisectoral
- Health Promotion
- Risk Factors
- Healthcare
- Surveillance
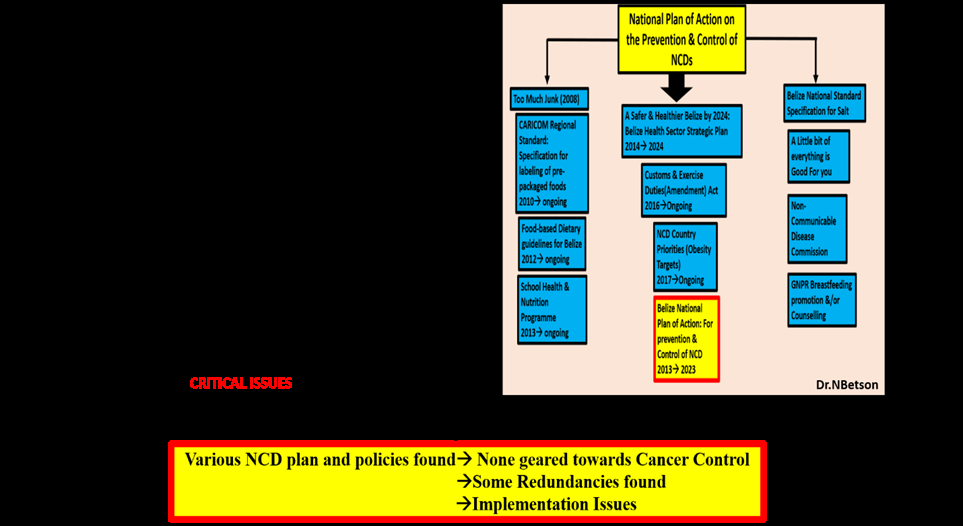
After Archival Research was conducted, it was highlighted that approximately twenty different types of plans and policies were found in efforts to contribute toward NCD control. Nevertheless, very few policies directly target cancer mortality and morbidity in Belize. There seem to have been issued in implementing these policies (failure to launch successfully) and some procedures that were not explicitly addressing the root issues of the prevalence of cancer (Table 1).
One of the prominent issues that were found:
- Adopting plans or policies intended for another country that did not address or fit the needs specifically of Belize pertains to barriers in delivering health care for cancer control.
- Redundancies in health plans and policies.
- Prominent duplication in policies and efforts towards cancer control.
- Disjointed and fragmented plans, policies and action towards cancer control.
- Lack of communication and multisectoral approach in planning for cancer control.
- Plans and Policies were not easily accessible or available.
| Multisectorality | Risk Factors |
|---|---|
| 1. Collaboration is needed in wide society and with government 2. By having whole-of-society partnerships with the NGOs and Private sector being given a ‘seat at a table’ to make central cancer response. 3. Bigger Barriers -> Lack of high level political will and cohesive response. Other actors worked in silos. | Host of barriers of actions to address risk factors of cancer: 1. Awareness of health eating in the population increase. Increase availability of nutrition-poor fast food concern and poor lifestyle choices that increase risk of cancer. 2. Most pressing issues for policy makes were: -> Procurement of Medication -> Chemotherapeutic drugs, Morphine, Pain Killers etc. -> Human Resources -> Shortage of specialized doctors. -> Increase in referrals -> Lack of financial support and Budget in the line of action for cancer control. |
| Heath Promotion | Health Care |
| 1. Multiple barriers like aforementioned limited resources. 2. Lack of designated focal point -> Have impeded health promotion initiatives. | 1. Insufficient emphasis on cancer prevention efforts in primary care. 2. Too much attention paid for the tertiary and medical technologies. 3. Delivery care in the rural area does not match urban centers. 4. Specialized treatment is an huge challenge with limited HR available. 5. While most stakeholders are aware of the treatment guidelines -> actual use of such guidelines is unknown. |
| Surveillance | |
| 1. Stakeholders highlighted the need for establishment of CR. 2. Lack pf HR and skills at MOHW, NGO partners and Private Sectors -> to undertake epidemilogical or evaluation research. 3. Building local capacity rather than relying on private external consultancies. |
This Table 1 was devised based on the preliminary plans and policies from the National NCD response and policies geared towards cancer control. Many obstacles were found, such as a decrease in the Multisectoral approach, a reduction in Health promotion, a surveillance system for Cancer being absent, Risk Factors for Cancer not being highlighted through evidence-based capture, and overall healthcare delivery for cancer control that was not optimal (Figure 6).
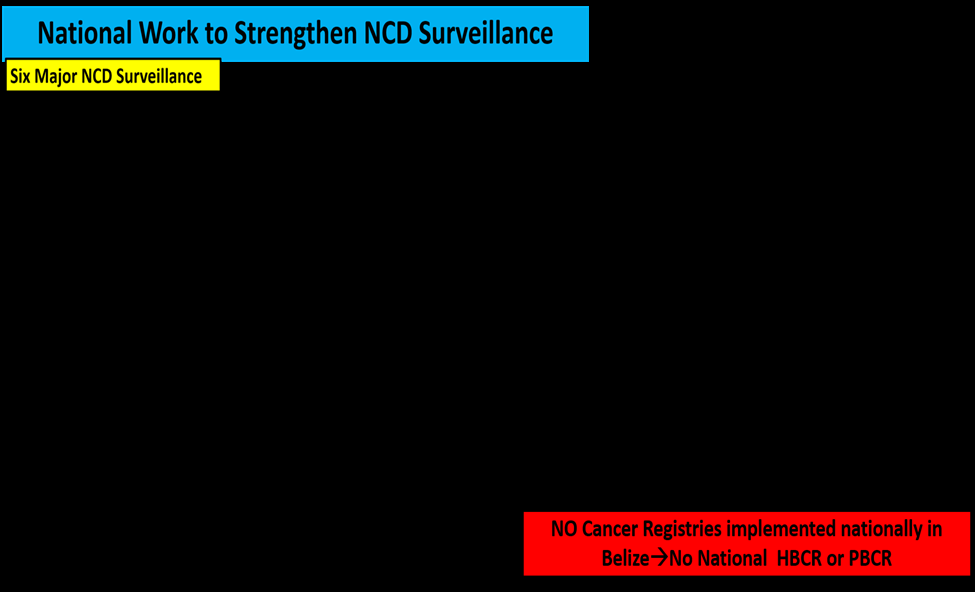
Six major NCD surveillances were found where some data could be retrieved. Through the BHIS, mortality (cancer deaths) was available. However, there is no systematic collection and analysis of information on the:
- Incidence rates
- Extent of diseases
- Screening tests
- Treatment
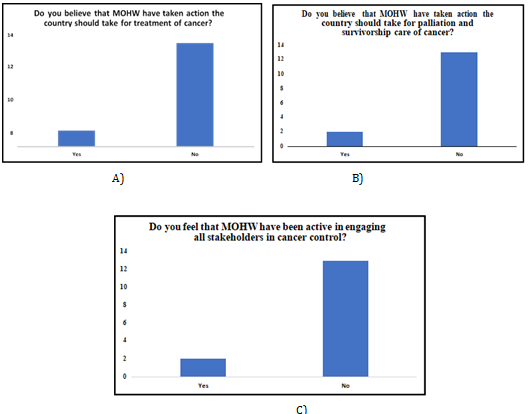
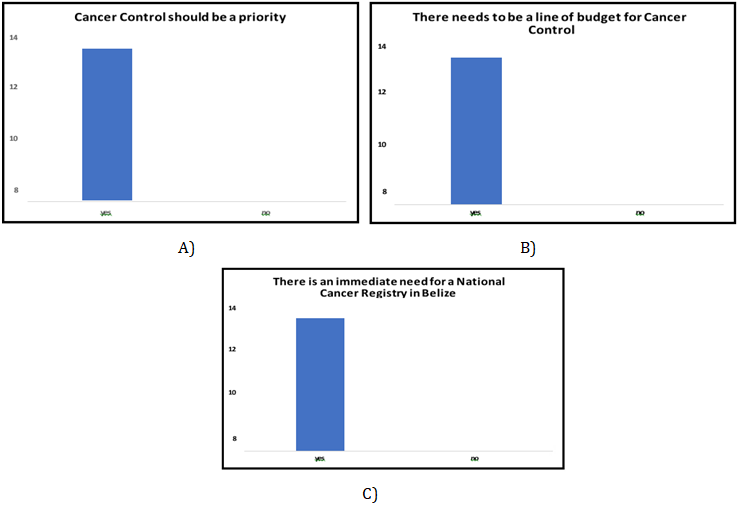
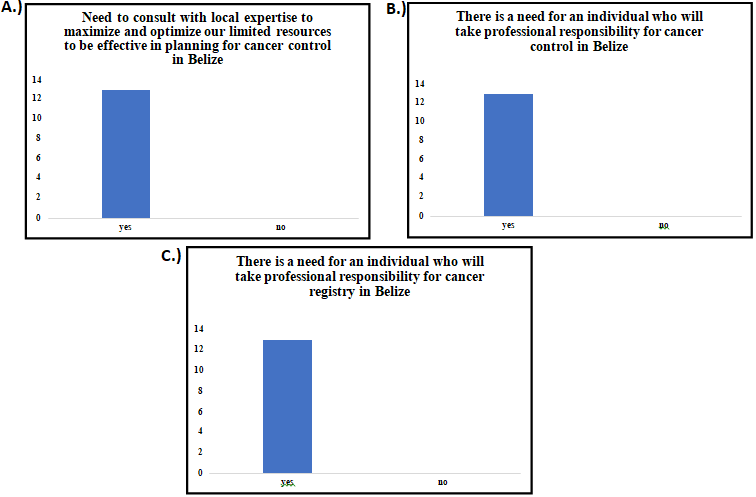
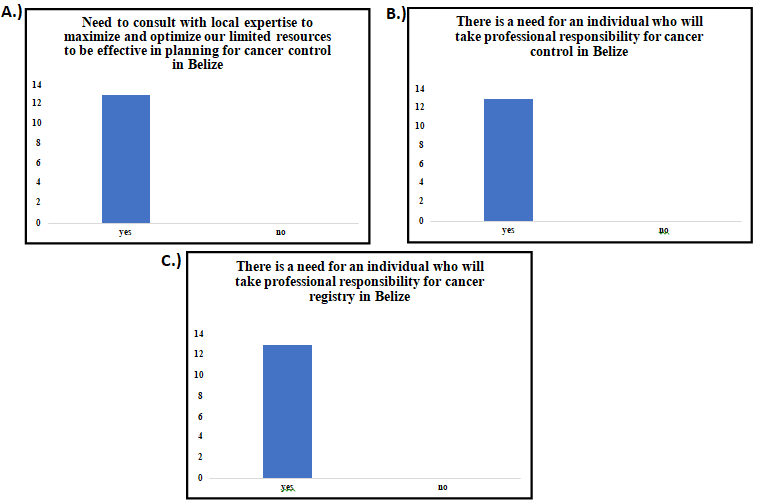
No cancer surveillance system was activated to measure the progress of all Belizeans with cancer. Thus, this is because no national cancer registry was functionally started to capture the various modalities, variables and risk factors of cancer. This is a major contributing factor to why cancer treatment is a significant challenge, the driving actions are not highlighted, and cancer prevention is low (Figures 7-13).
Discussion
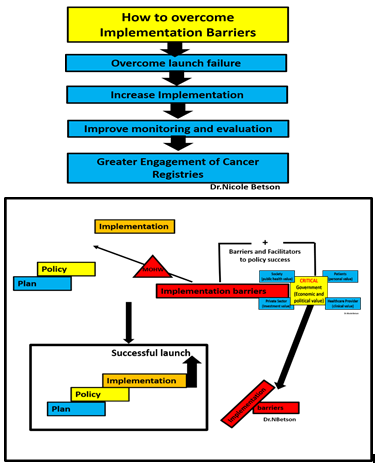
One of the main findings from the SSA that presented a fundamental challenge was the implementation barriers in every policy. These implementation barriers have many contextual determinants that can be challenging to identify and strategically address. Nevertheless, five primary implementation barriers were placed in the failure to launch the development of plans and policies throughout the years. These five primary implementation barriers are Inadequate human and financial resources, lack of clarity on operational guidelines, roles or responsibilities, conflicts with other policies, political will and Social/ behavioural resistance. The latter had significant implications on the “Barriers &
Facilitators to Policy Success”, which contributed to the unsuccessful implementation of the policies (Figure 14). Also, after assessing all the procedures, none were present that directly targeted cancer control. There was no financial budget that was attached for cancer control. Thus, it is critical to have a line of budget attached to any plan to have a successful implementation.

A Deeper Understanding and Breakdown of the Implementation Barriers
Belize is not the only country with a problem with implementation issues. Internationally this has been very ubiquitous in nature. It has been estimated that over 80% of countries have developed national cancer control plans. However, the central issue that presented a significant barrier was the successful launch of implementing the plan. There is a great need to assess and evaluate those implementation barriers to overcome this impediment (Figure 15). When conducting this SSA, it was highlighted that there were significant drivers that led to an unsuccessful launch, such as: 1. Lack of Governance structure and commitment to making cancer control a priority. 2. Political will When government changes priority, and the plan is shelved.
3. There is no funding allocation and a lack of budget for cancer control. 4. Did not actively involve many stakeholders and experts in the planning and implementation phase. 5. Efforts and communications need to be more effectively coordinated. 6. There is no monitoring system to take corrective actions when things are going wrong, NO NCCP.
There is a great need for the government (MOHW) to focus on cancer control funding to establish a Belize National Cancer Registry (BNCR), NCCP and cancer research. The NCCP and BNCR are the two primary vital mechanisms that will strengthen cancer health systems to deliver optimum care delivery for cancer. In addition, the NCCP and BNCR will be able to address backlogs in diagnosis and treatment. From the latter, the country can develop a cancer control plan that directly meets the needs and deficiencies in delivering cancer health care.
Addressing the Implementation Barriers Leads to a Successful Launch
A fortified governance structure with a political will to always ensure that cancer control is a priority with a line of budget attached. A line of budget and funding allocation must be directed towards cancer control because a plan without a budget is bound to fail [13]. This fortified governance structure must ensure that all stakeholders and experts are involved in every cancer control and implementation planning phase. Creating a fortified governance structure fully integrated with stakeholders’ input will eradicate those fragmented efforts and communication in cancer initiatives made [14]. The importance of how the government must be involved in requests and allocate funding for cancer control cannot be over-emphasized. This is a critical key and line of action for cancer control planning [15, 16].
There are many benefits to having a fortified government structure that is cross-linked with local stakeholders and experts in cancer control:
- Local Stakeholders and Experts on the ground have a comprehensive perspective of what is going on and those implementation barriers that may affect a successful launch.
- Having local stakeholders and experts will increase accountability.
- It shall ensure coordinated efforts and increase communication to suppress entities’ working siloes.
- Increase collaboration so resources can be pooled and data sharing to get a comprehensive care delivery for cancer control.
- Increase monitoring systems and have a contingency plan ready to be deployed.
- Eliminate undermined strategies and efforts for effectiveness in cancer control.
- Ensure that the plan and budget for cancer control are scaled appropriately.
- Ensure that the plan is feasible, realistic and suits the country’s immediate needs as it pertains to cancer control.
They will provide inputs based on their experiences as first-line respondents in delivering cancer care, such as prevention and palliative care. Academia involvement is also critical as it pertains to research [17]. Research is the nucleus for all action areas in cancer control (Figure 15). Areas of Action are essential for a successful launch:
- Policy and Planning Formulation
- Policy and Planning Implementation
- Policy and Planning Agenda [18]
Most countries that successfully implemented cancer control at a national level had an effective NCCP with an “exemplary government mechanism” in place that collaborated with local stakeholders and experts in cancer. This “exemplary government mechanism” is the central driver responsible for coordinating with key stakeholders to overcome these implementation barriers that inhibit a successful launch (Figure 16) [19]. This dedicated team had a national cancer registry to: 1. Collect and Maintain data
2. Conduct Cancer research and cancer epidemiological research 3. Plan based on evidence-based data 4. Implementation strategy for NCCP on how to finance cancer control based on data 5. Implement interventions and monitor cancer interventions 6. Prioritization of identifying critical gaps 7. Focus support and efforts in mobilizing partners for lack or barrier identified in treatment or care delivery for cancer.
The Belize National Cancer Registry is the Foundation and Solution for an Effective Cancer Control Plan
To address the country-specific cancer burden, reliable, evidence-based data is needed. Belize must collect data. Belize must launch a successful cancer registry to be able to:
- To identify the types of cancer prevalent in a country
- The number of cases
- The mortality
- The populations most affected and other information Collectively, all the latter are vital not only to design an effective strategy but also to monitor the impact of any cancer plan.
There is a great need to set up hospital-based, pathology-based, and population-based cancer registries. The Belize National Cancer Registry will elucidate the country’s burden and effectively plan, based explicitly on the data generated from the registry, to mitigate the increase of cancer in morbidity and mortality in Belize.
The logistical flow of the successful launch of the Belize National Cancer Registry:
- Successful implementation of BNCR with coordinated input from local stakeholders and experts.
- Enhance and strengthen the BNCR.
- Induce evidence-based data to feed into the development of the National Cancer Plan.
- Revision of cancer plans based on the evidence highlighted by BNCR.
The data generated from the BNCR will be more reflective and representative of the current state of cancer within the population. It will give evidence-based data on the distribution and key people at risk.
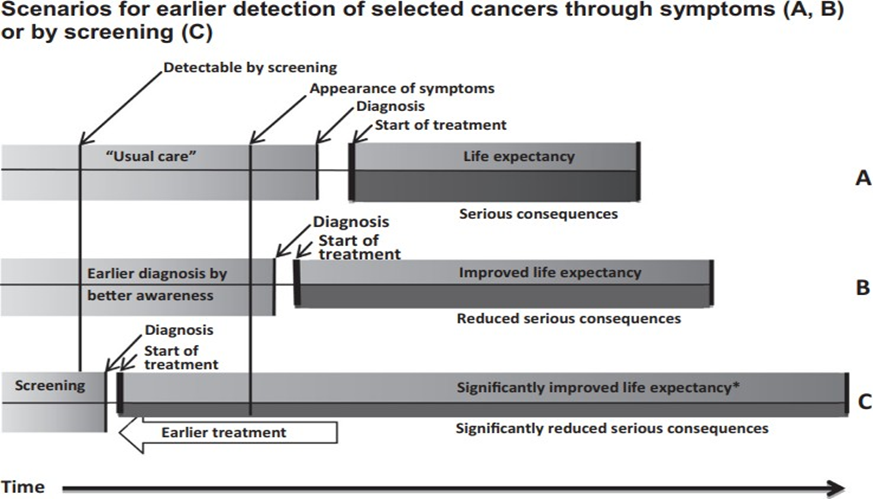
The Need for Early Detection for Cancer Control in Belize
Early detection and diagnosis are vital for eliminating the mortality of cancers. The start of cancer treatment depends on the stage of detection and diagnosis. Life expectancy increases significantly when diagnosis or detection in the early stages occurs [19, 20]. In addition, the severe consequences of the diseases lessen and access to immediate quality treatment significantly decrease cancer mortality (Figure 17).
Oncological Point of View
Oncologist: Dr. Ramon Yacab Cancer Care in Belize Vision: For guaranteed cancer care to every Belizean to be truly accessible, affordable and effective with services through the development of programs enhancing the complete continuum of care. Social disparities should not determine a patient’s opportunity to live.
Critical Issues Identified/Challenges
Lack of Awareness: Cancer is only remembered in October. But there is not any real awareness related to cancer. Diagnostic Testing 1. No radiological studies are available to patients in the form of CT scans or MRIs in the public health care system. Radiological studies may sometimes be more expensive than six months of patient treatment. 2. Pathology services have delayed results, and basic IHC is unavailable for breast cancer categorizations.
Treatment
Lack of Access to Chemotherapy Drugs: The KHMHA currently has chemotherapy drugs due to a revolving fund from a grant from SSB. The Revolving fund is a short to midterm patch, but we need continued medication supply. The medications are not included in the national drug formulary, nor are they being provided by MoH. There are different avenues of drug acquisition via PAHO/ COMISCA, which reduces cost, but these require direct intervention from a Government/MoH. Lack of Access to Radiation Services: Radiation is not available in Belize. Every patient requiring it must travel abroad with out of pock finances-those who can afford travel. No subsidy is provided to these patients, nor is there any regional agreement with neighbouring countries that could increase radiation accessibility. Lack of Access to Palliative Care: There is a significant need for medical and non-medical personnel training on the market for palliative care at the primary care level. Also, access to opioids has been a struggle; there were over six months of stock out of pain medication for patients.
Research: There is a lack of research regarding different aspects of oncology care.
Oncological Surgical Point of View
Oncological Surgeon: Dr Byron Simmons Cancer Care in Belize 1. No initiative or establishment
2. Lack of involvement, advocacy, engagement, and commitment from MOHW 3. No focal Person for cancer 4. Overwhelmed system� Doctors and Nurses 5. No functional activation of the Cancer Registry 6. No surgical management 7. Not much can be offered for Pediatric Cancer� , mostly referrals and solid tumour removal. 8. Note: The majority of Pediatric Cancer is Lymphoma and Leukaemia 9. In regards to adults, there is a significant influx or increase of surgical operations scheduled This results in competition for surgery works to the detriment of Cancer patients and Increases poor outcomes and survival 10. No CT scan at KHMH; will help diagnose cancer patients 11. No beds available for cancer patients 12. No organizational format for cancer patients 13. Lack of tools and HR
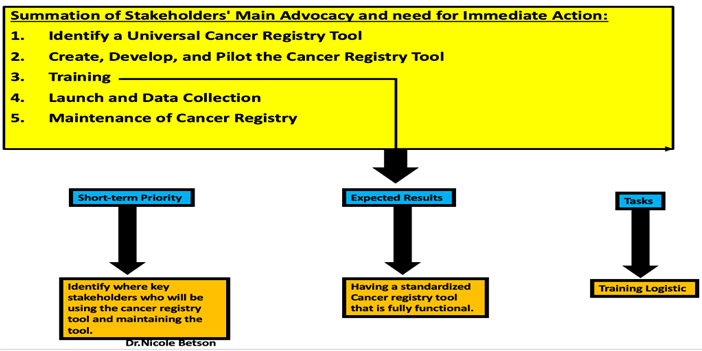
Cancer Registry
There is a need for both clinical and population-based registries. Doctors must go through the proposed Cancer Registry tool to do critical assessments and evaluations to improve the instrument. To verify if it captures key variables and is on an international level. To be heavily involved in the development and revision of the device.
Maternal and Child Health Care Perspective
Focal Person: Dr. Natalia Largaespada When a woman dies, the child, family, community, and country are affected negatively. Working women contribute to the well-being of their family and community and the country’s development. Children, at whatever age, cannot substitute the loss of their mother. The bonding and attachment between a mother and her child or children are never dissolved, leaving a scar that is never healed.
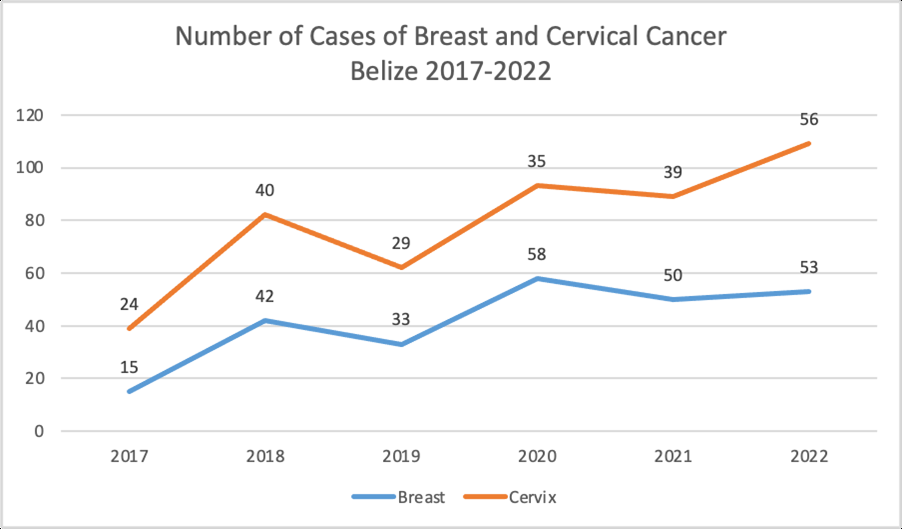
Women in Belize experience untimely death due to breast cancer and cervical cancer. Cervical cancer can be prevented with vaccines, early cervical cancer screening, access to early care and treatment, and adequate follow-up of affected women.
The Government of Belize is committed to eliminating cancer. The government cannot do it on its own. Cancer is a societal problem that requires the active participation of society. Although many of cancers do not have a clear preventive pathway, the preventive efforts for preventable cancers must be a multisector response from all entities and levels of care.
In 2021, the estimated total population of Belize was 430,191. Annually, 34 women are diagnosed with cervical cancer and approximately 25 die from the disease. The median number of days between diagnosis and death is 70, ranging from 1 to 364 (Figures 19-21). This clearly indicates late demand for services or a passive search for cases (Table 2).
| Burden of cervical cancer | Incidence | Morality |
|---|---|---|
| Annual Number of new cases/deaths | 34 | 25 |
| Crude Rate | 17 | 12.5 |
| Age-standarized rate | 19.1 | 14.8 |
| Cumulative Risk 0-74 years(%) | 1.8 | 1.43 |
| Ranking of cervical cancer (all years) | 2nd | 1st |
| Ranking of cervical cancer (15-44 years) | 2nd | 2nd |
The cervical cancer prevention and control interventions are summarized below:
- Pap smears available at health facilities
- 2007 Pap Smear and HPV testing campaign in Belize City (450 women)
- 2008 Belize Cancer Center Dangriga - community-based center
- 2013 Comprehensive Cancer Report
- 2013 Cost Effectiveness of HPV vaccine introduction
- 2016 Introduction of the HPV vaccine (Quadrivalent)
- 2016 School-based vaccination program funded by the government
- 2017 Introduction of VIA (Single Visit Approach)
- 2018 Updated manual and treatment guidelines – cervical cancer
- 2019 Visiting OBGYN Oncologist (once or twice a year)
- 2021 Oncology clinic at the national referral hospital (Karl Heusner Memorial Hospital)
- 2022 Introduction of the HPV testing From 1,044 HPV tests done using the Ampfire HPV Technology by Atila BioSystems, up to January 30th (6 weeks), 1,044 HPV tests were done, of which 259 resulted positive for a positivity rate of 24.8%. The high-risk HPV (hrHPV) test seeks to identify the presence of hrHPV 16 and 18 known to be the most oncogenic types; they are responsible for 70% of cervical cancer cases. The hrHPV test can also detect 12 other cervical cancer-causing hrHPV viruses. The positive rate for hrHPV 16 and/or 18 is 7% of the total HPV test done (Table 3).
| Primary Prevention | Secondary Prevention | Tertiary care |
|---|---|---|
| SRH Education | HPV Testing | Chemotherapy |
| HPV vaccine | Pap Smear | Radiotherapy |
| VIA | ||
| Colposcopy | ||
| LEEP |
Critical Issues Identified
- Poor National Response to Cancer Care Disjointed Advocacy Absent cohesive Leadership and Initiative
- Diagnosis of Cancer is not accurate or timely
- There is no comprehensive, cost-effective Cancer treatment established.
- Long-term care for survivorship and rehabilitation access � Non-existent
- There is a need for improved palliative care services in Belize.
- Poor management of information systems for cancer.
7. The generation of evidence for Cancer is non-existent. 8. No mechanism was identified for sustainable financing The availability of medication is inadequate medication (Chemotherapeutic drugs and morphine for cancer patients are palliative). 9. No adequate health workforce was established for Cancer. 10. No infrastructural plan was developed for Cancer. 11. No procurement of pharmaceuticals or diagnostics. 12. Cancer Registry not available. 13. Report with outcome/survival and mortality data not available.
14. Patient Management information system not available. 15. No publications are available.
Conclusion
In summation, active commitment from the government with a line of budget is a critical need for cancer control in Belize. Presently, no cancer registry in Belize has been successfully activated. There is an excellent need for Belize National Cancer Registry and National Cancer Control Program (Figure 22). The success of the latter is dependent on the multisectoral approach where the MOHW is the central driver. It is not usually how most MOH work, but a multisectoral process is the key to a successful launch and mitigating those implementation barriers. A plan without a budget and multisectoral strategy will remain just a plan or be shelved. In addition, there were a lot of projects, policies and efforts that had two significant issues. These primary issues were: 1. There were issues with the implementation. 2. Some plans and policies were not specifically tailored to address cancer control in Belize.
In either case, the common denominator was that it was not a multisectoral approach of inclusivity in developing plans and for implementation. There must be integration and interconnectivity between MOHW and local stakeholders/ experts in cancer. Consequently, this will lead to an unsuccessful launch.
- There is an excellent need for Advocacy, Engagement, and Commitment from the MOHW for ALL cancer patients.
- MOHW provides cancer care management.
- MOHW needs a Focal Person for Cancer to be the liaison of all public and private stakeholders to outsource locally and internationally.
- Need Procurement for Bulk of chemotherapy from MOHW.
- Need for National Cancer Control Program and Centre.
A centralized location that fosters the needs of ALL cancer for screening.
The Ministry of Health and Wellness has an excellent opportunity to take leadership in cancer control. MOHW now has the chance to fortify the governance structure that takes on a multisectoral approach to successfully launch Belize’s first National Cancer Control Program and Belize National Cancer Registry.
- Fixing issues within government institutions
- Fixing the organisational structure since it is a systemic change that needs critical attention.
- There is a need for an operational and cancer control plan, not a conceptual document.
- There is a great need for quality and efficient services
- Ensuring and monitoring optimum care is being delivered.
- Primary services: Cervical and Breast screening Quality control with efficiency. There is a lag time of approximately 2-3 months.
- Procurement of needed medication
- Need for quality Pathology services
- The pathology department needs immediate fixing.
- Updated equipment
- Better-trained physicians and nurses in oncology.
- There is a need for Radiological Services for investigation & management.
- Targeted mental health support and nutritional support structures for cancer patients.
- There is a need for a cancer registry so that the country can come to grips with having a cancer control plan to reduce the burden of cancer in Belize.
- No more delaying the process by waiting for international partners to initiate the process.
- Building the tool with critical factors to consider, as seen in Figure 18 and Figure
Recommendations
There is a great call and need for immediate action and attention for cancer control in Belize. All stakeholders/ experts in cancer control, especially locally, must be involved throughout the planning and implementation phase. International consultants should not be the primary solution for cancer control because they do not have the experience to tackle the issues or challenges the local experts face daily.
Belize is a relatively small jurisdiction in regards to per million population. This can be both a blessing and a bane, but if approached systematically and strategically efficiently, we can augment the former and decrease the latter. As has been established from time immemorial, below are the six pillars of a National Cancer Program:
- Prevention
- Screening
- Early Diagnosis
- Treatment
- Rehabilitation
- Palliation Because of our small population size, these six broad aspects of oncology can be managed in a time-sensitive fashion to include as significant a proportion of Belizeans as possible.
We all know what each entails, but for some reason, we have not been able to launch a national response to address each and instead have had an ad hoc approach.
As for the opposing facet of our small population, advocacy through the auspices of MOHW, a cancer centre/ unit/ ward/ is designated with sufficient organizational and material infrastructure, as well as the concentration of personnel dedicated to cancer to concentrate the limited resources we have as well as building on experiences to increase our success rates in regards to managing run of the mill as well as complex cases, with improved results that would translate into better survival rates.
Speaking specifically on the Cancer Registry, key stakeholders using the tool must see the instrument and be involved in the development phase before the official launch. If and when it is launched, emphasis should be placed on sensitizing, training and stimulating the “catchment personnel”, be it surgeons, oncologists, medical officers, or pathologists.
Specific Health Services
Early Diagnosis Program
There needs to be an emphasis on an early diagnosis program (Figure 24). Significant barriers that cause the reduction of proper diagnosis and treatment among patients who have cancer: 1. Among the public, there is poor cancer awareness 2. At the primary health care level, there is suboptimal knowledge about cancer symptoms and adequate diagnosis follow-up;
3. Accessibility is poor 4. Too expensive in terms of affordability for quality services concerning diagnosis and treatment. 5. Unclear referral pathways, errors in diagnosis 6. Administrative red tape 7. Accessing services efficiently because of various barriers:
- Psychosocial
- Financial
- Logistical
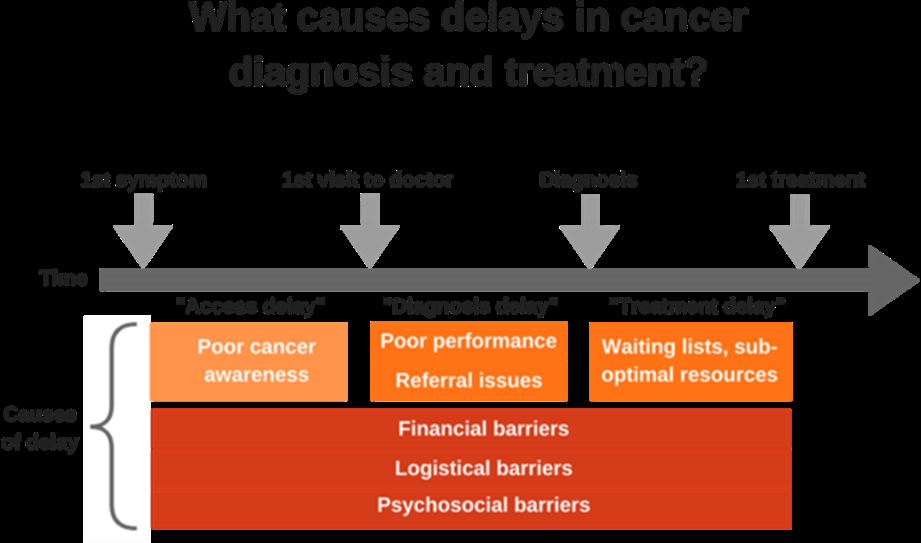
There seems always to be a delay between detecting the first symptoms and treatment. First, to reduce this from happening, it is critical to have adequate health staff training to react efficiently and rapidly. Second, affordable, quality and rapid services (diagnostic and treatment) need to be offered (Figure 25). Third, there needs to be an educational platform that sensitizes all individuals on when to seek professional help as soon as symptoms appear. Collectively, this shall reduce cancer barriers seen in the delivery of care (Figure 26). The implementation of this approach is inexpensive compared to screening programmes. Early Diagnosis programs can reach a larger audience (target) population. This type of program will eradicate those barriers prevalent in cancer control.
Acknowledgements
Javier Zuniga Mr. Enrinque Romero Oncologist Dr. Ramon Yacab Oncological Surgeon Dr. Byron Simmons Belize Health Care Partners Dr. Atanascio Cob Belize Medical Associates Dr. Rosado Dr. John Sosa Dr. Fernando Cuellar Garden City and St. Gabourel Medical Center Dr. Renee Gudoy St. Luke Hospital Dr.Ivan Depaz La Loma Luz, Adventist Hospital Mr. Adan Sosa Dr. Marvin Camal Northern Medical Plaza Dr. Marko Mendez Belize Specialist Hospital, Gastroenterology and Endoscopy Center Dr.Irvin Gabourel Buttonwood Medical Center Dr. John Goff Belize Dangriga Cancer Center Dr. Ellsworth Grant (Medical Director) Nurse Dellone Pascasio (CEO) Nurse Pauline Okolo Nurse Prosper NHI Dr. Ramon Figueroa University of Belize Dr. Lisa Johnson Ministry of Health and Wellness Maternal and Child health-care Dr.Natalia Largaespada Special Acknowledgement: I would like to express my deepest appreciation to Dr. Javier Zuniga. This endeavor would not have been possible without his approval, support and encouragement. In addition, I would like to express my deepest gratitude to Mr. Enrinque Romero and the National AIDS Commission for their financial assistance and continued support. In addition, Can you please add Dr. Javier Zuniga to the paper (I noticed in correction it only had Javier Zuniga, I want to give him respect as a doctor) Competing Interest Statement: The authors have declared no competing interest. Clinical Trial: The study was not registered for clinical trials because the study did not involve human subjects. Funding Statement: No external funding was received. Author Declarations I confirm all relevant ethical guidelines have been followed, and any necessary IRB and/or ethics committee approvals have been obtained. Yes The details of the IRB/oversight body that provided approval or exemption for the research described are given below:
- Ethical approval was not necessary because this study did not involve human subjects and animal studies.
- All necessary patient/participant consent has been obtained and the appropriate institutional forms have been archived. Yes.
- I understand that all clinical trials and any other prospective interventional studies must be registered with an ICMJE-approved registry, such as ClinicalTrials. gov. I confirm that any such study reported in the manuscript has been registered and the trial registration ID is provided (note: if posting a prospective study registered retrospectively, please provide a statement in the trial ID field explaining why the study was not registered in advance). Yes.
- I have followed all appropriate research reporting guidelines and uploaded the relevant EQUATOR Network research reporting checklist(s) and other pertinent material as supplementary files, if applicable. Yes.
References
-
Hendren S, Chin N, Fisher S, Winters P, Griggs J, et al. (2011) Patients’ barriers to receipt of cancer care, and factors associated with needing more assistance from a patient navigator. J Natl Med Assoc 103(8): 701-710.
-
Townsend JS, Moore AR, Mulder TN, Boyd M (2015) What does a performance measurement system tell us about the National comprehensive cancer control program? J Public Health Manag Pract 21(5): 449-458.
-
Murphy CC, Lupo PJ, Roth ME, Winick NJ, Pruitt SL (2021) Disparities in Cancer Survival Among Adolescents and Young Adults: A Population-Based Study of 88 000 Patients. J Natl Cancer Inst 113(8): 1074-1083.
-
Rodriguez GM, Leach M, Osorio J, Villicana G, Koontz Z, et al. (2022) Exploring cancer care needs for Latinx adults: a qualitative evaluation. Support Care Cancer 31(1): 76.
-
Fan Q, Nogueira L, Yabroff KR, Hussaini SMQ, Pollack CE (2022) Housing and Cancer Care and Outcomes: A Systematic Review. J Natl Cancer Inst 114(12): 1601- 1618.
-
Keegan TH, Ries LA, Barr RD (2016) For the National Cancer Institute Next Steps for Adolescent and Young Adult Oncology Epidemiology Working Group. Comparison of cancer survival trends in adolescents and young adults in the United States with those in children and older adults. Cancer 122(7): 1009-1016.
-
Sung H, Siegel RL, Rosenberg PS, Jemal A (2019) Emerging cancer trends among young adults in the USA: analysis of a population-based cancer registry. Lancet Public Health 4(3): e137-e147.
-
Zaki TA, Liang PS, May FP, Murphy CC (2023) Racial and Ethnic Disparities in Early-Onset Colorectal Cancer Survival. Clin Gastroenterol Hepatol 21(2): 497-506.
-
Hannon PA, Fernandez ME, Williams RS, Mullen PD, Escoffery C, et al. (2010) Cancer control planners’ perceptions and use of evidence-based programs. J Public Health Manag Pract 16(3): E1-E8.
-
Blake KD, Moss JL, Gaysynsky A, Srinivasan S, Croyle RT (2017) Making the case for investment in rural cancer control: an analysis of rural cancer incidence, mortality, and funding trends. Cancer Epidemiol Biomarkers Prev 26(7): 992-997.
-
Meilleur A, Subramanian SV, Plascak JJ, Fisher JL, Paskett ED, et al. (2013) Rural residence and cancer outcomes in the United States: issues and challenges. Cancer Epidemiol Biomarkers Prev 22(10): 1657-1667.
-
Cartmell KB, Bonilha HS, Simpson KN, Ford ME, Bryant DC, et al. (2020) Patient barriers to cancer clinical trial participation and navigator activities to assist. Adv Cancer Res 146: 139-166.
-
BRFSS, CDC (2018) Behavioural risk factor surveillance system survey data. Atlanta, Georgia: US Department of Health and Human Services, Centers for Disease Control and Prevention.
-
Williamson MR (2021) Success Rates for the Objectives of US State Cancer Control Plans: A First Look. Cancer Control 28: 10732748211041504.
-
Hayes NS, Hohman K, Vinson C, Pratt-Chapman M (2018) Comprehensive cancer control in the U.S.: summarizing twenty years of progress and looking ahead. Cancer Causes Control 29(12): 1305-1309.
-
ICCP (2016)National Cancer Control Plan Development and Implementation Assessment Tool. International Cancer Control Partnership.
-
Belle Isle L, Plescia M, La Porta M, Shepherd W (2010) In conclusion: Looking to the future of comprehensive cancer control. Cancer Causes Control 21(12): 2049- 2057.
-
CDC (2020) Cancer Plan Self-Assessment Tool. Atlanta2020. Centers for Disease Control and Prevention.
-
CDC (2010) Comprehensive Cancer Control Branch Program Evaluation Toolkit. Centers for Disease Control and Prevention.
-
Oar A, Moraes FY, Romero Y, Ilbawi A, Yap ML (2019) Core elements of national cancer control plans: A tool to support plan development and review. Lancet Oncol 20(11): 645-652.
- Origin, Evolution, and Functional Impact of Short Insertion- Deletion Variants in Human Genomes: A Review
- Harnessing Molecular Glues for Next-Generation Vaccine, Cancer and Cardiovascular Disease Drug Development: A Comprehensive Review
- Lateral Cervical Epidermal Inclusion Cyst in a Paediatric Patient: A Rare Case Report
- Malarial Plasmodium Falciparum with Hepatitis B and C Virus Infections among Blood Donors in Ife Central Local Government Area, Ile Ife, Osun State, Nigeria
- Withanolides and Withaferin A- What’s next in Ashwagandha Research
- Designing of Dual Pulse Photoacoustic Tomography for Imaging of Drug-Response and Tumor Growth