Physical Healing in Dermatology: A Collaborative Approach
Globally, there is dramatic growth in the incidence of problematic scars. While dermatologists strive to decrease mortality from cancers, skin lesions, and inflammatory conditions, the resultant scars following from these treatments are rarely considered. It is common for scars from treatments to cause adhesions, leading to pain, neuropathy, or psychological issues. Even when the scar seems minimal, any injury to the highly neurological dermal layer can cause lifelong dysfunction. Refer-ring patients for scar therapy is not standard practice in dermatology; however, research shows that patients prioritize aesthetically pleasing, non-painful positive scars outcomes after dermatologic interventions. Patients who are at higher risk for pathological scar formation and pediatric clients should be prioritized for therapeutic intervention. Additionally, scar management is critical when lesions occur in the head, neck, and face due to the potential for neuropathy or poor cosmetic outcomes. Rehabilitation therapies can support recovery from the physical and psychological consequences of lacerations as well as minimally invasive or surgical procedures. Therapists specializing in scar management can offer unique treatments to help dermatology patients return to normal function after lifesaving treatments and routine intervention causes lesions. Promoting a comprehensive approach for dermatological care that includes referral to rehabilitation therapy will prevent the development of aberrant scars after procedures, thus reducing the financial and psychological burden and improving patient satisfaction.
Introduction
Patients in the United States (U.S.) spend nearly 2.5 billion dollars each year to manage postoperative scars, with an additional one million spent to address complications from adhesions [1]. These numbers are projected to soar to $60.5 billion by 2031 on a global scale [2]. Wound care is a comprehensive process for many patients, requiring multiple interventions to optimize healing. Research consistently promotes a multi-modal approach to scar management. Rehabilitation professionals can offer physical management to expedite recovery and function. Physical and occupational therapists specializing in scar management can become a link between dermatologic treatment and recovery through a comprehensive approach.
International research shows a surprisingly high incidence of scar tissue among their populations, with over half reporting having a scar; Russia leads with 61%, followed by the U.S. with 53% [3]. The most common areas where females had scars were the stomach (20.4%) and the face (15.9%). Among males, the most scarred skin was the face (18.7%) and the stomach (13.2%) [3]. The long-term cost of lacerations, lesions, and surgical scars includes physical and psychological impairments that can lead to social isolation or functional limitations [1, 3, 4, 5]. Lesions on the face or neck can cause pain in the dermatomes, along peripheral and cranial nerves, and limited motion through facial lines, causing jaw pain, facial asymmetry, headaches, and social anxiety [6]. Scar tissue is a significant challenge to cutaneous healing due to loss of skin function and appearance. The deficits may be heightened in the pediatric or adolescent population, which can experience long-lasting impacts of scars from physical growth [7].
Pathological scars can come in many forms, including atrophic, hypertrophic, and keloid scars [8, 9, 10, 11, 12, 13]. While scars are the natural conclusion of lesions or incisions from dermatologic procedures, any damage to the system of skin can diminish the system’s effectiveness in keeping the body in homeostasis [10, 14, 15]. Aberrant scars can cause contractures, pain, discoloration, and pruritic [9, 11, 16].
Environmental and genetic factors can impact wound healing, decreasing the ability of the wound borders to close and causing poor outcomes [12]. These can include limited skin elasticity [13], access to healthcare and education, and comorbidities such as infection and poor nutrition. Hypertrophic scars are most prevalent in those 10-30 years old due to increased elastin and skin tension, higher collagen production, and a greater risk of trauma [15]. Additionally, keloid scars are more common in those with more melanin, Fitzpatrick scale III-V (e.g., 10 to 16%) [12, 13, 15], and pregnant women due to hormonal increases [12]. The dermatologist aims to decrease morbidity while providing a satisfactory scar for the patient. Despite the advances in care, over half of patients are not satisfied with their scars, leading to social isolation and anxiety [17].
A 2024 survey of U.S. physical therapists shows that 81% (n = 572) believe therapists should be addressing postoperative scars in rehabilitation [18]. Therapists optimize movement and function while preventing procedure complications, such as stiffness, pain, edema, and pathological scar formation. A multi-modality approach to scar management for intervention is recommended, rather than one gold standard treatment [10]. The American Physical Therapy Association has specialists in wound care, while in Brazil, physical therapists act as dermatology specialists [19]. U.S. occupational therapists also have certified specialists in wound care [20].
Therapists use various techniques in the acute phase to reduce swelling and pain. These include focal vibration therapy (Figures 1 & 2), non-contact nitrogen-based cryotherapy, Kinesio taping applications, and gentle superficial skin scraping (instrument-assisted soft tissue massage) to accelerate healing [6, 18]. In the subacute phase, adhesion can decrease mobility, causing postural dysfunction and physical pain. Rehabilitation can specifically mobilize scars and the surrounding soft tissues to improve the range of motion and reduce contractures during all phases of wound healing (Figure 3). Allowing the tissues to glide freely reduces stress on the underlying neural structures, enhancing function and posture [6, 13]. In cases where the wound is associated with muscle or joint injury, therapists can further assist with proprioception, strengthening, balance, and mobility in the maturation phase of healing to facilitate quicker recovery.
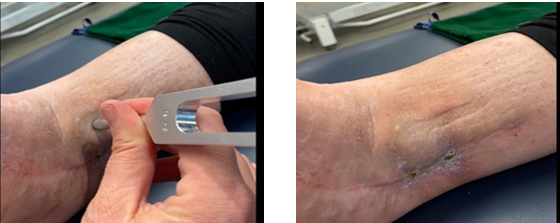
Figures 1 & 2: Note the reduction in edema where the tuning fork has been applied along the incision.

Dermatologists rarely consider scar therapy as a post- procedure follow-up, and little education is provided to patients regarding the management of their scars. Our experience indicates that scars play a much more significant role than previously acknowledged and can limit motion, cause pain, and create tension in other areas over time [6]. The scar’s depth is also essential since a scar can penetrate through multiple physiological layers depending on the amount of dysfunctional tissue involved. Scars that go down to the muscular level will impair the use of that muscle, which could, over time, impact joint mobility, muscle strength, and function. Patients could avoid future muscle or biomechanical imbalances and poor cosmetic outcomes by recommending early scar therapy.
Cancer
Some of the most influential scars are skin cancer excisions and benign tumors. One in five people have skin cancer in their lifetime [21]. Squamous cell carcinoma (CSCC) is the second most common cancer and is projected to double in incidence in European countries by 2030 [21]. The areas treated are typically visible, such as the nose, cheeks, ears, neck, shoulders, back, and arms. The injuries in these areas can significantly isolate patients and limit their ability to participate in society. Aside from psychological consequences, these lesions can impair critical cranial nerve function, including eye closure, mastication, and facial expression. Scars on the face or neck can also lead to headaches and jaw pain.
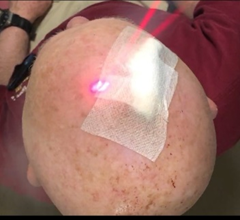
Rehabilitation can offer wound healing options to accelerate healing, including nitrogen-based cryotherapy post-operatively and photobiomodulation (Figures 4 & 5). Kinesio taping, vibration therapy, superficial skin scraping, and soft tissue massage can promote optimal wound closure across phases (Figures 6 & 7). Physical manipulation can aid tissue pliability and reduce edema when the wound is sufficiently closed.



Benign Tumors and Moles
Patients frequently have numerous moles removed from the back, chest, head, and arms. While appearing small, the scars created in these areas can produce tension in the sensory nervous system. Over time, these tensions can limit skin mobility, causing pain, and as the scar matures, it can influence movement patterns (Figures 8-10).
Therapists can thoroughly examine the number of scars and locations and map them over the sensory nerve and fascia pathways. A scar’s width, direction, and depth will influence the body in many ways. However, having treatments in place to assess the impact and avoid possible future ramifications is essential in holistic care.
Figures 8-10: Note the limited shoulder range of motion due to pain in the sensory nerves following the removal of multiple moles on the posterior trunk. Shoulder function was immediately improved by treating the scar with focal vibration therapy using a weighted ohm tuning fork and Kinesio tape applications.
Dermatologists rarely consider scar therapy at post- procedure follow-up, mainly where the lesions occur on the back or scalp. Our experience indicates that scars play a much more significant role than previously acknowledged and can limit motion, cause pain, and create tension in other areas over time.
The scar’s depth is also essential since a scar can penetrate through multiple physiological layers depending on the amount of dysfunctional tissue involved. Scars that go down to the muscular level will impair the use of that muscle, which could, over time, impact joint mobility and function. Recommending early scar therapy can help with future muscle or biomechanical imbalances.
Pediatric Considerations
Pediatric patients can present specific physical and psychological challenges that therapy should address. Dermatologists treat this population for vascular abnormalities, eczema, skin infections, lipomas, or inflammation [22]. These treatments can lead to skin adhesion and potentially impair motor development in infants and younger children [23]. Cutaneous sensory nerves and free nerve endings in the dermis transfer afferent information to the hypothalamus [24] deficits in this information cause motor skill impairments [25]. Physical growth in children can cause asymmetrical bone formation as skin tensions change with age [7] (Figures 11-14).
Lipomas or cyst removal can also cause deep fibrotic tissue, decreasing mobility in the soft tissues and surrounding joints (Figures 15-17). By mapping scars, therapy can be guided specifically for each patient, minimizing the impact on the skin, fascia, muscles, and joints. What is more important is that by focusing on the scars, especially in children, future physical and psychosocial outcomes can be diminished or eliminated [7, 18, 23]. Referral to therapists specializing in scar tissue management is essential for healing.







Conclusion
While dermatology addresses skin care, infection control, and the healing environment, therapists support wound healing by focusing on skin mobility, pain management, circulation, and function. When both fields work together, they can significantly improve patient outcomes of wound healing.
As patient care becomes more complex and health care costs rise, collaborative care to prevent and reduce the consequences of scar tissue is essential to promote best practices. Screening for high-risk patients and early detection of poor wound healing may minimize the impact. Understanding this, all patients would benefit from referral to scar specialists.
References
-
Hassanabad A, Zarzycki AN, Jeon K, Deniset JF, Fedak PM (2021) Postoperative Adhesions: A Comprehensive Review of Mechanisms. Biomedicines 9(8): 867.
-
2024 Global Scar Treatment Market $60.5 Billion by 2031. iHealthcareanalysrt.
-
Amici JM, Seite S, Floch S, Caroline F, Charles T (2021) Prevalence of scars: Results of the first international study. J Am Academy of Dermatol 85(3): AB120.
-
Li S, Ding H, Yang Y, Yu B, Chen M (2023) Global research status of pathological scar reported over the period 2001-2021: A 20-year bibliometric analysis. Int Wound J 20(5): 1725-1738.
-
Fernandes MG, Silva LP, Cerqueira MT, Murphy CM, Resi RL, et al. (2022) Mechanomodulatory biomaterials prospects in scar prevention and treatment. Acta Biomater 150: 22-33.
-
Taylor A, Harvey EG (2024) A framework for optimizing postoperative scars: A Therapist’s perspective. J Hand & Microsurgery pp: 100163.
-
Touze L, Teot L, Mustoe TA, Middelkoop E (2020) Scars in pediatric patients. Textbook on scar management: State of the art management and emerging technologies. Springer.
-
Eid MM, Abdelbasset WK (2022) Insight about different physical therapy techniques for management of hypertrophic scars. Inter J Biomed 12(2): 188-192.
-
Grigoryan KV, Kampp JT (2020) Summary and evidence grading of over-the-counter scar treatments. Inter J Dermatol 59(9): 1136-1143.
-
Lubczynska A, Garncarczyk A, Dziadecka D (2023) Effectiveness of various methods of manual scar therapy. Skin Research and Technology: International Society for Bioengineering and the Skin 29(3): 13272.
-
Nischwitz SP, Rauch K, Luze, H, Hofmann E, Draschl A, et al. (2020) Evidence-based therapy in hypertrophic scars: An update of a systematic review. Wound Repair and Regeneration 28(5): 656-665.
-
Ogawa R, Dohi T, Tosa M, Aoki M, Akaishi S (2021) The latest strategy for keloid and hypertrophic scar prevention and treatment: The Nippon Medical School (NMS) protocol. J Nippon Med School 88(1): 2-9.
-
Wong R, Geyer S, Weninger W, Guimberteau JC, Wong JK (2016) The dynamic anatomy and patterning of skin. Exp Dermatol 25(2): 92-98.
-
Reilly S, Crofton E, Brown J, Strong J, Ziviani J (2021) Use of tape for the management of hypertrophic scar development: A comprehensive review. Scars Burns & Healing 7: 1-17.
-
Rabello FB, Souza CD, Farina JA (2014) Update on hypertrophic scar treatment. Sao Paulo Clinics 69(8): 565-573.
-
Krakowski AC, Totri CR, Donelan MB, Shumaker PR (2016) Scar management in the pediatric and adolescent populations. Pediatrics 137(2): 20142065.
-
Kinani M, Duteille F (2020) Scar Epidemiology and Consequences. In: Teot L, et al. (Eds.), Textbook on Scar Management: State of the Art Management and Emerging Technologies. Cham (CH): Springer. 6th (Chapter).
-
Harvey EG, Ewen H, Moore E, Ru E (2024) The knowledge, attitude, and practices of physical therapists regarding postoperative scar tissue in the United States. The University of Indianapolis Dissertation.
-
Claudino R, Pietro N, Silva T (2019) Evidence-Based Practice: a survey of Brazilian physical therapists from the dermatology subdiscipline. Braz J Phys Ther 23(5): 395-401.
-
Amini D (2018) Role of Occupational Therapy in Wound Management. The Am J Occupational Therapy 72(2): 7212410057p1-7212410057p9.
-
Hasan N, Nadaf A, Imran M, Almalki WH, Almujri SS, et al. (2023) Skin cancer: understanding the journey of transformation from conventional to advanced treatment approaches. Mol Cancer 22(1): 168.
-
Kaushik A, Natsis N, Gordon SC, Seiverling EV (2020) A practical review of dermoscopy for pediatric dermatology part I: Melanocytic growths. Pediatr Dermatol 37(5): 789-797.
-
Harvey EG (2023) Kinesio taping to address post- sternotomy scars in pediatric patients: A case report. Scars, Burns & Healing 8: 1-7.
-
Lechuz J, Espiau MR, Lechuz E (2017) Treatment of the scar after arthroscopic surgery on a knee. J of Bodywork and Movement Therapies 21(2): 328-333.
-
Matur Z, Oge AE (2017) Sensorimotor integration during motor learning: Transcranial magnetic stimulation studies. Noro Psikiyatri Arsivi 54(4): 358-363.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling