Clinical Audit of Drug Prescription for Skin Disorders in Dermatology OPD at A Tertiary Care Centre
Introduction: Clinical audits are part of continuous quality improvement process that focus on specific issues or aspects of health care and clinical practice. There is growing concern about inappropriate drug utilization and prescribing habits of practitioners at all levels of health services. The cost of irrational use of medicines is enormous in terms of scarce resources and risk of adverse drug reactions. There is a paucity of data regarding prescription practices particularly in the dermatology department, so present audit was conducted. Materials and Methodology: This prospective prescription audit was carried out in Skin OPD of tertiary care centre amongst 100 prescriptions for duration of two months from November to December 2022. Demographic details and details of medications were recorded in a prestructured proforma and statistical analysis was done using descriptive studies. Results: In the current audit, 100 prescriptions were reviewed of which maximum prescriptions (33%) had a total of 3 drugs prescribed followed by 5 drugs in 22% of the prescriptions. Almost half, 45% prescriptions had 2 topical drugs and total 36% prescriptions had 2 systemic drugs given. In topical medications, 41% had moisturizers, 33% had antifungals. In systemic medications, 65% were anti-histaminic, 28% were antifungals. The frequency, strength, brand name and generic name were mentioned for topical and systemic drugs in 96% and 97% respectively. Total 14% of the prescriptions had FDCs. The average cost of prescription was Indian rupees 374.38. Discussion: Rational prescription writing is a talent that is learned via practise. Irrational prescriptions unnecessarily increase cost and duration of treatment. Drug interactions, medication resistance, and adverse drug reactions are also brought on by such activities which raises patient’s mortality, morbidity, and financial burden. Conclusion: This audit serves the purpose of evaluating prescriptions and further motivating such regular checks to improve patient outcomes.
Abbreviations
OPD: Out Patient Departments; FDC: Fixed Drug Combinations; WHO: World Health Organization.
Introduction
“Audit” derived from Latin takes on a meaning of “an official inspection of an organization’s accounts, typically by an independent body’. Clinical (or medical) audits are part of the continuous quality improvement process that focus on specific issues or aspects of health care and clinical practice [1].
The quality of the patient’s medical care is reflected in the prescription, which is a written medicolegal document created by an authorised person for the patient’s treatment. Improper prescription practices raise the patient’s mortality, morbidity, and financial burden.
Common skin conditions contribute significantly to the global illness burden. In terms of overall health burden, skin disorder is the 18th most common problem, and it was the fourth most common nonfatal problem in 2010 [2]. Total 2% of all consultations at Out Patient Departments (OPD) worldwide are for skin diseases [3]. Despite of conditions like pyoderma, acne, urticaria, dermatitis, scabies, fungal skin infections, and alopecia being the frequent skin problems in India, no comparable information about the prescription audit of the same is available.
There are many issues with the way drugs are prescribed in India, including inappropriate drug combinations, abuse of multivitamins, unnecessary use of antibiotics for fungus, and prescribing medications from the same class, resulting in antibiotic resistance. Irrational use of steroids is also a major healthcare issue [4]. Hence, the present study is done with the objective to see the prescription patterns in skin OPDs at tertiary care centre and to spot any deviations from current norms or existing recommendations.
Materials and Methodology
This prospective prescription audit was carried out in Skin OPD of tertiary care centre with the aim to study the pattern of drug prescription including the cost analysis for skin disorders. It was carried out for duration of two months from November to December 2022. A total 100 prescription issued to the patients was studied. The data collected included diagnosis, and total number of topical and systemic drugs. For each topical and systemic drug, the name of the molecule, brand name, frequency, dosing, strength, mentioning of fixed drug combinations (FDC) and whether instructions on use of drugs was given or not was noted. Descriptive studies were used for analysis.
The standards of clinical audit includes the following criteria As per Core components- WHO Policy Perspectives on Medicines, 2002:
- To ensure that patients receive medications appropriate to their clinical needs and in doses that meet their individual requirements at the lowest cost
- As per Code of Medical Ethics Regulations (MCI India) 2002:
- To ensure that drugs with their generic names are being prescribed and the dosage form and the strength of the drugs are being mentioned
- To see that Polypharmacy is being avoided
Results
In the current audit, 100 prescriptions were reviewed. Our hospital has software for prescription, thus demographic details of patients including full name, age and gender were mentioned in 100% of prescriptions. Information regarding name of prescribing doctor, name and contact details of hospital was mentioned in 100% prescriptions and all prescriptions had diagnosis of the patient.
Total 36% patients had infectious condition followed by 21% patients who had eczematous skin conditions. Table 1 Maximum prescription (33%) had a total of 3 drugs prescribed followed by 5 drugs in 22% of the prescriptions, 4 drugs in 20% and 2 drugs in 10% prescriptions. The maximum numbers of drugs prescribed were 9 which were noted in only 1% of the prescriptions.
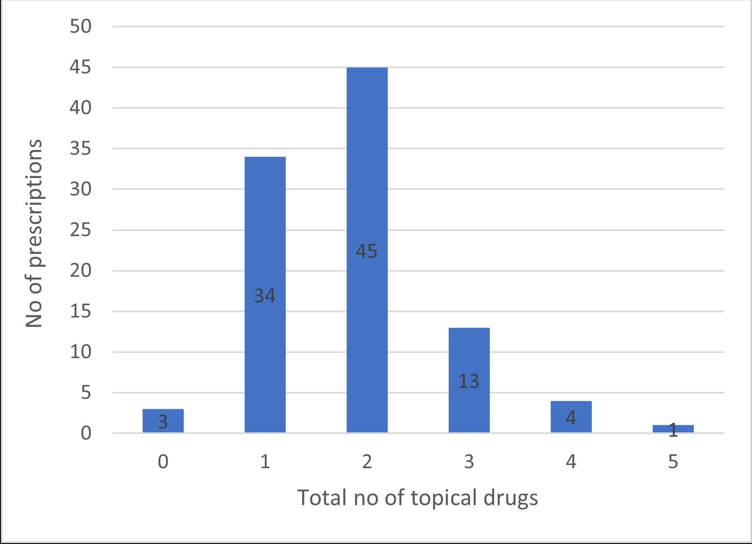
Out of the 100, almost half, 45% prescriptions had 2 topical drugs prescribed and 34% had 1 topical drug prescribed. Maximum number of topical drugs given was 5 which were observed in 1% prescription Figure 1.
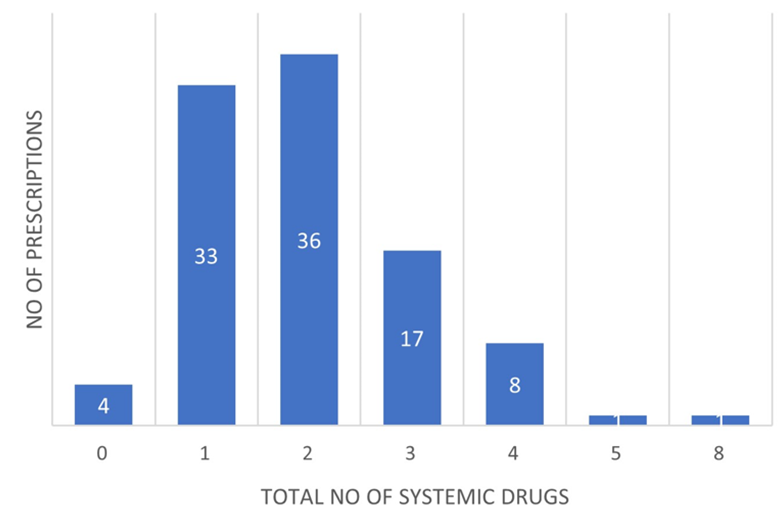
Total 36% prescriptions had 2 systemic drugs given which was closely followed by 33% prescriptions which had 1 systemic drug given. A maximum of 8 systemic drugs were given in 1% prescription Figure 2.
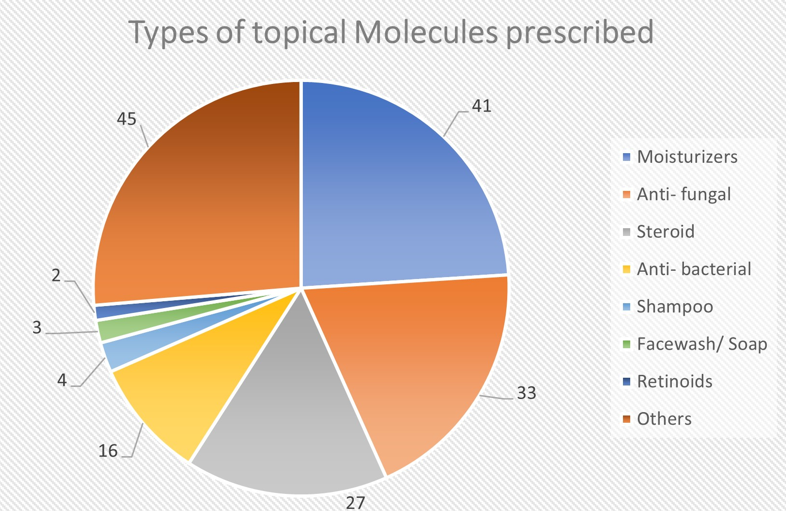
In topical medications, 41% had moisturizers, 33% had antifungals, 27% had steroid, 16% had anti-bacterial, 4% had shampoos, 3% had facewash/ soap and 2% had retinoids. Total 45% of the prescriptions had other molecules. (calcineurin inhibitors, keratolytic agents, vitamin D analogues, depigmentary agents) Figure 3 the frequency, strength, brand name and generic name were mentioned in 97% of all prescriptions, while 14% of the prescriptions had FDCs. Instructions about usage of the drugs were given in 98% of the prescriptions.
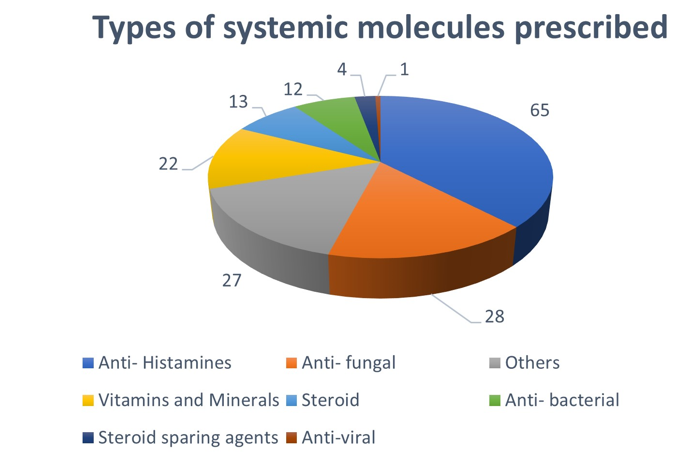
In systemic medications, 65% were anti-histaminic, 28% were antifungals, 22% were vitamins and minerals, 13% were steroid, 12% were anti-bacterial, 4% were steroid sparing agents, 1% were antiviral and 27% were others (Antacids, anti-inflammatory and scabicidal agents) Figure 4 the frequency, strength, brand name and generic name were mentioned in 96% of all prescriptions. Overall average drugs per prescription were 4.08 and the maximum number of average drugs per prescription was seen in drug reactions (Urticaria and MP rash) with 5.4 drugs per prescription. The average cost of prescription was 374.38 INR with the highest average cost per prescription for acne vulgaris (554.98 INR) (Table 1).
| Disorders | No. of Prescriptions | Average no. of drugs prescribed | Average cost of prescription (in INR) |
|---|---|---|---|
| Infections | |||
| Bacterial Infections (Leprosy) | 36 | 3.91 | 433.51 |
| Fungal | |||
| Infections | |||
| Viral Infections | |||
| Scabies | |||
| Drug Reactions | |||
| Urticaria | 5 | 5.4 | 340.24 |
| Maculopapular rash | |||
| Eczemas | |||
| Contact irritant | 21 | 3.2 | 272.69 |
| Allergic Dermatitis | |||
| Eczema | |||
| LSC | |||
| Seborrhoeic Dermatitis | |||
| Photodermatitis | |||
| Acne Vulgaris | 9 | 4.6 | 554.98 |
| Pigmentory | |||
| Vitiligo | 5 | 3.1 | 460.7 |
| Facial Pigmentation | |||
| PIH | |||
| Papulosquamous | |||
| Psoriasis | 6 | 5 | 294.44 |
| LP | |||
| Miscellaneous |
Table 1: Average number of drugs and cost per prescription in various conditions.
| Corn | 18 | 3.4 | 264.13 |
|---|---|---|---|
| Callosities | |||
| Xerosis | |||
| Ulcers | |||
| Pruritus | |||
| Telogen Effluvium | |||
| Pellagra | |||
| Keloid | |||
| Plantar Fissures | |||
| Intertrigo | |||
| Burns | |||
| Total | 100 | 4.08 | 374.38 |
Table 2: Average number of drugs and cost per prescription in various conditions.
Discussion
Clinical Audit is a quality improvement process that measures current patient care and outcomes against agreed standards of best practice. The World Health Organization (WHO) stated ‘rational use of drugs requires that patients receive medication appropriate to their clinical needs, in doses that meet their own individual requirement for an adequate period of time and at the lowest cost to them and their community’ [2].
Rational prescription writing is a talent that is learned via practise. Prescribing errors promote the irrational use of drugs and decrease the patient compliance. Irrational prescriptions unnecessarily increase the cost and duration of the treatment. Drug interactions, medication resistance, and adverse drug reactions are also brought on by such activities. In the end, it raises the patient’s mortality, morbidity, and financial burden [4].
There is a paucity of audits involving prescription practices in dermatology OPD setting. There is a greater need for proper guidelines especially in a speciality like dermatology where irrational prescriptions are due to a multitude of reasons. Patient specific reasons include unrealistic expectations demanding immediate cure which may force the prescriber to administer medications irrationally e.g., methotrexate in limited stages of psoriasis vulgaris. Misinformation about the drugs may sometimes lead to drug abuse such as chronic use of steroids as self- medication in many chronic illnesses. Physician specific reasons include lack of awareness of management guidelines. Prescribers must update themselves regularly by reading scientific publications, attending continuing medical educations, and conferences. Such activities would make the prescriber practice evidence-based dermatology rather than generalizing the limited experience. The dermatology field is being constantly plagued by many industries which resort to advertisements with misleading claims and unethical promotional activities. This would adversely affect the prescribing behaviour of the dermatologist and misleads the patients [5].
As per WHO, “polypharmacy” is the concurrent use of multiple medications. Although there is no standard definition, polypharmacy is often defined as the routine use of five or more medications including over-the-counter, prescription and/or traditional and complementary medicines used by a patient. Polypharmacy increases the chances of adverse drug reactions, drug interactions as well as the total cost per prescription [2]. On comparison with a study on drug prescribing and economic analysis for skin diseases in Dermatology OPD at a tertiary care hospital where average drugs prescribed were 2.39/prescription [6], our study had an average of 4 drugs prescribed in majority of the prescriptions. This was lower than study by Pathak AK, et al. [7] where average number of drugs per prescription was 5.13 [7].
It is much easier to prescribe a systemic agent than prescribe, educate, and motivate a patient to use topical and or other therapies. This may lead to prescribing systemic agents unreasonably, where the dermatoses can be controlled by only topical agents. Such practices should, however, be avoided. Topical corticosteroids are also used beyond prescribed time due to peer pressure, rapid feel-good effect, and ignorance about harmful effects lead to continuation of treatment beyond prescribed time [5].
In the study by Pathak AK, et al. [7] acne (17.95%) was most common dermatological disorder closely followed by eczema (16.62%), dermatophytosis (14.89%) and pigmentation disorders (3.47%). Our study had infections as the most common dermatological condition (36%) including bacterial, fungal, viral, and parasitic infections. This was closely followed by eczemas (21%) whereas pigmentary disorders formed about 5% of all the dermatological conditions.
In study by Bijoy KP, et al. [6] topical drugs were prescribed in majority of 62.7% prescriptions and our study had topical preparations in 97% of all prescriptions. Instructions about usage of the drugs were given in 98% of the prescriptions in present study. This was a positive outcome in terms of the fact that the practitioners should explain, educate, and motivate the patient to use topical formulations.
The Pathak AK, et al. [7] study did not classify the drugs according to their topical and systemic preparations and had anti-histamines as the most common prescribed preparation (24.13%) followed by anti-fungal (21.02%), antibiotics (15.91%) and steroid and combinations in 13.01% prescriptions. In our study, the most commonly prescribed class of drug in topical preparations were moisturizers (41%) followed by anti-fungal (33%). In systemic preparations, most common were anti-histamines (65%) followed by anti- fungal (28%). Study being conducted in months of winter can be the reason of maximum moisturizers being prescribed. One should also add moisturizing agent with steroids to avoid the side effects and better penetration.
In the study by Bijoy KP, et al. [6] frequency of administration was specified in majority of prescriptions (99%) for topical administered drugs but dose/strength was specified in 54 (13.85%) prescriptions only [6]. Sharma M, et al. [8] study which included other OPDs also of which (11.5%) prescriptions were from dermatology) showed that generic names were mentioned in 68.5% studies, strength in 27.1% and frequency in 50% of prescriptions [8]. This was in stark difference with our study where 97% of all prescriptions had frequency, strength, brand name and generic name mentioned. At our hospital we have a software which includes details of molecule in terms of frequency, strength brand and generic names of molecules, while writing a prescription. This type of software-based prescriptions helps minimizing the prescribing errors by the clinicians as writing the prescription on paper might lead to missing of few minor details. This kind of software should be installed in all possible hospitals and clinics.
Average cost of drugs per prescription was found to be 196.74 INR according to Bijoy KP, et al. [6] whereas in our study the average cost of prescription was 374.38 INR. This difference can be due to gap of ten years between the two studies, with increase in the cost of topical medications. The 2016 study by Pathak AK, et al. [7] had an average cost of prescription of 487.5 which was higher than in our study [7]. The costs of individual drugs might have increased leading to higher total cost per prescription in present study. This data requires a further in-depth analysis as to whether it is within rational drug practice guidelines or not. Adherence to Standard Treatment Guidelines during prescription writing and periodic monitoring of institutional drug policy will help to achieve the goal of improving health care delivery.
Conclusion
This drug utilization study provides an insight to the prescriber regarding various issues related to polypharmacy, cost analysis and prevalent disease pattern in the region. The prescriptions in dermatology clinics should be detailed, accurate and cost-friendly for the benefit of patients which can only be achieved by practicing the ways of rational prescribing and following the guidelines for the same. This audit serves the purpose of further motivating such regular checks to improve patient outcomes. Our future plans based on this audit is to.
- To educate the doctors regarding need for minimizing prescribing errors and importance of explanation of usage of drugs in the department.
- To do reaudit to evaluate improvement after creating awareness about the rational prescriptions which include adverse reaction alerts also.
Source(s) of Support: NIL
Conflicting Interest: NIL
Acknowledgement: NIL
References
-
(2002) National Institute for Clinical Excellence, CHI, Royal College of Nursing, University of Leicester. World Health Organization pp. 1-9.
-
(2004) The World Medicine Situation. Geneva: World Health Organization Press. World Health Organization.
-
Biswas NR, Jindal S, Siddiquei MM, Maini R (2001) Patterns of prescription and drug use in ophthalmology in a tertiary hospital in Delhi. British J Clin Pharmacol 51(3): 267-269.
-
(2003) Introduction to Drug Utilization Research. OSLO: World Health Organization.
-
Prakash B, Nadig P, Nayak A (2016) Rational prescription for a dermatologist. Indian J Dermatol 61(1): 32-38.
-
Bijoy KP, Vidyadhar RS, Palak P, Chintan SP, Atmaram PP (2012) Drug prescribing and economic analysis for skin diseases in dermatology OPD of an Indian tertiary care teaching hospital: a periodic audit. Indian Journal of Pharmacy Practice 5(1).
-
Pathak AK, Kumar S, Kumar M, Mohan L, Dikshit H (2016) Study of drug utilization pattern for skin diseases in dermatology OPD of an Indian tertiary care hospital-A prescription survey. Journal of clinical and diagnostic research 10(2): FC01-FCO5.
-
Sharma M, Payal N, Devi LS, Divya G, Manisha K, et al. (2021) Study on Prescription Audit from a Rural Tertiary Care Hospital in North India. J Pure Appl Microbiol 15(4): 1931-1939.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling