Pharmacogenetics of Type 2 Diabetes Mellitus: Linking Genetic Variability to Drug Efficacy and its Cardiovascular Outcomes
Type 2 Diabetes Mellitus (T2DM) is a complex metabolic disorder characterized by insulin resistance, impaired insulin secretion, and increased hepatic glucose production. The rising prevalence of obesity-related insulin resistance has led to a surge in T2DM cases, particularly in urban populations of both developed and developing countries. To address this multifactorial pathophysiology, several classes of pharmacological agents are available, each targeting different aspects of glucose regulation. The choice of therapy is often guided by efficacy, patient-specific factors, and potential side effects, particularly cardiovascular safety. This article outlines the mechanisms of action of commonly used T2DM drugs, and their adverse drug effects, specifically examining cardiovascular impact. We selected the drugs which are most commonly used by our Physicians these includeseven major classes of anti-diabetic drugs: Metformin, GLP-1 receptor agonists, SGLT2 inhibitors, Sulfonylureas, Meglitinides, Thiazolidinediones (TZDs), and DPP-4 inhibitors. Understanding their distinct pharmacodynamics is crucial for optimizing individualized treatment plans and minimizing complications of their Cardiac effects in patients with T2DM.
Jamil K¹*, Yerra SK² and Sultana S¹
¹Genetics Department, Bhagwan Mahavir Medical Research Centre, India ²Cardiology department, Mahavir Hospital and Research Centre, India
Abbreviations
T2DM: Type 2 Diabetes Mellitus; CVD: Cardiovascular Disease; SGLT-2: Sodium-Glucose Co-Transporter TZDs: Thiazolidinediones; DPP-4: Dipeptidyl Peptidase-4; GLUT-2; Glucose Transporter Type 2; ATP: Adenosine Triphosphate; ADP: Adenosine Diphosphate; DNA: Deoxyribonucleic Acid; GI: Glycemic Index (sometimes also Gastrointestinal, depending on context); MI: Myocardial Infarction; HF: Heart Failure; DKA: Diabetic Ketoacidosis; LDL: Low- Density Lipoprotein (bad cholesterol); HDL: High-Density Lipoprotein (good cholesterol); IGT: Impaired Glucose Tolerance; CNS: Central Nervous System; MACE: Major Adverse Cardiovascular Events; NASH: Non-Alcoholic Steatohepatitis; PCOS: Polycystic Ovary Syndrome; GWAS: Genome-Wide Association Study; PKA: Active protein kinase; AMPK: AMP-activated protein kinase; PPARγ: Peroxisome Proliferator-Activated Receptor Gamma.
Introduction
Type 2 Diabetes Mellitus (T2DM) is a global public health concern, with obesity being a primary contributing factor [1]. A significant proportion of T2DM patients—especially in South Asian populations—present with obesity, exacerbates insulin resistance and increases the risk of cardiovascular complications. In these patients, choosing the appropriate pharmacotherapy requires careful consideration of both glycaemic efficacy and metabolic effects, including impact on body weight and cardiovascular outcomes [2]. In obese individuals, the accumulation of visceral adipose tissue contributes to chronic low-grade inflammation, increased free fatty acids, and adipokine dysregulation—all of which impair insulin signalling pathways [3]. Effective pharmacotherapy in obese T2DM patients must therefore address hyperglycaemia, insulin resistance, weight management, plus cardiovascular protection. This review evaluates the pharmacological characteristics of key antidiabetic drug classes and their suitability for managing obese T2DM patients.
Pharmacogenetics of T2DM Drugs, Genetic Interactions Every year, thousands of deaths are attributed to fatal drug reactions, many of which arise from complex interactions between disease severity, drug–drug interactions, nutritional status, impaired renal and hepatic functions, and inherited genetic variations in drug metabolism [4]. In type 2 diabetes mellitus (T2DM), pharmacogenomic research has shown that genetic polymorphisms play a pivotal role in determining both therapeutic efficacy and adverse drug reactions [5]. For instance, polymorphisms in the CYP2C9 gene affect the metabolism of sulfonylureas, leading to reduced clearance and a higher risk of hypoglycaemia in slow metabolizers [6]. Similarly, variants in the SLC22A1 gene, encoding the OCT1 transporter, influence the hepatic uptake of metformin, thereby modulating its glucose-lowering effect [7]. The PPARγ, Pro12Ala polymorphism alters sensitivity to thiazolidinediones, while variations in KCNJ11 (E23K) and ABCC8 genes, which encode subunits of the pancreatic KATP channel, impact sulfonylurea responsiveness by altering β-cell insulin secretion [8]. Moreover, polymorphisms in the TCF7L2 gene, a key genetic risk factor for T2DM, have been consistently linked to differential therapeutic outcomes with both sulfonylureas and metformin [9]. These examples highlight that genetic diversity—rooted in differences in DNA sequences among individuals, ethnic groups, and populations—not only contributes to variability in drug response but also underlines the importance of pharmacogenomics in guiding personalized therapy for T2DM and simultaneously determining its cardiotoxicity safety. Genetic polymorphism of the denes interacting with the Drugs is presented in Table 1.
| Drug Class / Drug | Key Gene(s) | Polymorphism(s) | Effect on Drug Response / Clinical Implication |
|---|---|---|---|
| Sulfonylureas (e.g., Glibenclamide, Glimepiride) | CYP2C9 | CYP2C9 *2, *3 alleles | Reduced metabolism → higher plasma levels → ↑ risk of hypoglycaemia |
| KCNJ11 / ABCC8 | KCNJ11 E23K, ABCC8 variants | Alter β-cell KATP channel activity → variable insulin secretion response | |
| TCF7L2 | rs7903146 (T allele) | Poorer response to sulfonylureas; risk of secondary failure | |
| Metformin | SLC22A1 (OCT1) | R61C, G401S, 420del, G465R | Reduced hepatic uptake → diminished glucose-lowering effect |
| SLC47A1 (MATE1), SLC47A2 (MATE2-K) | rs2289669, rs12943590 | Altered renal clearance → variability in therapeutic effect | |
| ATM | rs11212617 | Associated with enhanced glycaemic response to metformin | |
| Thiazolidinediones (e.g., Pioglitazone, Rosiglitazone) | PPARG | Pro12Ala | Ala variant associated with improved insulin sensitivity and better drug response |
| CYP2C8 | CYP2C8 *3 allele | Faster metabolism → lower drug levels → reduced efficacy | |
| DPP-4 Inhibitors (e.g., Sitagliptin, Vildagliptin) | DPP4, GLP1R | Limited polymorphism data | Early studies suggest variability in incretin response influencing efficacy |
| SGLT2 Inhibitors (e.g., Dapagliflozin, Empagliflozin) | SLC5A2 (SGLT2) | Mutations rare but relevant | Polymorphisms may influence renal glucose reabsorption and efficacy |
| Insulin Therapy | INS, IGF2, INSR | Multiple variants | Genetic background influences insulin sensitivity and dosing requirements |
Table 1: Genetic Polymorphisms of genes Influencing Drug Response in Type 2 Diabetes Mellitus.
Mechanism of action of the Drug-Gene Interactions
Sulfonylureas
(e.g., Glipizide, Glimepiride) These drugs bind to sulfonylurea receptor (SUR1) in Pancreatic β-cells on ATP-sensitive K⁺ channels, close the channel and bring about membrane depolarization resulting in opening voltage-gated Ca²⁺ channels, increases calcium influx triggers insulin secretion. The net effect shows increase in insulin levels and lowering blood glucose levels causing the Glucose-independent risk of hypoglycaemia [10]. Sulfonylureas (e.g., Glibenclamide, Glipizide, Glimepiride) often cause Hypoglycaemia especially in elderly or renal dysfunction and weight gain. Older subjects taking drugs like Glibenclamide had increased CV risk in some studies (due to ischemic preconditioning inhibition) [11].
Metformin (Biguanide)
Metformin inhibits hepatic gluconeogenesis, activates AMP- (activated protein kinase) improves insulin sensitivity to enhances glucose uptake in muscle and fat. However, its side effects include -gastrointestinal (GI) disturbances: nausea, diarrhoea, abdominal discomfort and Vitamin B12 deficiency upon long-term use. Its been described as Cardioprotective, reduces macrovascular complications and may improve endothelial function and reduce LDL [12].
Thiazolidinediones (TZDs)
(e.g., Pioglitazone, Rosiglitazone) Thiazolinediones (TZDs) mostly acts on Adipose tissue, muscle and, liver by activating peroxisome proliferator- activated receptor-γ (PPAR-γ), a nuclear receptor which relates to increase in transcription of genes regulating glucose and lipid metabolism, to improve insulin sensitivity in peripheral tissues (adipocytes, muscle). This promotes adiponectin release, and reduces inflammatory cytokines. This causes decrease in insulin resistance, and fasting glucose, with no effect on insulin secretion [13].
Thiazolidinediones (TZDs) such as Pioglitazone, Rosiglitazone are known for fluid retention and weight gain, Patients are at risk of bone fractures (esp. in women). Pioglitazone: may reduce stroke and MI risk but increases heart failure risk due to fluid retention. Rosiglitazone is associated with a risk for MI [14, 15].
Dipeptidyl Peptidase-4 (DPP-4) Inhibitors
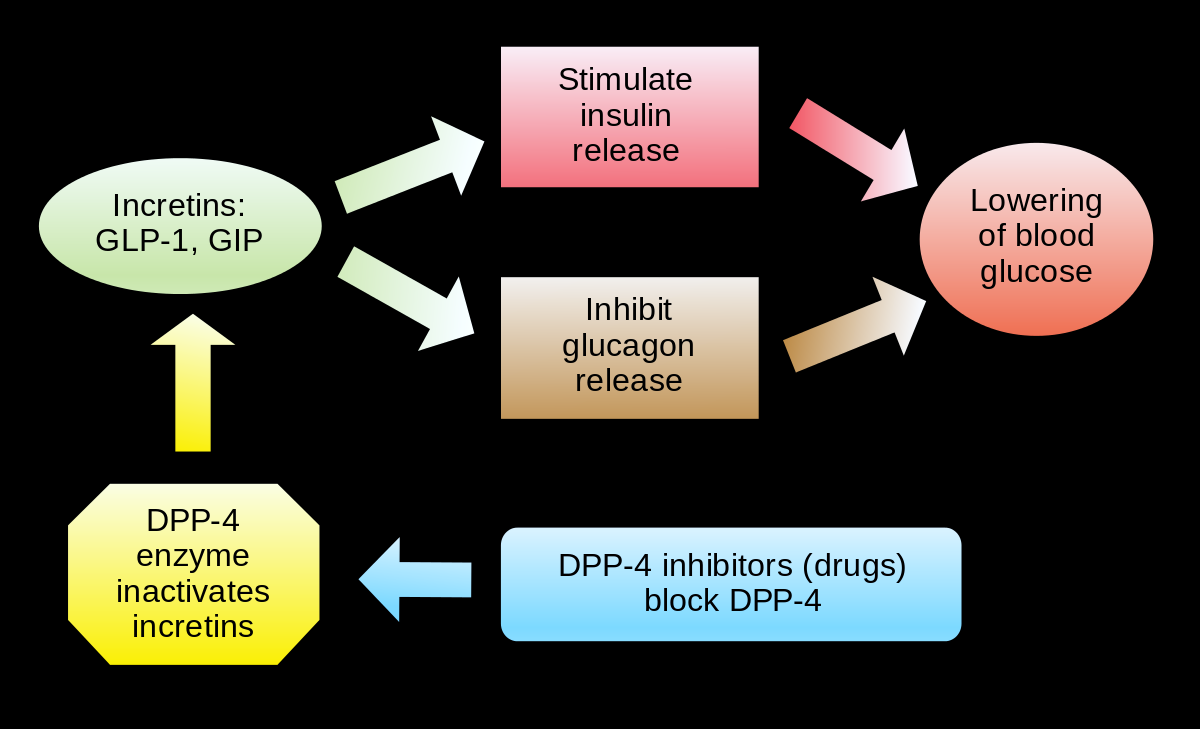
(e.g., Sitagliptin, Saxagliptin, Linagliptin) These drugs inhibit DPP-4 enzyme → prolong the half-life of endogenous incretins (GLP-1 and GIP), increase Glucose- dependent insulin secretion, and lower Glucagon secretion resulting in lowering blood glucose, mainly postprandial [16].
DPP-4 Inhibitors such as Sitagliptin, Saxagliptin, Linagliptin are generally well tolerated for Nasopharyngitis, headache, joint pain. In some cases Saxagliptin: increases the risk of hospitalization for heart failure (SAVOR-TIMI 53 trial), Sitagliptin and Linagliptin are considered safe for CVD with no HF signal [17].
SGLT2 Inhibitors
(Sodium-glucose co-transporter-2 inhibitors: e.g., Empagliflozin, Dapagliflozin) This drug prevents glucose reabsorption in kidneys, increases urinary glucose excretion (glucosuria), mild osmotic diuresis, affecting plasma glucose, modest weight loss, BP reduction [18]. SGLT2 Inhibitors such as Empagliflozin, Canagliflozin, Dapagliflozin can cause genital and urinary tract infections, and Diabetic ketoacidosis (euglycemic DKA) with a risk of amputations (esp. with Canagliflozin). It is highly cardioprotective and useful even in non-diabetic heart failure patients [19].
GLP-1 Receptor Agonists-
(Glucagon-like peptide-1 analogues: e.g., Liraglutide, Semaglutide) The site of action of this class of drugs is: Pancreas, stomach, brain, liver Mostly these drugs mimic the incretin hormone GLP-1, leading to increase in Glucose- dependent insulin secretion from β-cells, decrease in Glucagon secretion from α-cells, enhances satiety via CNS leading to weight loss, with minimal risk of hypoglycaemia [20]. GLP-1 Receptor Agonists also include drugs like, Liraglutide, Semaglutide, Exenatide. However, they may cause nausea, vomiting, and weight loss. Its positive effects includes reduction in major adverse cardiovascular events (MACE) in patients with T2DM and existing CVD [21].
Meglitinides
(e.g., Repaglinide, Nateglinide) These drugs are mostly similar to sulfonylureas, bind to a different site on ATP-sensitive K⁺ channels in Pancreatic β-cells, cause rapid, short-acting insulin release, with a net effect on control postprandial glucose spikes, lower hypoglycaemia risk than sulfonylureas Meglitinides (e.g., Repaglinide, Nateglinide) cause hypoglycaemia (less than sulfonylureas), and weight gain in patients. These drugs are considered safer for cardiac events in elderly due to shorter action [22]. The mechanism of action of the drugs is summarised in Table 2.
| Drug Class | Primary Action | Site of Action | Insulin Secretion | Effect on Weight |
|---|---|---|---|---|
| Metformin | ↓ Hepatic glucose production, ↑ insulin sensitivity | Liver, muscle | No | Neutral or ↓ |
| GLP-1 agonists | ↑ Insulin (glucose-dependent), ↓ glucagon, ↓ appetite | Pancreas, brain, gut | Yes (glucose- dependent) | ↓ |
| SGLT2 inhibitors | ↑ Renal glucose excretion | Kidney | No | ↓ |
| Sulfonylureas | ↑ Insulin secretion (glucose- independent) | Pancreatic β-cells | Yes | ↑ |
| Meglitinides | ↑ Short-acting insulin secretion | Pancreatic β-cells | Yes | ↑ or Neutral |
Table 2: Summary of Mechanism of action of the drugs.
| Drug Class | Major ADEs | Effect on Heart/CV System |
|---|---|---|
| Metformin | GI upset, lactic acidosis, B12 deficiency | Cardioprotective |
| GLP-1 agonists | GI effects, pancreatitis, thyroid concerns | ↓ MACE, ↓ CV death, ↓ stroke |
| SGLT2 inhibitors | UTI, genital infections, DKA, volume loss | ↓ HF hospitalization, ↓ CV mortality |
| Sulfonylureas | Hypoglycaemia, weight gain | Possible ↑ CV risk (older drugs) |
| Meglitinides | Mild hypoglycaemia, weight gain | Neutral CV effects |
| Thiazolidinediones | Edema, HF, fractures, weight gain | ↑ HF risk (fluid retention); Pioglitazone: ↓ stroke risk |
| DPP-4 inhibitors | Nasopharyngitis, pancreatitis (rare) | Neutral; Saxagliptin: ↑ HF hospitalization |
Table 3: Adverse drug Reactions of the commonly used drugs in Diabetes.
Understanding the pharmacodynamics and side-effect profiles of these agents is crucial for personalizing therapy in obese T2DM patients who are at a risk for cardiac events and for improving glycaemic control while minimizing risks and promoting long-term metabolic health.
Discussion
The recognition of genetic and inflammatory determinants of cardiovascular risk has significant implications for personalized medicine in T2DM. Genetic screening can identify high-risk individuals who may require early aggressive intervention, while inflammatory biomarkers can be used for dynamic monitoring of disease progression and response to therapy. Tailored pharmacotherapy to optimize glycaemic and cardiovascular outcomes could significantly enhance the predictive accuracy beyond conventional risk scores. In this review we present drug-gene interactions of the most widely used drugs for T2DM.
Metformin belongs to an older class of medications in T2DM. Metformin (Glucophage), a synthetic derivative of guanidine, has been in clinical use for over 50 years. Over time, it has become the most widely prescribed oral medication for type 2 diabetes (T2DM), surpassing sulfonylureas. Its widespread use is due to its well-established effectiveness in controlling blood glucose levels, both as a standalone treatment and in combination with various other therapies [23]. Metformin exerts its effects through both AMPK- dependent and AMPK-independent pathways. It works by inhibiting mitochondrial respiration and may also suppress mitochondrial glycerophosphate dehydrogenase. Additionally, its action involves a mechanism associated with the lysosome [24].
Metformin, driven by membrane potentials, accumulates in mitochondria at concentrations up to 1000 times higher than in the extracellular medium due to its positive charge [25]. Metformin primarily affects mitochondria by inhibiting Complex I of the respiratory chain, which leads to a suppression of ATP production [26]. Metformin influences liver metabolism through multiple mechanisms, beginning with its uptake into hepatocytes. This process is facilitated by the organic cation transporter-1 (OCT1) [27], allowing metformin, which is positively charged, to accumulate inside cells and, notably, within mitochondria due to membrane potentials across both the plasma and mitochondrial inner membranes. Once inside the mitochondria, metformin inhibits Complex I, a crucial enzyme in the mitochondrial electron transport chain, which prevents ATP production. This reduction in ATP increases the cytoplasmic ADP: ATP and AMP:ATP ratios, the latter through displacement of the adenylate kinase reaction, ultimately leading to the activation of AMP-activated protein kinase (AMPK) [28]. AMPK can also be activated via a lysosomal mechanism, which involves Axin and the late endosomal/lysosomal adaptor, MAPK, and mTOR activator 1 (LAMTOR1) [29]. The increased AMP:ATP ratio resulting from mitochondrial inhibition not only activates AMPK but also inhibits the enzyme fructose-1,6-bisphosphatase (FBPase), thereby suppressing gluconeogenesis [30]. Another pathway through which AMPK affects metabolism involves the phosphorylation and activation of the enzyme 3′,5′-cyclic phosphodiesterase 4B (PDE4B), which further lowers cAMP levels. In the presence of glucagon, cAMP levels increase, triggering protein kinase A (PKA) activation. PKA, in turn, promotes a shift from glycolysis to gluconeogenesis by phosphorylating and inactivating PFKFB1, decreasing fructose-2,6-bisphosphate (F2,6BP), which is an activator of phosphofructokinase (PFK) and an inhibitor of FBPase. PKA also inhibits the glycolytic enzyme pyruvate kinase (Pyr K) and phosphorylates the transcription factor cAMP response element binding protein (CREB), leading to increased expression of gluconeogenic enzymes like PEPCK and G6Pase [31, 32]. Metformin can sometimes result in a weight loss of about 4kgs or can be weight neutral medication. But when it is being used in combination with sulfonylureas or insulin, it blunts the weight gain induced by these medications [33].
Sulfonylureas can be used in monotherapy or in combination with any other classes of oral diabetic drugs except meglitinides because they lower the glucose levels by a similar mechanism of action [34].
Sulfonylureas function as insulin secretagogues, reducing blood glucose levels by directly stimulating insulin release from pancreatic β-cells, independent of glucose levels [34].
Pancreatic β-cells regulate insulin secretion through the coordinated actions of GLUT2 (a high-Km glucose transporter), glucokinase (which phosphorylates glucose), and glucose metabolism [35]. The second-generation sulfonylureas exhibit similar clinical efficiency as the first- generation sulfonylureas. The drug sulfonylureas do not have linear dose response and the majority A1C reduction occurs at half maximum dose. The effect of sulfonylureas when added to metformin therapy or as a monotherapy on A1C levels varies but results in the reduction of A1C nearly to 0.50-1.5% [36]. The weight gain induced by sulfonylurea therapy also adversely affect the glycaemic control, some studies have shown that sulfonylurea treatment caused weight gain of approximately 3 kgs, which occurred during the first 3-4 years of treatment and then stabilized [37].
| Advantages | Disadvantages |
|---|---|
| Long history of use | Weight gain |
| Rapid acting | Hypoglycaemia |
| Once a day administration is possible | Limited durability |
Table 4: Showing the impact of long term used drugs on humans.
Meglitinides are non-sulfonylurea insulin secretagogues that stimulate insulin release in a glucose-dependent manner, reducing the risk of hypoglycaemia compared to sulfonylureas [38].
What sets meglitinides apart is their rapid onset and short duration of action, making them highly effective as prandial glucose-lowering agents [39]. By targeting post- meal glucose spikes, meglitinides help improve overall glycaemic control while reducing the risk of prolonged insulin release, which is associated with hypoglycaemia in sulfonylureas. The NAVIGATOR study was a large-scale, double-blind, randomized clinical trial that evaluated the effects of nateglinide on cardiovascular outcomes in 9,306 individuals with impaired glucose tolerance (IGT) who also had either pre-existing cardiovascular disease (CVD) or cardiovascular risk factors. Participants were assigned to receive either nateglinide (up to 60 mg three times daily) or a placebo [40], and they were monitored over a period of five years to assess any impact on cardiovascular events. Weight gain is another common side effect of meglitinides, typically ranging from 1 to 3 kg [23, 41]. However, nateglinide leads to less weight gain than repaglinide. These variations in side effects may influence treatment decisions, particularly for patients at higher risk of hypoglycaemia or those concerned about weight management [42].
Thiazolidinediones (TZDs) are a class of insulin- sensitizing drugs that help regulate glucose metabolism by activating peroxisome proliferator-activated receptor-gamma (PPAR-gamma), a nuclear receptor involved in gene expression related to glucose and lipid metabolism. Members of this class include troglitazone (Rezulin), pioglitazone (Actos), and rosiglitazone (Avandia) [23]. TZDs have been found to benefit individuals with polycystic ovarian syndrome (PCOS) by enhancing endothelial function, promoting ovulation, and decreasing insulin resistance [43]. Pioglitazone helps reduce liver fat and may improve fibrosis in patients with nonalcoholic steatohepatitis (NASH). However, other factors and potential risks must be carefully evaluated in NASH patients [44, 45]. A key benefit of TZDs is that they do not induce hypoglycemia when used as monotherapy and can be safely administered to patients with renal disease [46].
By activating peroxisome proliferator-activated receptor-gamma (PPAR-γ), TZDs regulate glucose and lipid metabolism, reducing insulin resistance and improving glycaemic control in individuals with type 2 diabetes [47]. Adiponectin, a cytokine released by adipose tissue, plays a crucial role in improving insulin responsiveness. Additionally, TZD therapy supports fatty acid oxidation, further contributing to metabolic regulation [43, 48], These genes (PPAR-γ), - are expressed in key metabolic tissues, including muscle, fat, and liver, where they play a crucial role in maintaining insulin sensitivity and lipid homeostasis [49].
When TZDs bind to their target, they trigger a conformational change that modifies the expression of multiple genes involved in metabolic regulation. This includes genes encoding lipoprotein lipase, glucokinase, fatty acyl-CoA synthase, and other key enzymes that influence glucose and lipid metabolism [50]. PPAR-gamma agonists help reduce insulin resistance by enhancing the expression of adiponectin and GLUT4, while counteracting the effects of TNF-alpha in adipocytes. The upregulation of GLUT4 facilitates greater glucose uptake in both adipose tissue and skeletal muscle cells in response to insulin, improving overall glucose metabolism [49].
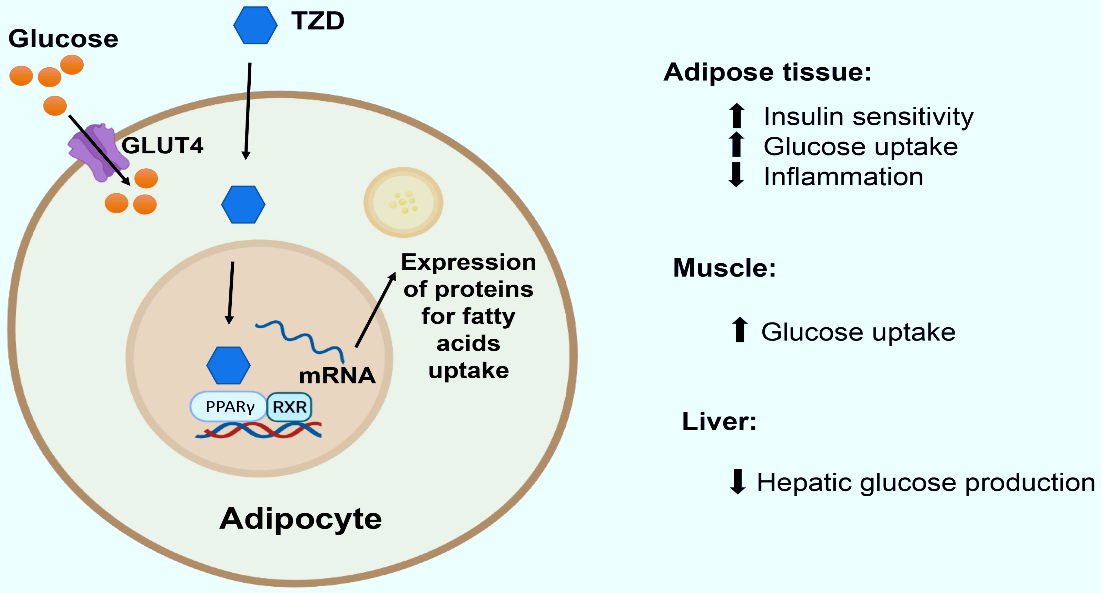
TZDs activate PPARγ receptors in adipose tissue, promoting the absorption of circulating fatty acids into adipocytes [52]. Beyond their role in glycaemic control and insulin resistance improvement, TZDs may also possess anti- inflammatory and anti-cancer properties [53].
The effects of TZDs on cardiovascular disease in type 2 diabetes (T2DM) have been a subject of research, with some studies showing potential benefits. TZDs, such as pioglitazone, have demonstrated the ability to improve several cardiovascular risk factors, including blood pressure, lipid profiles (increasing HDL and decreasing triglycerides), and glycaemic control (lowering A1c). These changes may help reduce the risk of cardiovascular events in patients with T2DM [54].
Polycystic ovary syndrome (PCOS)
TZDs, by enhancing insulin sensitivity, can help reduce circulating androgen levels, improve ovulation rates, and enhance glucose tolerance in patients with polycystic ovary syndrome (PCOS) [55]. Several small trials have indicated that TZDs, when used alongside clomiphene, may offer benefits for improving fertility in women with PCOS. These medications can address some of the underlying metabolic issues that contribute to PCOS, such as insulin resistance, which in turn may improve reproductive outcomes [56]. However, concerns about potential side effects and long- term toxicity have limited their widespread use for treating PCOS specifically. Nevertheless, if a patient with PCOS also has type 2 diabetes and TZDs are selected for managing their diabetes, the beneficial effects on insulin sensitivity may have the added advantage of improving some of the metabolic and reproductive issues associated with PCOS [57]. Dipeptidyl peptidase 4 (DPP-4) inhibitors are a class of antihyperglycemic drugs used to treat type 2 diabetes mellitus, a major risk factor for cardiovascular diseases such as coronary artery disease, heart failure, and stroke [58]. DPP-4 inhibitors, also known as gliptins, are oral medications approved by the FDA for managing type 2 diabetes in adults. The FDA-approved drugs in this class include sitagliptin, saxagliptin, linagliptin, and alogliptin, while vildagliptin is approved by the EMA but not the FDA [59].
These medications work by targeting incretin hormones, which regulate glucose balance following food intake. In addition to their blood sugar-lowering effects, DPP-4 inhibitors offer benefits such as antihypertensive, anti- inflammatory, antiapoptotic, and immunomodulatory effects on the heart, kidneys, and blood vessels, independent of the incretin pathway [60]. They can be prescribed alone or in combination with other diabetes treatments, including metformin, sulfonylureas, thiazolidinediones, or insulin [61].
![Figure 5: Activation of adipose PPARγ receptors by TZDs drives fatty acid uptake into fat cells [51].](/fulltextimages/14063/fig_5.png)
Figure: 6 Basic structure of Dipeptidyl peptidase 4 (DPP-4).
DPP-4 is a widely distributed enzyme that plays a key role in regulating blood sugar by breaking down incretin hormones, primarily GLP-1 (glucagon-like peptide-1) and GIP (gastric inhibitory peptide). These hormones help maintain glucose homeostasis by promoting insulin release and suppressing glucagon secretion, which reduces blood sugar levels [62]. GLP-1 is secreted by enteroendocrine L cells in the small intestine in response to food intake. It lowers blood glucose by stimulating insulin production, decreasing glucagon levels, and slowing gastric emptying, which helps regulate postprandial glucose spikes [63].
These incretin hormones are rapidly broken down, and effects are short-lived. DPP-4 inhibitors work by blocking the action of the DPP-4 enzyme, preventing the breakdown of GLP-1 and GIP. As a result, the levels of these hormones remain elevated for longer duration, leading to sustained insulin secretion from pancreatic [β] cells. This mechanism helps lower both fasting and postprandial blood glucose levels, making DPP-4 inhibitors an effective treatment option for type 2 diabetes [62].
The A1c reduction achieved with DPP-4 inhibitors remains consistent whether they are used alone or in combination with other glucose-lowering medications, and there is no significant difference in efficacy among different DPP-4 inhibitors [65].
They also do not provide cardiovascular protection or help prevent the decline in renal function. Since the glucose- lowering, weight loss, and other effects of oral semaglutide closely resemble those of injectable semaglutide, many experts believe that its impact on cardiovascular and renal outcomes would also be similar [66].
Oral semaglutide offers the advantage of non-injection delivery, making it an appealing option for patients with type 2 diabetes who prefer to avoid injections. It effectively lowers A1c, promotes weight loss, and reduces blood pressure, with minimal serious side effects. However, some patients may find it challenging to follow the specific instructions for proper use of the medication. While the weight loss effect with oral semaglutide is somewhat lower, studies are ongoing to assess higher doses for enhanced weight reduction. It is anticipated that the oral form will also provide the other benefits seen with GLP-1 receptor agonists, such as reducing cardiovascular and renal complications [67].
Conclusion
The therapeutic response to anti-diabetic drugs is not uniform across all patients, and growing evidence highlights the role of genetic interactions in shaping drug efficacy and safety profiles. Pharmacogenomic studies have revealed that genetic polymorphisms in drug-metabolizing enzymes, transporters, and drug targets significantly influence inter- individual variability in response to oral hypoglycaemic agents and insulin sensitizers. For example, variants in the CYP2C9 gene alter the metabolism of sulfonylureas, leading to differences in drug clearance and increased risk of hypoglycaemia in certain carriers. Similarly, polymorphisms in the SLC22A1 gene, encoding the organic cation transporter OCT1, affect metformin uptake in the liver, thereby modifying its glucose-lowering effect.
Genetic interactions also extend to drug targets: mutations in the PPARG gene modulate sensitivity to thiazolidinediones, while variants in the KCNJ11 and ABCC8 genes, which encode components of the pancreatic β-cell KATP channel, influence sulfonylurea response. Moreover, the TCF7L2 gene, one of the strongest genetic risk factors for T2DM, has been consistently linked to differential response to sulfonylureas and metformin, suggesting its role in guiding personalized therapy.
Pharmacogenetic interactions not only aids in predicting treatment outcomes but also reduces the risk of adverse drug reactions, optimizing individualized management of T2DM. With advancements in next-generation sequencing and genome-wide association studies (GWAS), the identification of gene–drug interactions is becoming increasingly precise, paving the way for precision medicine approaches, where therapy is tailored according to each patient’s genetic profile.
Declarations
Conflict of Interest
Authors declare no conflict of Interest.
Financial Aid
This study received no financial aid
Ethics committee Approval
Not required
References
-
Yu HJ, Ho M, Liu X, Yang J, Chau PH, et al. (2023) Incidence and temporal trends in type 2 diabetes by weight status: A systematic review and meta-analysis of prospective cohort studies. J Glob Health 13(1): 04088.
-
Ghouri N, Javed H, Sattar N (2021) Pharmacological Management of Diabetes for Reducing Glucose Levels and Cardiovascular Disease Risk: What Evidence in South Asians?. Curr Diabetes Rev 17(9): e122820189511.
-
Zatterale F, Longo M, Naderi J, Raciti GA, Desiderio A, et al. (2020) Chronic Adipose Tissue Inflammation Linking Obesity to Insulin Resistance and Type 2 Diabetes. Front Physiol 10: 1607.
-
Koyama T, Iinuma S, Yamamoto M, Niimura T, Osaki Y, et al. (2024) International Trends in Adverse Drug Event- Related Mortality from 2001 to 2019: An Analysis of the World Health Organization Mortality Database from 54 Countries. Drug Saf 47(3): 237-249.
-
Dawed AY, Zhou K, Pearson ER (2016) Pharmacogenetics in type 2 diabetes: influence on response to oral hypoglycemic agents. Pharmacogenomics Pers Med 9: 17-29.
-
Yee J, Heo Y, Kim H, Yoon HY, Song G, et al. (2021) Association Between the CYP2C9 Genotype and Hypoglycemia Among Patients With Type 2 Diabetes Receiving Sulfonylurea Treatment: A Meta-analysis. Clin Ther 43(5): 836-843.e4.
-
Sundelin E, Gormsen LC, Jensen JB, Vendelbo MH, Jakobsen S, et al. (2017) Genetic Polymorphisms in Organic Cation Transporter 1 Attenuates Hepatic Metformin Exposure in Humans. Clin Pharmacol Ther 102(5): 841-848.
-
Jang EJ, Lee DH, Im SS, Yee J, Gwak HS (2023) Correlation between PPARG Pro12Ala Polymorphism and Therapeutic Responses to Thiazolidinediones in Patients with Type 2 Diabetes: A Meta-Analysis. Pharmaceutics 15(6): 1778.
-
Pearson ER, Donnelly LA, Kimber C, Whitley A, Doney AS, et al. (2007) Variation in TCF7L2 influences therapeutic response to sulfonylureas: a GoDARTs study. Diabetes 56(8): 2178-2182.
-
Proks P, Reimann F, Green N, Gribble F, Ashcroft F (2002) Sulfonylurea stimulation of insulin secretion. Diabetes 51 S3: 68-76.
-
Kalra S, Bahendeka S, Sahay R, Ghosh S, Md F, et al. (2018) Consensus Recommendations on Sulfonylurea and Sulfonylurea Combinations in the Management of Type 2 Diabetes Mellitus - International Task Force. Indian J Endocrinol Metab 22(1): 132-157.
-
Dutta S, Shah RB, Singhal S, Dutta SB, Bansal S, et al. (2023) Metformin: A Review of Potential Mechanism and Therapeutic Utility Beyond Diabetes. Drug Des Devel Ther 17: 1907-1932.
-
Quinn CE, Hamilton PK, Lockhart CJ, McVeigh GE (2008) Thiazolidinediones: effects on insulin resistance and the cardiovascular system. Br J Pharmacol 153(4): 636-645.
-
Kernan WN, Viscoli CM, Furie KL, Young LH, Inzucchi SE, et al. (2016) Pioglitazone after Ischemic Stroke or Transient Ischemic Attack. N Engl J Med 374(14): 1321- 1331.
-
Nissen SE, Wolski K (2007) Effect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes. N Engl J Med 356(24): 2457- 2471.
-
Makrilakis K (2019) The Role of DPP-4 Inhibitors in the Treatment Algorithm of Type 2 Diabetes Mellitus: When to Select, What to Expect. Int J Environ Res Public Health 16(15): 2720.
-
Scirica BM, Bhatt DL, Braunwald E, Steg PG, Davidson J, et al. (2013) Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N Engl J Med 369(14): 1317-1326.
-
Saisho Y (2020) SGLT2 Inhibitors: the Star in the Treatment of Type 2 Diabetes?. Diseases 8(2): 14.
-
Confederat LG, Dragostin OM, Condurache MI (2025) SGLT2 Inhibitors and the Risk of Urogenital Infections: A Concise Review. J Clin Med 14(6): 1960.
-
Liu QK (2024) Mechanisms of action and therapeutic applications of GLP-1 and dual GIP/GLP-1 receptor agonists. Front Endocrinol 15: 1431292.
-
Kristensen SL, Rørth R, Jhund PS, Docherty KF, Sattar N, et al. (2019) Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet Diabetes Endocrinol 7(10): 776-785.
-
Pakkir Maideen NM, Manavalan G, Balasubramanian K (2018) Drug interactions of meglitinide antidiabetics involving CYP enzymes and OATP1B1 transporter. Ther Adv Endocrinol Metab 9(8): 259-268.
-
Tahrani AA, Barnett AH, Bailey CJ (2016) Pharmacology and therapeutic implications of current drugs for type 2 diabetes mellitus. Nat Rev Endocrinol 12(10): 566-592.
-
Rena G, Hardie DG, Pearson ER (2017) The mechanisms of action of metformin. Diabetologia 60(9): 1577-1585.
-
Bridges HR, Jones AJ, Pollak MN, Hirst J (2014) Effects of metformin and other biguanides on oxidative phosphorylation in mitochondria. Biochem J 462(3): 475-487.
-
El-Mir MY, Nogueira V, Fontaine E, Avéret N, Rigoulet M, et al. (2000) Dimethylbiguanide inhibits cell respiration via an indirect effect targeted on the respiratory chain complex I. J Biol Chem 275(1): 223-228.
-
Wang DS, Jonker JW, Kato Y, Kusuhara H, Schinkel AH, et al. (2002) Involvement of organic cation transporter 1 in hepatic and intestinal distribution of metformin. J Pharmacol Exp Ther 302(2): 510-515.
-
Hawley SA, Ross FA, Chevtzoff C, Green KA, Evans A, et al. (2010) Use of cells expressing gamma subunit variants to identify diverse mechanisms of AMPK activation. Cell Metab 11(6): 554-565.
-
Zhang CS, Li M, Ma T, Zong Y, Cui J, et al. (2016) Metformin Activates AMPK through the Lysosomal Pathway. Cell Metab 24(4): 521-522.
-
Vincent MF, Marangos PJ, Gruber HE, Van den Berghe G (1991) Inhibition by AICA riboside of gluconeogenesis in isolated rat hepatocytes. Diabetes 40(10): 1259-1266.
-
Koo SH, Flechner L, Qi L, Zhang X, Screaton RA, et al. (2005) The CREB coactivator TORC2 is a key regulator of fasting glucose metabolism. Nature 437(7062): 1109- 1111.
-
Patel K, Foretz M, Marion A, Campbell DG, Gourlay R, et al. (2014) The LKB1-salt-inducible kinase pathway functions as a key gluconeogenic suppressor in the liver. Nat Commun 5: 4535.
-
Sanchez-Rangel E, Inzucchi SE (2017) Metformin: clinical use in type 2 diabetes. Diabetologia 60(9): 1586-1593.
-
Thulé PM, Umpierrez G (2014) Sulfonylureas: a new look at old therapy. Curr Diabetes Rep 14(4): 473.
-
Prentki M, Matschinsky FM, Madiraju SR (2013) Metabolic signaling in fuel-induced insulin secretion. Cell Metab 18(2): 162-185.
-
Maloney A, Rosenstock J, Fonseca V (2019) A Model- Based Meta-Analysis of 24 Antihyperglycemic Drugs for Type 2 Diabetes: Comparison of Treatment Effects at Therapeutic Doses. Clin Pharmacol Ther 105(5): 1213- 1223.
-
Khunti K, Chatterjee S, Gerstein HC, Zoungas S, Davies MJ (2018) Do sulphonylureas still have a place in clinical practice?. Lancet Diabetes Endocrinol 6(10): 821-832.
-
Anderson M, Powell J, Campbell KM, Taylor JR (2014) Optimal management of type 2 diabetes in patients with increased risk of hypoglycemia. Diabetes Metab Syndr Obes 7: 85-94.
-
Guardado-Mendoza R, Prioletta A, Jiménez-Ceja LM, Sosale A, Folli F (2013) The role of nateglinide and repaglinide, derivatives of meglitinide, in the treatment of type 2 diabetes mellitus. Arch Med Sci 9(5): 936-943.
-
NAVIGATOR Study Group, Holman RR, Haffner SM, McMurray JJ, Bethel MA, et al. (2010) Effect of nateglinide on the incidence of diabetes and cardiovascular events. N Engl J Med 362(16): 1463-1476.
-
Tran L, Zielinski A, Roach AH, Jende JA, Householder AM, et al. (2015) Pharmacologic treatment of type 2 diabetes: oral medications. Ann Pharmacother 49(5): 540-556.
-
Rosenstock J, Hassman DR, Madder RD, Brazinsky SA, Farrell J, et al. (2004) Repaglinide versus nateglinide monotherapy: a randomized, multicenter study. Diabetes Care 27(6): 1265-1270.
-
Yau H, Rivera K, Lomonaco R, Cusi K (2013) The future of thiazolidinedione therapy in the management of type 2 diabetes mellitus. Curr Diabetes Rep 13(3): 329-341.
-
Musso G, Cassader M, Paschetta E, Gambino R (2017) Thiazolidinediones and Advanced Liver Fibrosis in Nonalcoholic Steatohepatitis: A Meta-analysis. JAMA Intern Med 177(5): 633-640.
-
He L, Liu X, Wang L, Yang Z (2016) Thiazolidinediones for nonalcoholic steatohepatitis: A meta-analysis of randomized clinical trials. Medicine 95(42): e4947.
-
Clemens KK, O’Regan N, Rhee JJ (2019) Diabetes Management in Older Adults With Chronic Kidney Disease. Curr Diabetes Rep 19(3): 11.
-
Yamanouchi T (2010) Concomitant therapy with pioglitazone and insulin for the treatment of type 2 diabetes. Vasc Health Risk Manag 6: 189-197.
-
Vieira R, Souto SB, Sánchez-López E, Machado AL, Severino P, et al. (2019) Sugar-Lowering Drugs for Type 2 Diabetes Mellitus and Metabolic Syndrome-Review of Classical and New Compounds: Part-I. Pharmaceuticals 12(4): 152.
-
Tyagi S, Gupta P, Saini AS, Kaushal C, Sharma S (2011) The peroxisome proliferator-activated receptor: A family of nuclear receptors role in various diseases. J Adv Pharm Technol Res 2(4): 236-240.
-
Choi SS, Park J, Choi JH (2014) Revisiting PPARγ as a target for the treatment of metabolic disorders. BMB Rep 47(11): 599-608.
-
Mahgoub MO, Ali II, Adeghate JO, Tekes K, Kalász H, et al. (2023) An Update on the Molecular and Cellular Basis of Pharmacotherapy in Type 2 Diabetes Mellitus. Int J Mol Sci 24(11): 9328.
-
Ahmadian M, Suh JM, Hah N, Liddle C, Atkins AR, et al. (2013) PPARγ signaling and metabolism: the good, the bad and the future. Nat Med 19(5): 557-566.
-
Ialenti A, Grassia G, Di Meglio P, Maffia P, Di Rosa M, et al. (2005) Mechanism of the anti-inflammatory effect of thiazolidinediones: relationship with the glucocorticoid pathway. Mol Pharmacol 67(5): 1620-1628.
-
Tripathy D, Solis-Herrera C, Ryder REJ (2021) Cardioprotective Effects of Pioglitazone in Type 2 Diabetes. Diabetes Spectr 34(3): 243-247.
-
Froment P, Touraine P (2006) Thiazolidinediones and Fertility in Polycystic Ovary Syndrome (PCOS). PPAR Res 2006: 73986.
-
Ghazeeri G, Kutteh WH, Bryer-Ash M, Haas D, Ke RW (2003) Effect of rosiglitazone on spontaneous and clomiphene citrate-induced ovulation in women with polycystic ovary syndrome. Fertil Steril 79(3): 562-566.
-
Brettenthaler N, De Geyter C, Huber PR, Keller U (2004) Effect of the insulin sensitizer pioglitazone on insulin resistance, hyperandrogenism, and ovulatory dysfunction in women with polycystic ovary syndrome. J Clin Endocrinol Metab 89(8): 3835-3840.
-
Bonora E, Cigolini M (2016) DPP-4 inhibitors and cardiovascular disease in type 2 diabetes mellitus. Expectations, observations and perspectives. Nutr Metab Cardiovasc Dis 26(4): 273-284.
-
Lim SW, Jin JZ, Jin L, Jin J, Li C (2015) Role of dipeptidyl peptidase-4 inhibitors in new-onset diabetes after transplantation. Korean J Intern Med 30(6): 759-770.
-
Lim SW, Jin JZ, Jin L, Jin J, Li C (2015). Role of dipeptidyl peptidase-4 inhibitors in new-onset diabetes after transplantation. The Korean journal of internal medicine 30(6): 759-770.
-
Rosenstock J, Brazg R, Andryuk PJ, Lu K, Stein P, et al. (2006) Efficacy and safety of the dipeptidyl peptidase-4 inhibitor sitagliptin added to ongoing pioglitazone therapy in patients with type 2 diabetes: a 24-week, multicenter, randomized, double-blind, placebo- controlled, parallel-group study. Clinical therapeutics 28(10): 1556-1568.
-
Capuano A, Sportiello L, Maiorino MI, Rossi F, Giugliano D, et al. (2013) Dipeptidyl peptidase-4 inhibitors in type 2 diabetes therapy--focus on alogliptin. Drug design, development and therapy 7: 989-1001.
-
Gupta V, Kalra S (2011) Choosing a gliptin. Indian journal of endocrinology and metabolism 15(4): 298-308.
-
Wikipedia (2025) Dipeptidyl peptidase-4 inhibitor. The Free Encyclopedia.
-
Scheen AJ (2012) DPP-4 inhibitors in the management of type 2 diabetes: a critical review of head-to-head trials. Diabetes & metabolism 38(2): 89-101.
-
Husain M, Birkenfeld AL, Donsmark M, Dungan K, Eliaschewitz FG, et al. (2019) Oral Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. The New England journal of medicine 381(9): 841-851.
-
Andersen A, Knop FK, & Vilsbøll T (2021) A Pharmacological and Clinical Overview of Oral Semaglutide for the Treatment of Type 2 Diabetes. Drugs 81(9): 1003-1030.
- Pattern of Gonadal Hormones in Oral Testosterone-Supplimented Male Wistar Rats with Diabetes-Induced Hypogonadism
- Re-Evaluation of the Genotoxicity of Currently Used Food Dyes in Mouse Multiple Organs Via Continuous Administration by Drinking Using the Comet Assay
- Exploratory Proteomic Profiling of SARS-CoV-2 Infected THP-1 Macrophages Reveals Alterations in Inflammatory Response and Cellular Metabolism
- Study of Genotoxicity of Hepatocarcinogens in Multiple Organs in Mice by Feeding and Drinking Using the Comet Assay
- Spirulina Polypeptides Inhibit the Growth of Human Lung Tumor (H460) Cells
- The Role of Faculty in Assessment: Traditional vs. Competency- Based Medical Education in Toxicology Learning