Effects of 5-HTP and Melatonin on the Sleep Cycle of Medical Students
The hormone Melatonin and the amino acid 5-Hydroxytryptophan (5-HTP) directly and indirectly affect your sleeping habits, which can result in several beneficial effects. This study observed the effects of 5-HTP and melatonin administration on the sleep cycles of medical students, who are continually under the pressures of school, resulting in improper sleeping habits and unregulated sleeping cycles, resulting in low levels of melatonin. Sixty-six students received three treatments: 5-HTP (50mg), Melatonin (5mg), and placebo, in a randomized, double-blind study. Each procedure was administered for 21 days, with reflex and cognitive tests conducted after each week, along with maintaining a daily sleep log and dream journal. The altering effects of the treatments on the sleep cycle of the subjects were successfully seen in this study. Reflex speed, along with the cognitive functions test, showed a significant positive increase for the 5-HTP group, while the Melatonin group showed significantly higher sleep periods along with an increase in the frequency of dreams. There were no significant changes for the placebo group throughout the experiment. Overall alertness and mood were increased for the 5-HTP group, while there was a decline in alertness for the melatonin group. 5-HTP exerted a modest benefit in improving the sleep quality of students, while Melatonin successfully improved the amount of sleep students were receiving.
Introduction
The pineal gland is one of several endocrine glands in our body found only in vertebrates [1]. It is located behind the third cerebral ventricle in between the two cerebral hemispheres of the brain [1, 2]. The size of the pineal gland is large in children, but as humans progress through puberty, the gland begins to shrink to a length of 0.8cm with a weight of 0.1g [3, 4]. Melatonin is a hormone that is indirectly derived from the amino acid tryptophan; this hormone is responsible for the sleep/wake cycle, which helps govern our circadian rhythm [5, 6, 7, 8]. The sleep cycle has five stages, which are produced in 90-minute cycles. Sleep is divided into two conditions: the first being non-rapid eye movement (NREM), which contains the first four stages of the sleep cycle [9]. The second condition of the sleep cycle is called rapid eye movement (REM), which contains stage 5 of the sleep cycle [2]. The first stage represents the time between wakefulness and sleep. The duration of stage one may last 10-15 minutes but may be variable depending on the state of the individual [1, 9]. Stage two represents the longest period of the sleep cycle and occupies approximately 50% of the sleep cycle [9]. Stage 2 sleep consists of two brain activity states, the first being a theta wave state, which shows higher brain activity; this is carried over from the first stage of sleep to the second [1, 9].
After approximately 10-20 minutes of stage 2, brain waves move into slower brain activity called delta waves, which last for approximately 15-30 minutes [6, 9]. The evidence of delta waves signifies the start of stage 3 and transition into stage 4 of the sleep cycle; this represents the deepest part of sleep, where the body’s restorative capabilities are increased [10]. The fifth and last stage of the sleep cycle is characterized by eye movement and is associated with dreaming.
The body is temporarily paralyzed in this state, where muscles relax, but neurological and metabolic functions become more active [11]. The sleep cycle does not progress through the stages chronologically, instead, the body starts at the first stage of sleep and then progresses to stages two, three, and four, after stage four, stages two and three are repeated before the body goes into its final stage 5; after the completion of stage 5, the body will restart the cycle from stage 2 [9].
Melatonin is derived from tryptophan, which is naturally obtained from food sources. Tryptophan is then converted into 5-Hydroxytryptophan, which is further converted into serotonin [12]. The human body converts serotonin to melatonin, which is stored in the pineal gland [3]. The secretion of melatonin in the body is controlled by the amount of light that passes the retina. Low-light environments, such as nighttime, trigger the release of melatonin, creating the effects of sleepiness and allowing the human body to fall asleep [13, 14, 15].
Low levels of melatonin in the human body can cause delayed sleep phase cycle, insomnia, and headaches, which can indirectly lead to more severe side effects such as depression, loss of appetite, and weight gain [16, 17, 18, 19]. The production of melatonin can be stimulated in various ways to produce the beneficial effects of increased melatonin secretion.
5-Hydroxytryptophan is produced from tryptophan and is an intermediary compound for the production of serotonin [12]. 5-HTP is extracted from the Griffonia plant and is shown to be one of the most effective ways to increase serotonin levels in the brain, therefore directly influencing the increase of melatonin production [12]. 5-HTP increases the quality of sleep by increasing the amount of deep sleep (stages 3 and 4) and shortening light sleep (stages 1 and 2), without affecting the overall duration of sleep [12, 20]. Melatonin can also be increased by taking a melatonin supplement, which helps in falling asleep faster and allows for less disturbed sleep.
The difference between taking 5-HTP and melatonin is that with melatonin, the beneficial effects of the serotonin system are not seen [21]. 5-HTP also manipulates the sleep stages, allowing better sleep and shorter necessary naps. This is due to the ability of 5-HTP to bypass the brain’s light regulation system [12, 13, 14, 15, 16, 17, 18, 19, 20, 21]. Therefore, allowing the body to secrete melatonin regardless of the amount of light exposure [12, 13, 14, 15, 16, 17, 18, 19, 20, 21].
The main objective of this study is to understand the effects of 5-HTP and melatonin in medical students who are continuously under the pressures of school, resulting in sleep deprivation and an improper sleeping cycle. This study will look at the different effects of 5-HTP and melatonin and how each supplement positively changes the sleep behaviour of students, resulting in a change in alertness, sleep patterns, and mood.
Subjects and Methods
Subjects
On approval by the Saint James School of Medicine research committee and drug approval by the IRB. Sixty- six (66) Medical students attending Saint James School of Medicine participated after providing informed consent. After baseline observation and participant survey, it was concluded that most participants were sleep-deprived. For this experiment, willing subjects underwent a health history to make sure no drug reaction occurred, maintaining the quality of the results. Participants falling under the following criteria were excluded from this experiment: currently taking antidepressants, pregnant/currently breastfeeding, high blood pressure or on blood pressure medication, diabetes, or a previous history of seizures.
During the experiment, participants were asked to refrain from using dextromethorphan (Robitussin and other cough syrups) or any Triptans (used for migraines and headaches), along with not driving or using machinery for four to five hours after taking the treatment. Participants using 5-HTP or melatonin might exhibit the following side effects: headache, short-term feelings of depression, daytime sleepiness, dizziness, stomach cramps, and irritability.
Methods
Participants will be asked to take pills of 5-HTP (50mg), melatonin (5mg), or a placebo (avicil) 2 hours before their normal bedtime. Participants are to resume their everyday normal activities, and at the end of the day, before their next dosage, are to record their results. Before beginning the supplement, dosing participants will undergo a motor and cognitive function test.
Part 1
This part of the experiment comprises the participant attempting the ruler drop test along with a cognitive skills/ memory test. Participants will also be asked for their previous health history, along with their sleeping patterns, before they begin to conduct the study.
Motor Reflex Test
Place the ruler between thumb and index finger approximately one inch above the hand, with both digits placed two inches apart. Drop the ruler and measure the length at which the participant stops the ruler from falling; repeat three times
Cognitive Memory Test
The researcher asks the participant to recite the alphabetical/numerical combination in order, with only two errors allowed. (Each participant will be given a new randomly generated alpha/numerical combination)
Part 2
In this part of the experiment, the participants will receive a package with pills of 5-HTP, melatonin, or an identical placebo. Participants will also be given a daily chart recording their results at the end of each day, with their first day being without the supplementation. Participants will also be asked to keep a sleep diary, along with recording any dreams.
Part 3
In this part of the experiment, the participants will once again attempt the ruler drop test along with a cognitive skills/memory test after each week before their next dosage.
Statistical Analysis
We used SPSS for Windows for statistical analysis. Data was confirmed for normality, and parametric tests were done. Using ANOVA, we compared reflex, cognition (alphabetical/ numerical), duration of sleep, and alertness during the day among the three treatments. Tukey HSD test was done between the treatment groups if ANOVA showed significance. Significance was defined at p < 0.05.
Results
A total of sixty-six participants were compliant (77.6%) out of eighty-five participants, 23 in the 5-HTP group, 20 in the Melatonin group, and 23 in the placebo. Those excluded from the analysis (19) were either non-compliant with medication intake or study procedures or were excluded from the experiment on medical grounds.
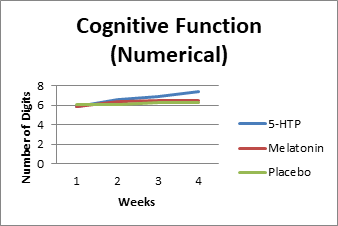
Figure 1 below represents the numerical cognitive function value for the three groups over 3 weeks, with week 1 representing the initial baseline observation. After 3 weeks, an increase in cognitive skill can be seen in the 5-HTP group. Table 1 outlines the observations made for the numerical part of the cognitive test along with individual group means. ANOVA (Table 2) showed a significant value between the groups, which was further analyzed with the Tukey HSD (Table 3), which showed a significant p-value for 5-HTP when compared to melatonin (p=0.04) and placebo (p<0.001).
| N | Mean | Std. Deviation | Std. Error | 95% Confidence Interval for Mean | Minimum | Maximum | ||
|---|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||||
| 5-HTP (1) | 69 | 6.9275 | 0.79185 | 0.09533 | 6.7373 | 7.1178 | 5 | 8 |
| Melatonin (2) | 60 | 6.45 | 0.83209 | 0.10742 | 6.235 | 6.665 | 5 | 9 |
| Placebo (3) | 69 | 6.2174 | 0.85525 | 0.10296 | 6.0119 | 6.4228 | 4 | 9 |
| Total | 198 | 6.5354 | 0.87623 | 0.06227 | 6.4126 | 6.6582 | 4 | 9 |
Table 1: Statistics for Numerical Cognitive Function.
Between Groups 18.026 2 9.013 13.19 .000*
Within Groups 133.23 195 0.683
Sum of Squares df Mean Square F Sig.
Total 151.25 197
*P<0.05 (Sig=Significant) Table 2: ANOVA analysis for numerical cognitive function.
| (I) Drug | (J) Drug | Mean Difference (I-J) | Std. Error | Sig. | 95% Confidence Interval | |
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||
| 1 | 2 | .47754* | 0.146 | .004* | 0.1329 | 0.8221 |
| 3 | .71014* | 0.141 | .000* | 0.3778 | 1.0425 | |
| 2 | 1 | -.47754* | 0.146 | .004* | -0.822 | -0.1329 |
| 3 | 0.23261 | 0.146 | 0.251 | -0.112 | 0.5772 | |
| 3 | 1 | -.71014* | 0.141 | .000* | -1.043 | -0.3778 |
| 2 | -0.23261 | 0.146 | 0.251 | -0.577 | 0.112 |
Table 2: Tukey HSD analysis for comparative significance.
5-HTP (1), Melatonin (2), Placebo (3). *P<0.05 (Sig=Significant). Table 3: Tukey HSD analysis for comparative significance.
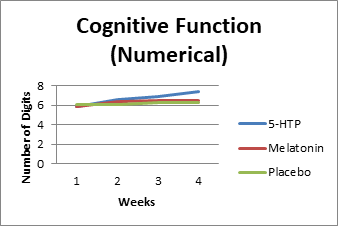
Figure 2 below represents the alphabetical cognitive function value for the three groups over 3 weeks, with week 1 representing the initial baseline observation. After 3 weeks, an increase in cognitive skill can be seen in the 5-HTP group. Table 4 outlines the observations made for the alphabetical part of the cognitive test along with individual group means.
ANOVA (Table 5) showed a significant value between the groups, which was further analyzed with the Tukey HSD (Table 6), which showed an insignificant p-value for 5-HTP when compared to melatonin (p=0.066) and a significant value when compared to the placebo group (p=0.032).
| N | Mean | Std. Deviation | Std. Error | 95% Confidence Interval for Mean | Minimum | Maximum | ||
|---|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||||
| 1 | 69 | 6.7101 | 0.80625 | 0.09706 | 6.5165 | 6.9038 | 5 | 9 |
| 2 | 60 | 6.35 | 0.89868 | 0.11602 | 6.1178 | 6.5822 | 5 | 9 |
| 3 | 69 | 6.3188 | 1.00722 | 0.12126 | 6.0769 | 6.5608 | 5 | 9 |
| Total | 198 | 6.4646 | 0.92141 | 0.06548 | 6.3355 | 6.5938 | 5 | 9 |
Table 3: Statistics for alphabetical cognitive function.
| Sum of Squares | df | Mean Square | F | Sig. | |
|---|---|---|---|---|---|
| Between Groups | 6.414 | 2 | 3.207 | 3.888 | .022* |
| Within Groups | 160.838 | 195 | 0.825 | ||
| Total | 167.253 | 197 |
Table 4: ANOVA analysis for alphabetical cognitive function.
*P<0.05 (Sig=Significant) Table 5: ANOVA analysis for alphabetical cognitive function.
| (I) Drug | (J) Drug | Mean Difference (I-J) | Std. Error | Sig. | 95% Confidence Interval | |
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||
| 1 | 2 | 0.36014 | 0.16031 | 0.066 | -0.0185 | 0.7388 |
| 3 | .39130* | 0.15462 | .032* | 0.0261 | 0.7565 | |
| 2 | 1 | -0.36014 | 0.16031 | 0.066 | -0.7388 | 0.0185 |
| 3 | 0.03116 | 0.16031 | 0.979 | -0.3475 | 0.4098 | |
| 3 | 1 | -.39130* | 0.15462 | .032* | -0.7565 | -0.0261 |
| 2 | -0.03116 | 0.16031 | 0.979 | -0.4098 | 0.3475 |
Table 5: Tukey HSD analysis for comparative significance.
5-HTP (1), Melatonin (2), Placebo (3). *P<0.05 (Sig=Significant). Table 6: Tukey HSD analysis for comparative significance.
Figure 3 below represents the reflex test for the three groups over 3 weeks, with week 1 representing the initial baseline observation. After 3 weeks an increase in reflex response can be seen in the 5-HTP group, with a slight increase in both the melatonin and placebo groups. Table 7 outlines the observations made for the reflex test along
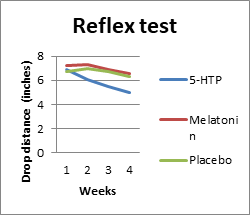
with individual group means. ANOVA (Table 8) showed a significant value between the groups which was further analyzed with the Tukey HSD (Table 9) which showed a significant p-value for 5-HTP when compared to melatonin (p<0.001) and placebo group (p<0.001).
| N | Mean | Std. Deviation | Std. Error | 95% Confidence Interval for Mean | Minimum | Maximum | ||
|---|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||||
| 1 | 69 | 5.5226 | 1.03821 | 0.12499 | 5.2732 | 5.772 | 3 | 8.33 |
| 2 | 60 | 6.91 | 1.53191 | 0.19777 | 6.5143 | 7.3057 | 2.5 | 10 |
| 3 | 69 | 6.6633 | 1.41021 | 0.16977 | 6.3245 | 7.002 | 3.66 | 9.33 |
| Total | 198 | 6.3405 | 1.45977 | 0.10374 | 6.1359 | 6.5451 | 2.5 | 10 |
Table 6: Statistics for the reflex test.
| Sum of Squares | df | Mean Square | F | Sig. | |
|---|---|---|---|---|---|
| Between Groups | 72.807 | 2 | 36.404 | 20.458 | .000* |
| Within Groups | 346.983 | 195 | 1.779 | ||
| Total | 419.791 | 197 |
Table 7: ANOVA analysis for reflex test.
*P<0.05 (Sig=Significant). Table 8: ANOVA analysis for reflex test.
| (I) Drug | (J) Drug | Mean Difference (I-J) | Std. Error | Sig. | 95% Confidence Interval | |
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||
| 1 | 2 | -1.38741* | 0.23547 | .000* | -1.9435 | -0.8313 |
| 3 | -1.14068* | 0.22711 | .000* | -1.677 | -0.6043 | |
| 2 | 1 | 1.38741* | 0.23547 | .000* | 0.8313 | 1.9435 |
| 3 | 0.24672 | 0.23547 | 0.548 | -0.3094 | 0.8028 | |
| 3 | 1 | 1.14068* | 0.22711 | .000* | 0.6043 | 1.677 |
| 2 | -0.24672 | 0.23547 | 0.548 | -0.8028 | 0.3094 |
Table 8: Tukey HSD analysis for comparative significance for reflex test between groups.
5-HTP (1), Melatonin (2), Placebo (3). *P<0.05 (Sig=Significant). Table 9: Tukey HSD analysis for comparative significance for reflex test between groups.
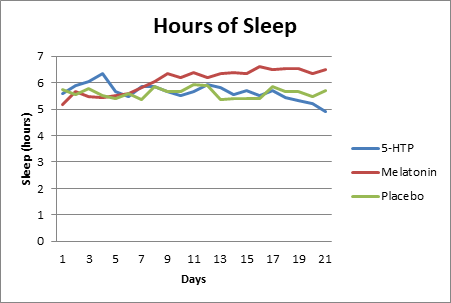
Figure 4 below represents the hours of sleep for the three groups over 3 weeks, with week 1 representing the initial baseline observation. After 3 weeks, an increase in sleep duration can be seen in the melatonin group. Table 10 outlines the observations made for the duration of sleep with individual group means. ANOVA (Table 11) showed a significant value between the groups, which was further analyzed with the Tukey HSD (Table 12), which showed an insignificant p-value for 5-HTP when compared to placebo (p=0.874) and a significant value for the melatonin group when compared to the placebo (p<0.001).
| N | Mean | Std. Deviation | Std. Error | 95% Confidence Interval for Mean | Minimum | Maximum | ||
|---|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||||
| 5-HTP | 483 | 5.6491 | 1.29455 | 0.0589 | 5.5333 | 5.7648 | 1 | 10 |
| Melatonin | 420 | 6.0869 | 1.25514 | 0.06124 | 5.9665 | 6.2073 | 2.5 | 9 |
| Placebo | 483 | 5.6087 | 1.25614 | 0.05716 | 5.4964 | 5.721 | 2 | 10 |
| Total | 1386 | 5.7677 | 1.28591 | 0.03454 | 5.6999 | 5.8354 | 1 | 10 |
Table 9: Statistics for hours of sleep.
| Sum of Squares | df | Mean Square | F | Sig. | |
|---|---|---|---|---|---|
| Between Groups | 61.803 | 2 | 30.902 | 19.178 | .000* |
| Within Groups | 2228.389 | 1383 | 1.611 | ||
| Total | 2290.192 | 1385 |
Table 10: ANOVA analysis for hours of sleep.
*P<0.05 (Sig=Significant). Table 11: ANOVA analysis for hours of sleep.
| (I) Drug | (J) Drug | Mean Difference (I-J) | Std. Error | Sig. | 95% Confidence Interval | |
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||
| 5-HTP | Melatonin | -.43784* | 0.08469 | .000* | -0.6365 | -0.2391 |
| Placebo | 0.04037 | 0.08168 | 0.874 | -0.1513 | 0.232 | |
| Melatonin | 5-HTP | .43784* | 0.08469 | .000* | 0.2391 | 0.6365 |
| Placebo | .47821* | 0.08469 | .000* | 0.2795 | 0.6769 | |
| Placebo | 5-HTP | -0.04037 | 0.08168 | 0.874 | -0.232 | 0.1513 |
| Melatonin | -.47821* | 0.08469 | 0 | -0.6769 | -0.2795 |
Table 11: Tukey HSD analysis for comparative significance for hours of sleep between groups.
*P<0.05 (Sig=Significant). Table 12: Tukey HSD analysis for comparative significance for hours of sleep between groups.
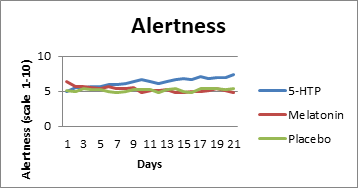
Figure 5 below represents the alertness during the day for the three groups over 3 weeks, with week 1 representing the initial baseline observation. After 3 weeks, an increase in cognitive skill can be seen in the 5-HTP group. Table 13 outlines the observations made for the alertness, along with individual group means. ANOVA (Table 14) showed a significant value between the groups, which was further analyzed with the Tukey HSD (Table 15), which showed a significant p-value for 5-HTP when compared to melatonin (p<0.001) and a significant value when compared to the placebo group (p<0.001).
| N | Mean | Std. Deviation | Std. Error | 95% Confidence Interval for Mean | Minimum | Maximum | ||
|---|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||||
| 5-HTP | 482 | 6.2946 | 1.69882 | 0.07738 | 6.1426 | 6.4466 | 1 | 10 |
| Melatonin | 420 | 5.2738 | 1.60957 | 0.07854 | 5.1194 | 5.4282 | 1 | 10 |
| Placebo | 483 | 5.1553 | 1.29582 | 0.05896 | 5.0394 | 5.2711 | 1 | 10 |
| Total | 1385 | 5.5877 | 1.62521 | 0.04367 | 5.5021 | 5.6734 | 1 | 10 |
Table 12: Statistics for hours of sleep.
| Sum of Squares | df | Mean Square | F | Sig. | |
|---|---|---|---|---|---|
| Between Groups | 372.559 | 2 | 186.28 | 78.415 | .000* |
| Within Groups | 3283.032 | 1382 | 2.376 | ||
| Total | 3655.591 | 1384 |
Table 13: ANOVA analysis for hours of sleep.
*P<0.05 (Sig=Significant). Table 14: ANOVA analysis for hours of sleep.
| (I) Drug | (J) Drug | Mean Difference (I-J) | Std. Error | Sig. | 95% Confidence Interval | |
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||
| 5-HTP | Melatonin | 1.02080* | 0.10288 | .000* | 0.7794 | 1.2622 |
| Placebo | 1.13933* | 0.09923 | .000* | 0.9065 | 1.3721 | |
| Melatonin | 5-HTP | -1.02080* | 0.10288 | .000* | -1.2622 | -0.7794 |
| Placebo | 0.11853 | 0.10283 | 0.482 | -0.1227 | 0.3598 | |
| Placebo | 5-HTP | -1.13933* | 0.09923 | .000* | -1.3721 | -0.9065 |
| Melatonin | -0.11853 | 0.10283 | 0.482 | -0.3598 | 0.1227 |
Table 14: Tukey HSD analysis for comparative significance for hours of sleep between groups.
*P<0.05 (Sig=Significant). Table 15: Tukey HSD analysis for comparative significance for hours of sleep between groups.
Discussion
The present study examines the effects of 5-HTP and melatonin on students who are continuously under the rigorous pressures of medical school resulting in sleep deprivation and an improper sleeping cycle. This study looks at the different effects of 5-HTP and melatonin and how each supplement positively changes the sleep behaviour of students, resulting in a change in alertness, sleep patterns, and mood.
5-HTP increases the quality of sleep by increasing the amount of deep sleep (stages 3 and 4) and shortening light sleep (stages 1 and 2), without affecting the overall duration of sleep [12, 20]. A better quality of sleep can have several beneficial effects on short-term memory and the storage of long-term memory. In this experiment, we conducted a cognitive functions test on all three groups with separate tests for numerical and alphabetical memory. When comparing 5-HTP to the placebo group for the numerical cognitive test (Table 3), we got a significant p-value (p<0.001), and when looking at the alphabetical cognitive test (Table 6), we also got a significant p-value (p<0.032). Comparing the melatonin group to the placebo group, we received insignificant values for the numerical test (Table 3) (p=0.251) and alphabetical test (Table 6) (p=0.979). The statistical analysis of the cognitive functions test suggests a positive correlation between an increase in cognitive function and the use of 5-HTP in sleep-deprived individuals.
Administration of 5-HTP allows for stimulation of the serotonin system. This can be seen through an improvement in other body functions, such as reaction time to a visual stimulus. In this experiment, a reflex test was conducted to test the reaction speed of the subjects after each week; an increase in reaction speed is evidence of higher alertness and focus. When comparing the results of the reflex test (Table 9) for 5-HTP to the placebo group, we observed a significant increase in reaction speed (p<0.001), whereas for the melatonin group, there was no significant change compared to the placebo group (p=0.548). The increase in reflex seen in the 5-HTP group was expected, as increased serotonin levels help improve reflexes and reactions to stimuli.
The secretion of melatonin in the body is controlled by the amount of light that passes the retina; low light environments, such as nighttime, trigger the release of melatonin, creating the effects of sleepiness and allowing the human body to fall asleep [13, 14, 15]. An increase of exogenous melatonin is known to increase the amount of sleep a person receives, whereas 5-HTP will allow for better quality of sleep without increasing the duration [13, 22]. When looking at the hours of sleep each participant received (Figure 4), we can conclude that the melatonin group had an increase in the number of hours of sleep they received each night when compared to the placebo group (p<0.001). When comparing 5-HTP to the placebo group, we observed that it is insignificant (p=0.874). This result was expected as 5-HTP does not increase the amount of sleep an individual receives. Participants of the melatonin group reported a higher number of dreams along with more vivid visuals; this is most likely due to melatonin’s properties of initiating deeper cycles of sleep, allowing for longer periods of dreaming. Participants also found it harder to wake up in the mornings and felt sleepy during the day.
When comparing the outcome in Figure 5, we observed that there is an increase in alertness for the 5-HTP group when compared to the placebo group. We observed a significant difference (p<0.001), but when the melatonin group is compared to the placebo, no significant change is noted (p=0.482). The observation was as expected, as an increase of serotonin in the CNS will increase attention and alertness, which is evident from the result collected in this study; an increase in alertness could also be a factor influencing the increase seen in the reflex test. Participants of the 5-HTP group reported feeling more awake and an increase in concentration.
This study had a few limitations. We used sleep logs to evaluate hours of sleep; using a more definitive method, such as actigraphy to monitor sleep, might have given more accurate results; however, considering the cooperative nature of the students and the full knowledge of properly recording the sleep logs, the disadvantages of a subjective sleep log can be overcome at least to a certain extent. Also, it was not possible to measure circadian markers such as core body temperature in our sample of students. If this value could have been obtained, we could have had a better understanding of the phase-shifting value of melatonin.
Conclusion
The study was successful with observation of results; we can see the sleep-altering effects of 5-HTP and Melatonin.
The observations made for the respective groups were expected, as 5-HTP has a more active effect on sleep cycles by manipulating the stages, allowing for longer deep sleep (stages 3 and 4) while shortening light sleep (stages 1 and 2) without altering the overall duration of sleep. Melatonin was noted to have a more passive role in sleep stages due to its ability to increase deep sleep. We also saw an increase in total sleep time, while at the same time, a decline in alertness was observed. The main objective of this study was to understand the effects of 5-HTP and melatonin on medical students whose sleep deprivation was mostly attributed to an improper sleeping cycle, leading to low levels of melatonin, causing a delayed sleep phase cycle. Administering 5-HTP, an indirect method of increasing melatonin, and administering exogenous melatonin, we were able to observe the different effects the respective drugs had on the sleep cycle of subjects and were able to note the positive changes in the sleep behavior of students.
Conflict of Interest
None
Funding
None
References
-
Dawson D, Encel N (1993) Melatonin and sleep in humans. Journal of pineal research 15(1): 1-12.
-
Kocher L, Brun J, Borson‐Chazot F, Gonnaud PM, Claustrat B (2006) Increased REM sleep associated with melatonin deficiency after pinealectomy: a case study. Chronobiology International 23(4): 889-901.
-
Macchi MM, Bruce JN (2004) Human pineal physiology and functional significance of melatonin. Frontiers in neuroendocrinology 25(3-4): 177-195.
-
Reiter RJ (1992) The ageing pineal gland and its physiological consequences. Bioessays 14(3): 169-175
-
Arendt J, Deacon S (1997) Treatment of circadian rhythm disorders–melatonin. Chronobiology international 14(2): 185-204.
-
Cajochen C, Kräuchi K, Wirz‐Justice A (2003) Role of melatonin in the regulation of human circadian rhythms and sleep. Journal of neuroendocrinology 15(4): 432-437.
-
Zee PC, Reid KJ (2016) Melatonin in sleep-wake regulation. InInsomnia, CRC Press, pp: 426-432.
-
Zhdanova IV, Lynch HJ, Wurtman RJ (1997) Melatonin: a sleep-promoting hormone. Sleep 20(10): 899-907.
-
James SP, Mendelson WB, Sack DA, Rosenthal NE, Wehr TA (1987) The effect of melatonin on normal sleep. Neuropsychopharmacology: official publication of the American College of Neuropsychopharmacology 1(1): 41-44.
-
Lewy AJ, Sack RL (1997) Exogenous melatonin’s phase- shifting effects on the endogenous melatonin profile in sighted humans: a brief review and critique of the literature. Journal of Biological Rhythms 12(6): 588-594.
-
Stone BM, Turner C, Mills SL, Nicholson AN (2000) Hypnotic activity of melatonin. Sleep 23(5): 663-669.
-
Birdsall TC (1998) 5-Hydroxytryptophan: a clinically- effective serotonin precursor. Alternative medicine review: a journal of clinical therapeutic 3(4): 271-280.
-
Lewy AJ, Wehr TA, Goodwin FK, Newsome DA, Markey SP (1980) Light suppresses melatonin secretion in humans. Science 210(4475): 1267-1269.
-
Suhner A, Schlagenhauf P, Johnson R, Tschopp A, Steffen R (1998) Comparative study to determine the optimal melatonin dosage form for the alleviation of jet lag. Chronobiology international 15(6): 655-666.
-
Yoon IY, Song BG (2002) Role of morning melatonin administration and attenuation of sunlight exposure in improving adaptation of night-shift workers. Chronobiology International 19(5) :903-913.
-
Dahlitz M, Alvarez B, Parkes JD, English J, Arendt J, et al. (1991) Delayed sleep phase syndrome response to melatonin. The Lancet 337(8750): 1121-1124.
-
De Giorgis G, Miletto R, Iannuccelli M, Camuffo M, Scerni S (1987) Headache in association with sleep disorders in children: a psychodiagnostic evaluation and controlled clinical study--L-5-HTP versus placebo. Drugs under experimental and clinical research 13(7): 425-433.
-
Haimov I, Lavie P, Laudon M, Herer P, Vigder C, et al. (1995) Melatonin replacement therapy of elderly insomniacs. Sleep 18(7): 598-603.
-
MacFarlane JG, Cleghorn JM, Brown GM, Streiner DL (1991) The effects of exogenous melatonin on the total sleep time and daytime alertness of chronic insomniacs: a preliminary study. Biological psychiatry 30(4): 371- 376.
-
Touret M, Sarda N, Gharib A, Geffard M, Jouvet M (1971) The role of 5-hydroxytryptophan (5- HTP) in the regulation of the sleep/wake cycle in parachlorophenylalanine (p-CPA) pretreated rat: a multiple approach study. Experimental brain research 86(1): 117-124.
-
Wyatt RJ, Zarcone V, Engelman K, Dement WC, Snyder F, et al. (1971) Effects of 5-hydroxytryptophan on the sleep of normal human subjects. Electroencephalography and clinical neurophysiology 30(6): 505-509.
-
Petre-Quadens O, De Greef A (1971) Effects of 5-HTP on sleep in mongol children: Preliminary results. Journal of the Neurological Sciences 13(1): 115-119.
- Adsorption of Bisphenol A on NH4OH- Modified Rice Husk and Sugar Cane Bagasse Biochar
- Comparative Assessment of the Reinforcement Efficiency of Palm Fruit Fibre and Coconut Fibre in High Density Polyethylene (HDPE) Matrix Composite
- Importance of Bio Compounds Naturally Present in Food with Functionality in Animal Metabolism
- Sub-Acute Study on the Cardiotoxic Effects of Monosodium Glutamate Ingestion in Albino Rat
- Weight Management and Its Natural Solutions: A Review
- Pharmacokinetics of the Tyrosine Kinase Inhibitor, Alectinib