Pazopanib Induced Hand-Foot Skin Reaction
Hand-foot syndrome, also known as palmoplantar erythrodysesthesia, palmar-plantar erythema, toxic erythema of the palms and soles, or Burgdorf syndrome, is a common skin reaction to chemotherapeutic agents. In hand-foot syndrome, the palms, soles, dorsal surfaces of the hands and feet, occlusion, friction and pressure areas are affected. Symmetrical erythema and edema are seen on the palms and soles, accompanied by neuropathic pain. It may progress to desquamation, erosion and ulceration with blister formation. The palms are more affected than the soles. The most common causative agents are doxorubicin, liposomal doxorubicin, docetaxel, 5-fluorouracil (5-FU), cytarabine, capecitabine, but it can also be seen due to drugs such as paclitaxel, hydroxyurea, methotrexate, 6-mercaptopurine, cyclophosphamide, cisplatin, daunorubicin, etoposide, vinorelbine, irinotecan and epirubicin. In recent years, with the use of multi-kinase inhibitors in oncology, palmoplantar reactions, which show unique clinical features, have been reported. Pazopanib is a multi-targeted tyrosine kinase inhibitor. It may cause a hand-foot skin reaction with erythematous, hyperkeratotic nodules, bullae and pain and tingling sensation in the hands and feet. If such changes in the hands or feet are observed after starting Pazopanib treatment, the patient should be evaluated for side effects. Treatment should be adjusted if necessary and discontinuation of pazopanib should be considered in severe cases. We present a case of hand-foot skin reaction due to pazopanib.
Abbreviations
FDA: Food and Drug Administration; HFSR: Hand-Foot Skin Reaction.
Introduction
Pazopanib is an orally available, multi-targeted tyrosine kinase inhibitor that inhibits tumor angiogenesis and cell proliferation [1]. It was approved by the USA Food and Drug Administration (FDA) in 2009 for the treatment of advanced renal cell carcinoma and in 2012 for the treatment of advanced soft tissue sarcoma in patients who have received prior chemotherapy [2].
A 53-year-old woman presented with erythematous callus-like hyperkeratotic nodules and bullae on her hands and feet (Figure 1). The patient described tingling and burning sensation. These lesions had appeared 2 weeks ago. The patient had been taking pazopanib 800 mg/day for 2 months with a diagnosis of renal cell carcinoma.

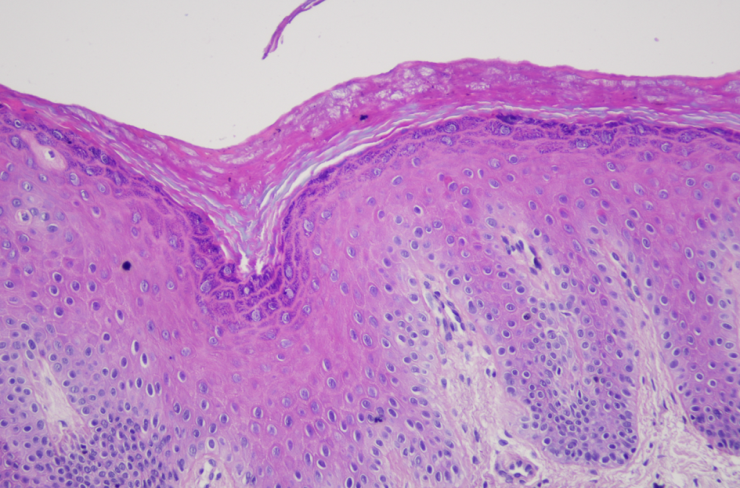
The biopsy showed hyperkeratosis, hypergranulosis, and perivascular mild lymphocytic infiltrate in the superficial dermis (Figure 2). As a result of these findings and symptoms, the patient was diagnosed with pazopanib-induced hand- foot skin reaction (HFSR).
The patient was treated with moisturizer and topical clobetasol propionate ointment and the lesions regressed within 2 months.
Discussion
Pazopanib is a multi-kinase inhibitor that selectively targets vascular endothelial growth factor 1, 2 and 3, platelet-derived growth factor receptor α and β and c-KIT mast/stem cell growth factor. The most common side effects are diarrhea, hypertension, hair colour changes, nausea, anorexia and vomiting [3].
The incidence of HFSR was 60.5%4 with regorafenib, 33.8%5 with sorafenib and 18.9%6 with sunitinib. The incidence of HFSR caused by pazopanib was lower than that of sorafenib and sunitinib, which share the same receptor targets [4, 5, 6, 7]. Docetaxel was the most incriminated drug in the genesis of HFS in a series (89%). In literature, the most common chemotherapy drugs associated with HFS are capecitabine, cytarabine, liposomal doxorubicin, FU and docetaxel [8, 9]. Other drugs may give a lower frequency of HFS, such as paclitaxel, methotrexate, hydroxyurea, and mitotane [9]. In areas prone to trauma or friction, such as high pressure points on the palms and soles of the feet, there is a higher propensity for vascular damage and reduced vascular repair, followed by keratinocyte apoptosis and the release of inflammatory chemokines [10].
In a prospective study, the frequency of HFSR with the combination of bevacizumab and sorafenib was higher than that with sorafenib as a single agent [11]. These results suggest that the VEGF signaling pathway is involved in the pathophysiology of HFSR.
Other hypotheses for the etiology of HFSR associated with tyrosine kinase inhibitors include accumulation of high local drug concentrations in eccrine sweat glands and keratinocyte damage secondary to sorafenib inhibition of c-kit or RAF kinase [10].
Conclusion
HFS due to cancer chemotherapy is quite challenging as it impacts not only the quality of life of patients but also the oncologists who manage such cases. The diagnosis of HFS may be easy in the case of typical lesions, but cases associating other localizations or other lesions should not rule out the diagnosis. The identification of risk factors is an important step for prevention. Many chemotherapeutic agents cause hand and foot syndrome. It should be kept in mind that pazopanib can cause HFSR and these patients should be monitored for skin changes on the hands and feet.
Ethics Statement
The authors declare that the necessary written informed consent has been obtained for the publication of this manuscript and accompanying images.
Conflict of Interest
The authors declare that the research was conducted without any commercial or financial relationship that could be interpreted as a potential conflict of interest.
References
-
Cella D, Beaumont JL (2016) Pazopanib in the treatment of advanced renal cell carcinoma. Ther Adv Urol 8(1): 61-69.
-
Nguyen DT, Shayahi S (2013) Pazopanib: approval for soft-tissue sarcoma. J Adv Pract Oncol 4(1): 53-57.
-
Udompanich S, Chanprapaph K, Rajatanavin N (2010) Phototoxic Reaction Induced by Pazopanib. Case Rep Dermatol 10(3): 251-256.
-
Belum VR, Wu S, Lacouture ME (2013) Risk of hand- foot skin reaction with the novel multikinase inhibitor regorafenib: a meta-analysis. Invest New Drugs 31(4): 1078-1086.
-
Chu D, Lacouture ME, Fillos T, Wu S (2008) Risk of hand- foot skin reaction with sorafenib: a systematic review and meta-analysis. Acta Oncol 47(2): 176-186.
-
Chu D, Lacouture ME, Weiner E, Wu S (2009) Risk of hand-foot skin reaction with the multitargeted kinase inhibitor sunitinib in patients with renal cell and non- renal cell carcinoma: a meta-analysis. Clin Genitourin Cancer 7(1): 11-19.
-
Balagula Y, Wu S, Su X, Feldman DR, Lacouture ME (2012) The risk of hand foot skin reaction to pazopanib, a novel multikinase inhibitor: a systematic review of literature and meta-analysis. Invest New Drugs 30(4): 1773-1781.
-
Fukuda A, Tahara K, Hane Y, Matsui T, Sasaoka S, et al. (2017) Comparison of the adverse event profiles of conventional and liposomal formulations of doxorubicin using the FDA adverse event reporting system. PLoS One 12: e0185654.
-
Zaiem A, Hammamia SB, Aouinti I, Charfi O, Ladhari W, et al. (2022) Hand-foot syndrome induced by chemotherapy drug: Case series study and literature review. Indian J Pharmacol 54(3): 208-215.
-
Yang CH, Chuang CK, Hsieh JJ, Chang JW (2010) Targeted therapy and hand-foot skin reaction in advanced renal cell carcinoma. Expert Opin Drug Saf 9(3): 459-470.
-
Azad NS, Ching JB, Dahut WL, Gutierrez M, Figg WD, et al. (2009) Hand-foot skin reaction increases with cumulative sorafenib dose and with combination anti- vascular endothelial growth factor therapy. Clin Cancer Res 15(4): 1411-1416.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling