A Rare Manifestation of Porokeratosis
A 45-year-old female presented with multiple dark coloured, severely itchy lesions all over the body since three years. On examination, there were multiple discrete as well as coalescing geographical plaques with central clearing and hyperpigmented raised irregular borders distributed over face including post auricular area, neck, upper chest, lower abdomen, groins, buttocks as well as bilateral upper and lower limbs.
Dear Editor,
A 45-year-old female presented with multiple dark coloured, severely itchy lesions all over the body since three Letter to Editor years. On examination, there were multiple discrete as well as coalescing geographical plaques with central clearing and hyperpigmented raised irregular borders distributed over face including post auricular area, neck, upper chest, lower abdomen, groins, buttocks as well as bilateral upper and lower limbs (Figures A-F).
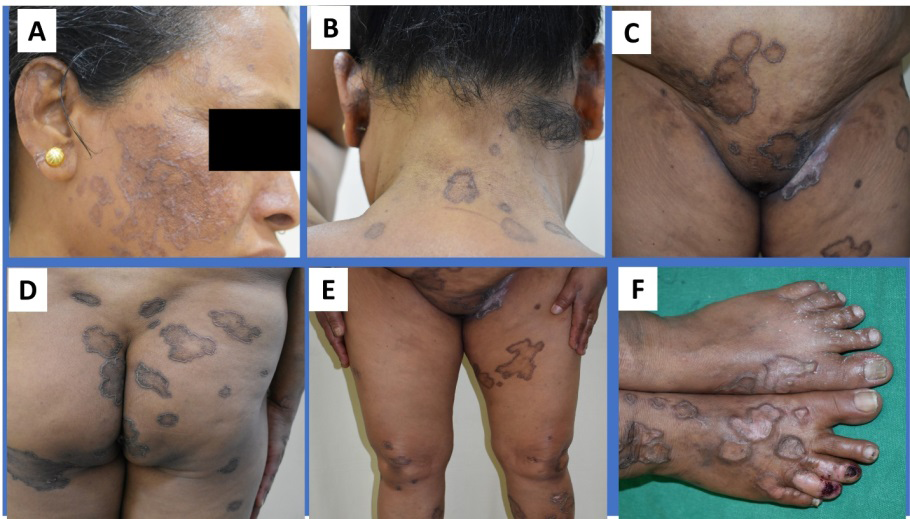
Figure 1A-F: Multiple plaques of porokeratosis disseminated over different body parts.
On the scalp, there were two such plaques in the midline- one over the frontal scalp and the other over the vertex (Figures 2A & B).
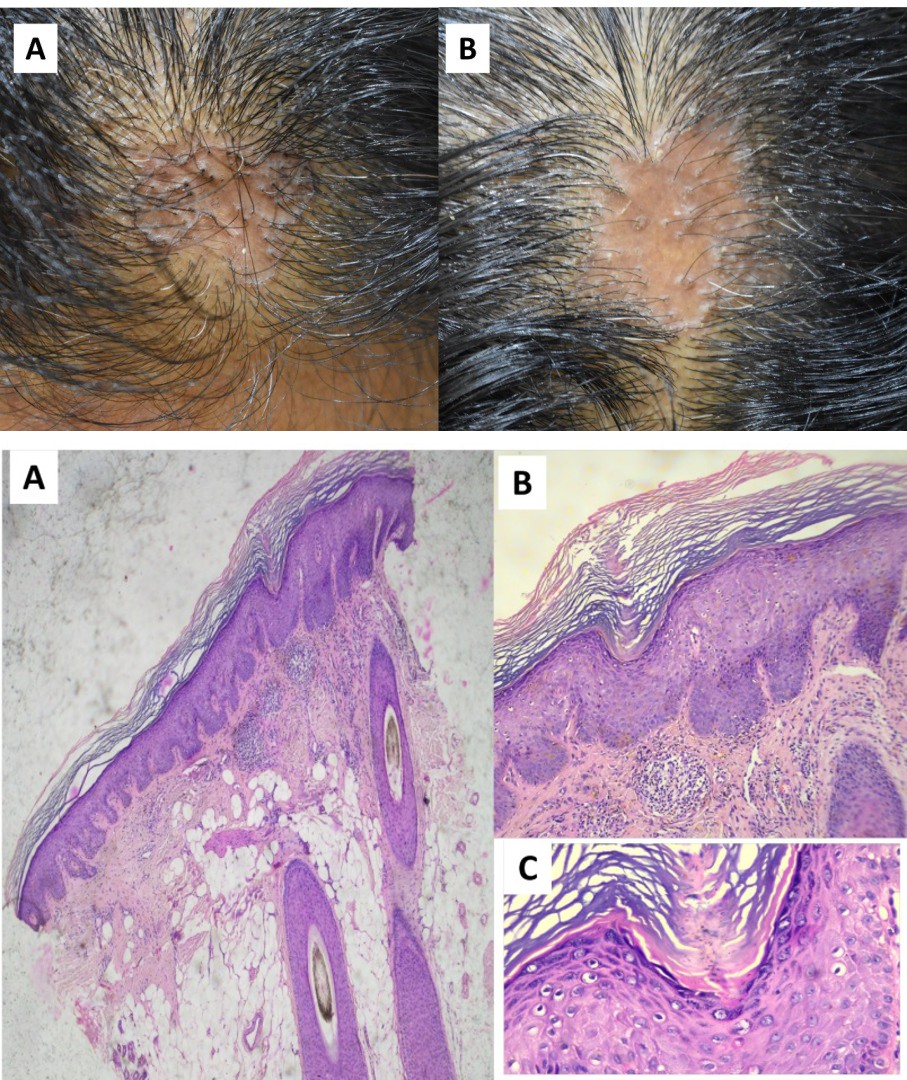
Figures 2A & B: Plaque associated with scarring alopecia on the A) Frontal scalp B) Vertex.
The center was shiny and atrophic with almost complete hair loss. Histopathology from the plaque on right forearm revealed hyperkeratosis, focal areas of parakeratosis and horny lamella with a collection of chronic inflammatory cells below. The plaque on the scalp had hyperkeratosis, focal spongiosis, perivascular collection of chronic inflammatory infiltrate and increased collagen (Figures 3 A-C).
Figures 3A-C: Histopathological section (H&E stain) of plaque on scalp showing hyperkeratosis, focal areas of parakeratosis and horny lamella with a perivascular collection of chronic inflammatory cells below at (A)10X, (B) 40X and (C) 100X.
Thus, we diagnosed the condition as Disseminated Superficial porokeratosis with secondary cicatricial alopecia.
Porokeratosis is a disorder of epidermal keratinization which may be either genetic or acquired and has several clinical variants described in literature [1, 2]. However, being a disorder of keratinization, it has mainly epidermal changes like cornoid lamellae, hyperkeratosis, hypogranulosis, and occasionally dyskeratotic cells with little/no dermal involvement. Hence, cicatricial alopecia was a rare, unexpected and surprising finding which instigated us to probe further.
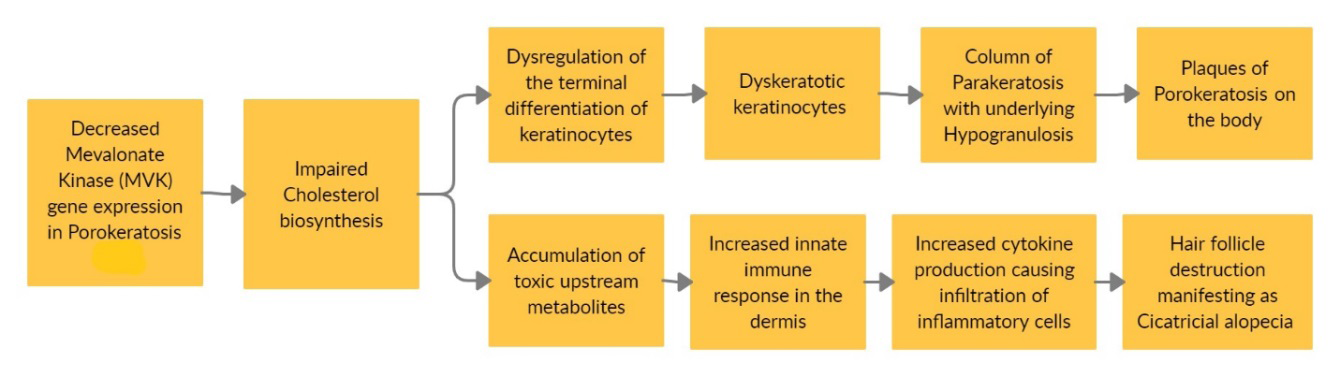
A study done by Liu Yin, et al. [3] found mutations in the Mevalonate Kinase (MVK) gene involved in cholesterol biosynthesis in 50% of the subjects with DSAP. The resultant decreased activity of Mevalonate Protein Kinase adversely affects keratinocyte differentiation. Another study done by Sreejith, et al. [4] unraveled a decreased expression of MVK gene in Primary Cicatricial alopecia. They concluded that changes in the cholesterol milieu in the hair follicle can trigger an innate immune response. Thus, on losing their immune privilege, the hair follicles get destroyed by the infiltrating inflammatory cells. Lihi Atzmony, et al. [5] hypothesized that topical cholesterol/lovastatin could alleviate porokeratosis by targeting the pathogenesis and found that it resulted in near complete clearance of DSAP lesions after 4 weeks of therapy.
Based on the above validations, we propose that the cause of cicatricial alopecia in this patient can be an underlying gene mutation associated with the cholesterol synthesis pathway. The resulting irregular keratinization manifests on the skin as lesions of porokeratosis and on the scalp as delayed inner root sheath disintegration. The hair follicle gets occluded and hence there is a retrograde hair growth leading to rupture of the follicle and a foreign body reaction against its contents in the dermis. The incoming inflammatory cells lead to hair follicle destruction and subsequent fibrosis manifesting clinically as scarring alopecia (Figure 4).
It is a very rare clinical manifestation and can be a diagnostic dilemma if the sole presentation is as patches of cicatricial which we think needs reporting so that when we are describing the causes of cicatricial alopecias, we should keep in mind that very rarely, porokeratosis is a cause.
References
-
Jha AK, Sonthalia S, Lallas A (2017) Dermoscopy of Porokeratosis of Mibelli. Indian Dermatol Online J 8(4): 304-305.
-
Lanka P, Lanka LR, Manivachagam D (2015) Punctate Porokeratosis Palmaris et Plantaris. Indian J Dermatol 60(3): 284-286.
-
Liu Y, Wang J, Qin Y, Huang C, Archacki S, et al. (2016) Identification of three mutations in the MVK gene in six patients associated with disseminated superficial actinic porokeratosis. Clin Chim Acta 454: 124-9.
-
Panicker SP, Ganguly T, Consolo M, Price V, Mirmirani P, et al. (2012) Sterol intermediates of cholesterol biosynthesis inhibit hair growth and trigger an innate immune response in cicatricial alopecia. PLoS One 7(6): e38449.
-
Atzmony L, Lim YH, Hamilton C, Leventhal JS, Wagner A, et al. (2020) Topical cholesterol/lovastatin for the treatment of porokeratosis: a pathogenesis-directed therapy. J Am Acad Dermatol 82(1): 123-131.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling