Abrikosoff’s Tumor: A Case Report
A 68-year-old patient had, for about 7 months, in the right buttock, a nodule of about 2 cm in diameter, rosy colour, centrally ulcerated, of hard consistency, asymptomatic. Histological examination and immunohistochemical investigations deposed for the diagnosis of granular cell tumour (Abrikosoff tumour). Granular cell tumour is a neoplasm in most cases benign, characterised by voluminous cells with eosinophilic cytoplasm and grainy appearance, with the granules corresponding to lysosomes. It is currently considered a variant of schwannoma, although cases with different histogenesis have been described. This tumour, most frequently localised on the dorsal surface of the tongue, very rarely affects the skin.
Introduction
Granular Cell Tumor (GCT), or Abrikosoff’s Tumor, is a very rare tumor arising in soft tissues. It was first described in 1926 by the Russian pathologist Abrikosoff. By then, only a few cases have been reported [1, 2]. It is almost always a benign neoplasm; however, malignancy is believed to occur in 1-2% of cases [1, 2, 3, 4, 5]. GCT is more common between the ages of 40 and 60, while very few cases have been described before the age of 20. Women are affected twice as men, and black ethnic groups are more affected than the Caucasian population [2, 6]. GCT affects the skin or mucosa of head or neck (45% –65%); more than half of these cases are found in the oral cavity, mainly in the tongue (23% –28%), other organs being more rarely affected [1, 2]. Both benign and malignant GCT present as a well-circumscribed, asymptomatic, slow-growing, solitary, sessile nodule. It is usually solitary; however, multiple lesions have been reported. Malignant GCT may be suspected when the size is greater than 4 cm; there is a subcutaneous localization, rapid growth, and extensive overlying ulceration [1, 2, 4, 6]. Cases associated with Noonan syndrome, neurofibromatosis, and Hodgkin lymphoma have been reported [2, 7, 8].
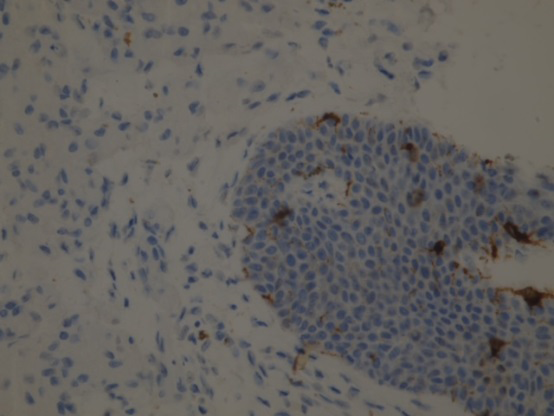
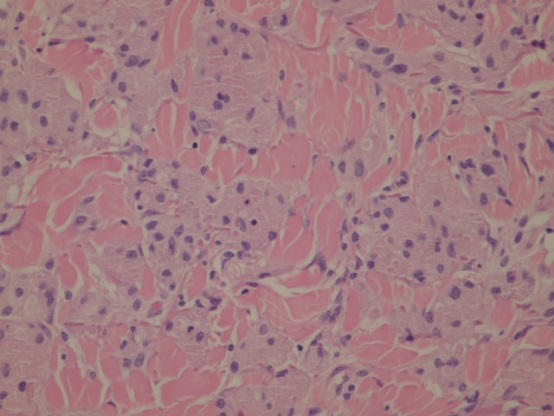
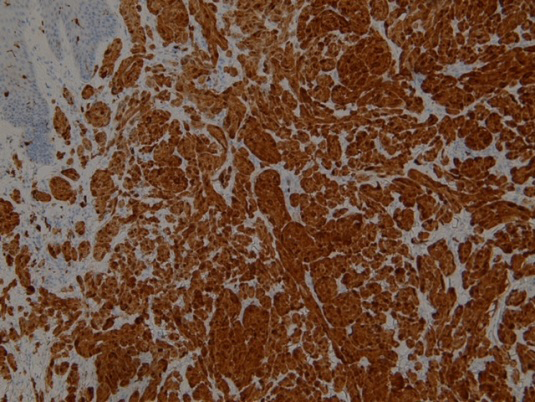
A 69-year-old male was first referred to us because of a painless, mobile nodule in the intergluteal area. It was pink in color, with central ulceration and hard consistency (Figure 1). It appeared about seven months before our observation and had grown to a diameter of about 2 cm over time. The patient was otherwise well and not taking any medication. The nodule was surgically excised. Histology showed a proliferation of cells with large eosinophilic and granular cytoplasm and relatively monomorphic nuclei with small nucleoli; the mitoses were numerous, even atypical; the cells were arranged in nest and trabeculae, ulcerating the epidermis; there were no pieces of evidence aspects of vascular permeation (Figure 2). Immunohistochemistry
was positive for S100(+), C68(+) (Figure 3, ENS (+/-), CD56(+), vimentin(+), Ki67 (+/-) (Figures 3 & 4). Therefore, a diagnosis of benign GCT was made. Currently, at a 6-month follow-up, there is no recurrence.

Discussion
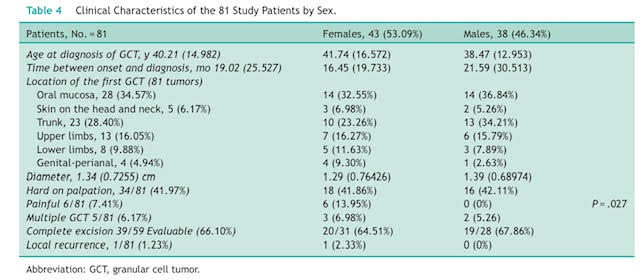
GCT is a rare neoplasm generally occurring in adults and is reported to be more common in women and black people. One case was described in a child at the site of BCG vaccine inoculation [1, 3, 4, 6, 7]. Rarely, familial cases have been reported.8 It appears as a single, slow-growing nodule, ranging in color from pink to gray to brown, asymptomatic. It can be multiple in 10-25% of cases, rarely reaching a large size. Traumatic fibroma is a typical reactive lesion that should be mainly included in the differential diagnosis. Furthermore, GCT can be misdiagnosed with leiomyoma, dermatofibrosarcoma, or angiosarcoma [1, 2, 3, 4, 6, 7, 8]. Head and neck are the most common arising sites of GCT, especially the anterior part of the tongue, and the oral cavity are the most frequently interested. Other locations are the breast, chest wall, respiratory tract, esophagus, vulva, bladder, perianal area, stomach, appendix, and parotid gland. GCT tumor in the limbs is very rare (Table 1) [1, 2, 5, 7, 8]. Diagnosis is histopathological; imaging is helpful for studying the tumor in internal organs [6]. Tumor histogenesis is controversial. Currently, GCT is considered as having a neural or nerve sheath origin, probably arising from Schwann cell. The preference for an area with high peripheral nerves density, such as the mouth, confirms this hypothesis [1, 2, 4]. Histology shows polygonal cells arranged in sheets with granular eosinophilic cytoplasm, small nuclei with PAS-positive, and diastase-resistant granules (accumulation of lysosomes). This picture is rather non-specific and can also be observed in several non-neural tumors, including those arising from smooth muscle, connective tissue, neuroglia, endothelial, and epithelial cells.
Furthermore, GCT shows connective tissue separated from the surrounding structures by dense fibrous proliferative tissue with a pseudoepitheliomatous surface, sometimes leading to the misdiagnosis of squamous cell carcinoma; however, rare cases of coexistence of the two tumors have been reported [1, 2, 4, 5]. Given these diagnostic challenges, immunohistochemistry is often required. GCT cells are negative for myoglobin, human black melanoma-45 (HMB-45), and glial fibrillar acidic protein (GFAP), while they are positive for the S-100, CD-68, receptor factor protein S-100, nerve growth 5, neuron-specific enolase, inhibinα, a transcription factor associated with microphthalmia and protein gene product 9.5. Positivity for S-100, CD-68, and neuron-specific enolase supports neural origin [1, 2]. Malignant GCT is rare, occurring in 1-2% of cases and causing death in about 40% of cases. There are no well- defined criteria for the diagnosis of malignancy, the main being rapid growth, size >4–5cm, ulceration, involvement of subcutaneous tissue, vascular and adjacent tissue invasion, atypic and mitotic figures (>2 mitoses per 10 high-power fields at x200 magnification), necrosis, vesicular nuclei with prominent nucleoli, cell spindling, high nuclear to cytoplasmatic ratio, and pleomorphism. Tumors with three or more of these features are considered malignant [1, 2, 4, 6]. However, some authors reported that only the presence of metastases is an accepted criterion for malignancy [1, 2]. The treatment of choice is surgical excision with free margins [1, 2, 8]. Recurrence is uncommon for benign GCT, although more frequent for multiple tumors. On the other hand, malignant GCT usually relapses within one year, with metastases occurring in 1%–3% of all cases, especially to the lymph nodes and lungs [1, 2, 4].
References
-
Almeida CEC, Caroço T, Silva M, Albano MN (2017) Abrikossoff’stumour on the upper limb: a rare presentation. BMJ Case Rep, pp: bcr2017222006.
-
Dell’Horto AG, Pinto JM, Diniz MS (2013) What is your diagnosis? An Bras Dermatol 88: 469–47.
-
Alnashwan YA, Ali KAH, Amr SS (2019) Metastasizing Malignant Granular Cell Tumor (Abrikossoff Tumor) of the Anterior Abdominal Wall, with Prolonged Survival. Case Rep Pathol pp: 9576487.
-
Pushpa G, Karve PP, Subashini K, Narasimhan MN, Ahmad PB (2013) Abrikossoff’s Tumor: An Unusual Presentation. Indian J Dermatol 58(5): 407.
-
Sposto MR, Navarro CM, De Andrade CR (2006) Granular cell tumour (Abrikossoff’stumour): case series. Oral Oncology Extra 42(50): 194-197.
-
Barca I, Cordaro R, Giudice A, Cristofaro MG (2020) Abrikossoff’s tumor of the tongue: Report of three cases and review of the literature. J Oral Maxillofac Pathol 24(1): 101-105.
-
Marcoval J, Bauer-Alonso A, Llobera-Ris C, Moreno- Vilchez C, Penin RM, et al. (2021) Granular Cell Tumor: A Clinical Study of 81 Patients. Actas Dermosifiliogr (Engl Ed) 112(5): 441-446.
-
Ferraz PND, Danu V, Almeida R, Figueiredo J (2020) Granular cell tumour (Abrikossoff’stumour) of the tongue. BMJ Case Rep 13(7): e235637.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling