A Recalcitrant Case of Eosinophilic Pustular Folliculitis
Eosinophilic Pustular Folliculitis (EPF) or papulooerythroderma of Ofuji (PEO) is a rare dermatosis that presents with recurrent pruritic follicular papules and pustules that can involve the entire skin surface sparing the skin folds. This can be accompanied with elevated IgE levels and eosinophils. Diagnosis has been challenging due to its ability to mimic several common dermatologic disorders, such as acne and contact dermatitis. Literature has described the first line of therapy to be oral and topical indomethacin, however, success has been variable, and reports have been anecdotal. Until this day, there is yet to be standard guidelines for approach to diagnosis and management of this condition. In this article, we report a case of a 29 year-old female of Chinese descent who presented with papules on bilateral malar and nasal areas recalcitrant to topical corticosteroids. She demonstrated success with the use of a monthly regimen of isotretinoin after a perplexing diagnostic dilemma.
Introduction
Eosinophilic Pustular Folliculitis or papuloerythroderma of Ofuji is a rare dermatosis of unknown etiology characterized by chronic recurrent crops of pruritic papules and pustules in a follicular distribution that can cover entire skin, sparing the skin folds, accompanied with eosinophilia and elevated IgE [1]. The most common subset of population affected consists of males with Asian descent [2]. Literature reported three variants of the disease: classic EPF, infantile EPF, and immunosuppression-associated EPF, which is primarily HIV related [3, 4]. While the etiology of the disorder remains unclear, it has been speculated that the dysregulation of the immune system has been found to be involved in its development, particularly of the T-helper (Th) 2 and Th22 cells [5]. Some evidence suggests involvement of cytokines and adhesion molecules that activate the follicular unit [6]. There remains no uniform consensus regarding treatment for any subtype of EPF. Anecdotal evidence supports the use of indomethacin (oral and topical), narrow band UVB, tetracyclines, and corticosteroids in treating EPF [1, 7, 8], with only a handful of reports suggesting the successful use of isotretinoin [6, 9]. We report a case of EPF and its challenging therapeutic approach.
Case
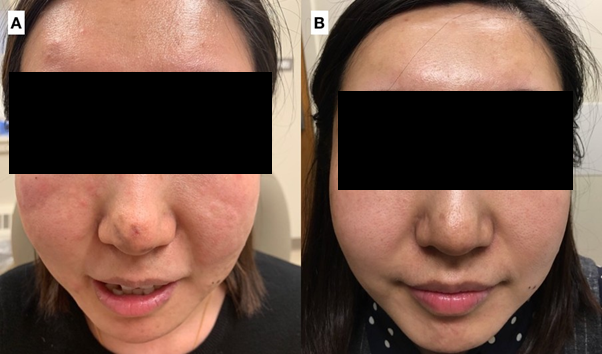
A 29-year-old Chinese female presented to our dermatology office with a 1-month history of a worsening pruritic eruption of papules on the face. Prior treatment included ketoconazole cream, hydrocortisone 1% cream and antihistamines without improvement. Patient was otherwise well with no other underlying medical problems or skin conditions and denied use of any new personal hygiene products. The eruption was also not associated with any aggravating factors, including sunlight or alcohol. Clinical examination was notable for multiple erythematous follicular papules and plaques on bilateral malar and nasal areas. Pruritus was graded 2-4 out of 10 (on scale of 1-10 with 10 being most pruritic) (Figure 1a).
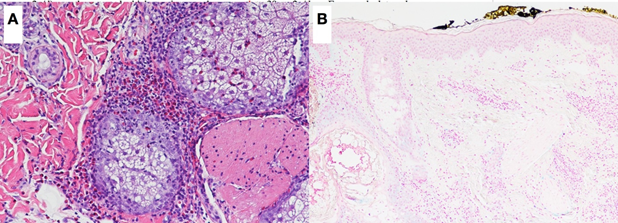
Laboratory workup was notable for slight peripheral eosinophilia on presentation of 6% or 0.6 absolute eosinophil count (Normal value (NV): 0.0-0.4 x10E3/uL). The rest of the blood work including hepatitis panel, sexually transmitted disease panel, G6PD and pregnancy tests were negative Initial differential diagnosis included acne, rosacea, irritant contact dermatitis, mycosis fungoides, and sarcoidosis. The patient was started on a mid-potent topical steroid twice daily for four weeks without improvement. On her second visit, a 4-mm punch biopsy from the left cheek was performed with histopathology revealing perifollicular infiltrate with eosinophils (Figure 2a). The CD4:8 ratio was normal, CD7 was preserved and CD30 failed to show staining. PAS and Gomori’s methenamine silver (GMS) stain were negative for organisms, and slight intrafollicular mucin was highlighted by colloidal iron stain (Figure 2b). A T-cell receptor gene rearrangement was performed given the inflammatory infiltrate and mucin, but it did not show a clonal population. Taken together, histopathology was consistent with EPF.
A 3-month trial of oral indomethacin (25mg 3x/d) was initiated with nearly complete resolution after the first month of treatment with recurrence two weeks after discontinuation. Oral isotretinoin was then started. Four weeks into oral isotretinoin treatment, patient reported resolution of facial lesions and pruritus (Figure 1b). She completed a nine-month course of isotretinoin with a cumulative dose of 210mg/kg and an average dose of 0.5- 1.5mg/kg/day. Patient was completely clear of lesions for 6 months off isotretinoin. Thereafter, patient would experience few pruritic papules recurring once a month, for which patient would take a single dose of 40mg isotretinoin monthly with continued birth control use. Patient has been on this regimen for 24 months with no complaints and normal laboratory workup.
Discussion
Although HIV-associated EPF is the prevalent variant, our patient presented with negative HIV serologic result [1]. Laboratory tests showed eosinophilia which has been described to be found in EPF cases. However, due to its nonspecific presentation as seen in our patient, it can easily mimic other commonly diagnosed conditions, such as acne, rosacea, and contact dermatitis. As such, histopathology in our case was a necessary step to arrive at the correct diagnosis.
The pathogenesis of EPF remains unclear, however it has been proposed that the lesions are caused by both a proliferation of eosinophils and an increase in chemotactic factors leading to eosinophilic chemotaxis at the pilosebaceous follicle [7]. Isotretinoin is a retinoic acid derivative FDA-approved for the treatment of severe and intractable acne vulgaris and various disorders of keratinization. We hypothesize that isotretinoin’s success in treating this case of EPF would be due to its inhibition of the eosinophilic chemotactic factors that can be found in sebaceous glands and the stratum corneum [10].
Widely accepted treatment recommendations for EPF are limited, especially for idiopathic cases, with treatment algorithms created based on anecdotal evidence from case series and reports. Dapsone and indomethacin have classically been proposed as first line therapy with variable success, and only two case reports show the efficacy of isotretinoin in recalcitrant disease [6, 9]. Considering the rarity of this disease, we hope reporting our case will contribute to the growing literature supporting oral isotretinoin in the treatment of EPF. Much is still needed to learn on the pathogenesis and management of this condition.
References
-
Brito FF, Martelli AC, Cavalcante ML, Pinto AC, Itimura G, et al. (2016) Ofuji disease: a rare der- matosis and its challenging therapeutic approach. An Bras Dermatol 91(5): 646-648.
-
Lewis HM, Shahsavari A, Goodman MB (2022) Papuloerythroderma of Ofuji. Island (FL): StatPearls Publishing.
-
Nomura T, Katoh M, Yamamoto Y, Miyachi Y, Kabashima K (2016) Eosinophilic pustular folliculitis: A proposal of diagnostic and therapeutic algorithms. J Dermatol 43(11): 1301-1306.
-
Nomura T, Katoh M, Yamamoto Y, Miyachi Y, Kabashima K (2016) Eosinophilic pustular folliculitis: A published work-based comprehensive analysis of therapeutic responsiveness. J Dermatol 43(8): 919-927.
-
Desai K, Miteva M, Romanelli P (2021) Papuloerythroderma of Ofuji. Clin Dermatol 39(2): 248- 255.
-
Patrone P, Bragadin G, Stinco G, De Francesco V, Frattasio A (2001) Ofuji’s disease: Diagnostic and therapeutic problems. A report of three cases. Int J Dermatol 40(8): 512-515.
-
Kinoshita Y, Kono T, Ansai, S, Saeki H (2019) An aggressive case of granulomatous eosinophilic pustular folliculitis on the face. JAAD Case Reports 5(3): 237-239.
-
Damiani G, Pacifico A, Scarabello A, Iacovelli P, Conic RRZ, et al. (2019) SUSPECTED eosinophilic pustular folliculitis presenting as rapidly evolving acneiform eruption . J Eur Acad Dermatology Venereol 34(1): e43-e44.
-
Berbis P, Jancovici E, Lebreuil G, Benderitter T, Debuertret L, et al. (1989) Eosinophilic Pustular Folliculitis (Ofuji’s Disease): Efficacy of Isotretinoin. Dermatologica 179(4): 214-216.
-
Dwivedi M, Sharma V, Pathak K (2017) Pilosebaceous targeting by isotretinoin-loaded invasomal gel for the treatment of eosinophilic pustular folliculitis: optimization, efficacy and cellular analysis. Drug Dev Ind Pharm 43(2): 293-304.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling