Pattern of Skin Diseases in Ebonyi State University Teaching Hospital
We report the pattern of skin diseases seen in the dermatology clinic of the Ebonyi State University Teaching Hospital, Abakaliki from November 1998 to December 2012. Four thousand and six (4006) new patients were seen during the study period. There were more females than males with a female/male ratio of 1.42:1. Infectious diseases accounted for 30.8% of all the skin disorders. This is consistent with early studies carried out in Nigeria and some other parts of Africa. Other top ranking skin diseases observed in decreasing order of frequencies include eczematous disorders (27.7%), urticaria/pruritus (7.7%), pilosebaceous disorders (5.4%), pigmentary disorders (5.1%) and papulosquamous disorders (5.0%). HIV related skin diseases accounted for 2.7% of disorders seen. The current pattern of diseases observed seemed to follow similar pattern observed in earlier studies and in contrast to recent studies. Infectious disorders ranked highest with eczematous disorders closely following
Introduction
Skin diseases are important and are a common cause of ill health in Africa [1]. In Africa, poor nutrition, inadequate portable water supply and poor environmental sanitation all add to the burden of disease [2]. The distribution of skin diseases varies from one country to another and between regions in the same country. There are various reports on the pattern of skin diseases in different areas of Nigeria with some Teaching Hospital observed differences [3, 4, 5, 6, 7]. With this study, we hope to identify the common skin disorders in our environment as this will assist in proper planning and management of these disorders.
Materials and Methods
This is a retrospective review of skin diseases in new patients presenting to the skin clinic of the Ebonyi State University Teaching Hospital in Abakaliki, Ebonyi state in South Eastern Nigeria between November 1998 and December 2012. Data was compared with findings from other geo-political zones. Ebonyi state was created in 1996 from old Abakaliki division of Enugu state and old Afikpo division of Abia state. It has a land mass of 5935 km2 sharing boundaries with Enugu on the West, Cross River in the East, Abia in the South-East and Benue in the North. The state has 13 local government areas (LGAs). It has an estimated population of 4.3 million. About 75% of the population are rural dwellers with farming as the predominant occupation [8]. The hospital, being a tertiary hospital receives referral from all hospitals in the state and neighbouring states. The patients age, gender and skin disease diagnosis were extracted from the medical records. The diagnosis in most instances was clinical and supplemented in few cases by histology. Other tests done were skin scraping for mycology tests, skin snip for microfilaria and slit skin smear for M.leprae. The Statistical Package for Social Sciences (SPSS) version 16 was used for data entry and analysis.
Ethical Considerations
This study was carried out in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Results
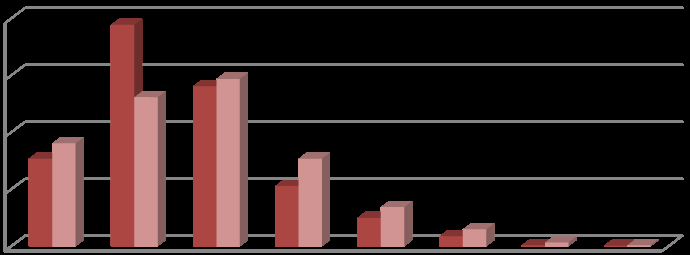
Four thousand and six (4006) new patients attended the skin clinic within the review period. Pure dermatological consultations accounted for 76.9% (3080) of the patients, while HIV and HIV related skin diseases accounted for 23.1% (926) of the patients. About 95(3.1%) had more than one dermatological diagnosis. There were more females 2353(58.7%) than males 1653(41.3%), with a female/male ratio of 1.42:1. Nine hundred and fifty nine (23.9%) were less than 16 years while 3047(76.1%) were more than 16 years. The ages of the patients ranged from 1 week to 90 years. The mean ± S.D of age was 27.65±13.96 years. Figure 1 below shows the age and sex distribution of all the new patients seen over this time frame, 1998- 2012.
| Skin diseases | Frequency | % | ||||||
|---|---|---|---|---|---|---|---|---|
| Infections/infestations | 980 | 30.8 | ||||||
| Dermatitis | 883 | 27.7 | ||||||
| Urticaria/pruritus | 245 | 7.7 | ||||||
| Pilosebaceous disorders | 173 | 5.4 | ||||||
| Pigmentary disorders | 162 | 5.1 | ||||||
| Papulosquamous disorders | 160 | 5.0 | ||||||
| Adverse drug reaction | 99 | 3.1 | ||||||
| Disorders of keratinization | 99 | 3.1 | ||||||
| HIV related skin diseases | 85 | 2.7 | ||||||
| Fibrous tumours of the skin | 76 | 2.4 | ||||||
| Neurocutaneous disorders | 32 | 1.0 | ||||||
| Hair disorders | 31 | 1.0 | ||||||
| Connective tissue disease | 19 | 0.6 | ||||||
| Benign neoplastic disorders | 17 | 0.5 | ||||||
| Bullous disorders | 17 | 0.5 | ||||||
| Cutaneous malignancies | 13 | 0.4 |
Table 1: Main Disease Groups.
| Lymphoedema | 12 | 0.4 |
|---|---|---|
| Psychiatric disorders | 6 | 0.2 |
| Miscellaneous | 77 | 2.4 |
| Total | 3186 | 100 |
Table 2: Main Disease Groups.
| Infections/ | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Frequency | %Group | %Total | |||||||||
| infestations | |||||||||||
| Fungal | 460 | 46.9 | 14.4 | ||||||||
| Bacterial | 288 | 29.4 | 9.0 | ||||||||
| Viral | 134 | 13.7 | 4.2 | ||||||||
| Parasitic | 98 | 10 | 3.1 | ||||||||
| Total | 980 | 100 | 30.8 |
Table 3: Infective Disorders.
| Frequency | %Group | %Total | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Dermatitis | |||||||||||
| Nonspecific-chronic dermatitis | 419 | 47.4 | 13.1 | ||||||||
| Atopic dermatitis | 127 | 14.4 | 4.0 | ||||||||
| Seborrheic dermatitis | 111 | 12.6 | 3.5 | ||||||||
| Allergic contact dermatitis | 80 | 9.1 | 2.5 | ||||||||
| Lichen simplex chronicus/prurigonodularis | 49 | 5.5 | 1.5 | ||||||||
| Pompholyx | 29 | 3.2 | 0.9 | ||||||||
| Nummular dermatitis | 28 | 3.2 | 0.9 | ||||||||
| Exfoliative dermatitis | 23 | 2.6 | 0.7 | ||||||||
| Stasis dermatitis | 5 | 0.6 | 0.2 | ||||||||
| Breast eczema | 5 | 0.6 | 0.2 | ||||||||
| Photodermatitis | 4 | 0.4 | 0.1 | ||||||||
| Irritant contact dermatitis | 3 | 0.3 | 0.09 | ||||||||
| Group total | 883 | 100 | 27.7 | ||||||||
| Hidradenitis suppurativa | 2 | 1.15 | 0.05 | ||||||||
| Steatocystoma multiplex | 2 | 1.15 | 0.05 | ||||||||
| Group total | 173 | 100 | 5.4 | ||||||||
| Pigmentary disorders | |||||||||||
| Vitiligo | 99 | 61.1 | 3.1 | ||||||||
| Albinism | 15 | 9.3 | 0.5 | ||||||||
| Postinflammatory hyperpigmentation | 15 | 9.3 | 0.5 | ||||||||
| Hypermelanosis | 14 | 8.6 | 0.4 | ||||||||
| Postinflammatory hypopigmentation | 9 | 5.6 | 0.3 | ||||||||
| Pellagra | 6 | 3.7 | 0.2 | ||||||||
| Idiopathic guttatehypomelanosis | 2 | 1.2 | 0.06 | ||||||||
| Chloasma | 1 | 0.6 | 0.03 | ||||||||
| Freckles | 1 | 0.6 | 0.03 | ||||||||
| Group total | 162 | 100 | 5.10 | ||||||||
| Papulosquamous disorders | |||||||||||
| Pityriasis rosea | 75 | 46.9 | 2.4 | ||||||||
| Lichen planus | 50 | 31.3 | 1.6 | ||||||||
| Psoriasis | 19 | 11.9 | 0.6 | ||||||||
| Lichen nitidus | 5 | 3.1 | 0.12 | ||||||||
| Lichen striatus | 5 | 3.1 | 0.12 | ||||||||
| PLEVC | 4 | 2.5 | 0.1 | ||||||||
| Pityriasis rubra pilaris | 1 | 0.6 | 0.03 |
Table 4: Is the breakdown of the specific conditions.
| PLEVA | 1 | 0.6 | 0.03 |
|---|---|---|---|
| Group total | 160 | 100 | 5.0 |
| Viral Infections | |||
| Viral warts | 48 | 35.8 | 1.5 |
| Herpes simplex | 26 | 19.4 | 0.8 |
| Herpes zoster | 25 | 18.7 | 0.8 |
| Molluscum contagiosum | 16 | 11.9 | 0.5 |
| Varicella | 11 | 8.2 | 0.4 |
| Viral exanthem | 7 | 5.2 | 0.2 |
| Miscellaneous | 1 | 0.8 | 0.03 |
| Group total | 134 | 100 | 4.2 |
| Adverse drug eruption | |||
| FDE | 74 | 74.7 | 2.3 |
| Nonspecific eruption | 15 | 15.3 | 0.5 |
| Acneiform eruption | 3 | 3.0 | 0.09 |
| SJS | 2 | 2.0 | 0.05 |
| Hypopigmentation | 2 | 2.0 | 0.05 |
| Striae | 1 | 1.0 | 0.03 |
| Hyperpigmentation | 1 | 1.0 | 0.03 |
| Mazzoti reaction | 1 | 1.0 | 0.03 |
| Group total | 99 | 100 | 3.1 |
| Disorders of keratinization | |||
| Follicular hyperkeratosis | 52 | 52.5 | 1.6 |
| Phrynoderma | 31 | 31.3 | 1.0 |
| Callosities/corns | 8 | 8.1 | 0.3 |
| Ichthyosis | 7 | 7.1 | 0.2 |
| Tylosis | 1 | 1.0 | 0.03 |
| Group total | 99 | 100 | 3.1 |
| Parasitic infestations | |||
| Onchodermatitis | 49 | 50 | 1.5 |
| Scabies | 39 | 39.9 | 1.2 |
| Cutaneous leishmaniasis | 2 | 2.0 | 0.05 |
| Tumbu fly | 1 | 1.0 | 0.03 |
| Cutaneous larva migrans | 1 | 1.0 | 0.03 |
| Others | 6 | 6.1 | 0.2 |
| Group total | 98 | 100 | 3.1 |
| Nail disorders | |||
| Acute paronychia | 1 | 1.1 | 0.03 |
| Chronic/candida paronychia | 26 | 29.6 | 0.82 |
| Tinea unguium/Onychomycosis | 61 | 69.3 | 1.9 |
| Group total | 88 | 100 | 2.8 |
| HIV related skin diseases | |||
| Papular pruritic eruption | 18 | 21.2 | 0.6 |
| Herpes zoster | 16 | 18.8 | 0.5 |
| Kaposi sarcoma | 11 | 12.9 | 0.4 |
| Bacterial infections | 10 | 11.8 | 0.3 |
| Dermatophytes | 7 | 8.2 | 0.2 |
| Seborrheic dermatitis | 7 | 8.2 | 0.2 |
| Chronic paronychia | 4 | 4.7 | 0.12 |
| Herpes simplex | 3 | 3.5 | 0.09 |
| Viral warts | 3 | 3.5 | 0.09 |
| Pruritus | 2 | 2.4 | 0.05 |
| Scabies | 2 | 2.4 | 0.05 |
| Varicella | 1 | 1.2 | 0.03 |
| Drug eruption | 1 | 1.2 | 0.03 |
| Group total | 85 | 100 | 2.7 |
| Fibrous tumours of skin | |||
| Keloids | 43 | 56.6 | 1.4 |
| Naevus | 16 | 21.1 | 0.5 |
| Actinic keratosis | 6 | 7.9 | 0.2 |
| Dermoid cyst | 4 | 5.3 | 0.12 |
| Pyogenic granuloma | 3 | 3.9 | 0.09 |
| Hypertrophic scars | 2 | 2.6 | 0.05 |
| Sebaceous cyst | 2 | 2.6 | 0.05 |
| Group total | 76 | 100 | 2.4 |
| Neurocutaneous disorders | |||
| Neurofibromatosis | 32 | 100 | 1.0 |
| Group total | 32 | 100 | 1.0 |
| Hair disorders | |||
| Alopecia areata | 20 | 64.5 | 0.63 |
| Acne keloidalisnuchae | 4 | 12.9 | 0.12 |
| Alopecia | 4 | 12.9 | 0.12 |
| Scarring alopecia | 3 | 9.7 | 0.09 |
| Group total | 31 | 100 | 1.0 |
| Connective tissue diseases | |||
| DLE | 12 | 63.2 | 0.4 |
| Scleroderma | 4 | 21.0 | 0.12 |
| Mixed connective tissue disease | 3 | 15.8 | 0.09 |
| Group total | 19 | 100 | 0.6 |
| Benign neoplastic disorders | |||
| Dermatosispapulosanigra | 15 | 88.2 | 0.47 |
| Syringoma | 2 | 11.8 | 0.05 |
| Group total | 17 | 100 | 0.5 |
| Bullous disorders | |||
| Erythema multiforme | 9 | 52.9 | 0.3 |
| Dermatitis herpetiformis | 4 | 23.5 | 0.12 |
| Pemphigus vulgaris | 3 | 17.6 | 0.09 |
| Pemphigus foliaceus | 1 | 5.9 | 0.03 |
| Group total | 17 | 100 | 0.5 |
| Cutaneous Malignancies | |||
| Endemic Kaposi sarcoma | 4 | 30.8 | 0.12 |
| SCC | 4 | 30.8 | 0.12 |
| BCC | 2 | 15.4 | 0.05 |
| Malignant melanoma | 2 | 15.4 | 0.05 |
| Basal cell epithelioma | 1 | 7.7 | 0.03 |
| Group total | 13 | 100 | 0.4 |
| Lymphoedema | |||
| Lymphoedema | 12 | 100 | 0.4 |
| Group total | 12 | 100 | 0.4 |
| Psychiatric disorders | |||
| Trichotillomania | 2 | 33.3 | 0.05 |
| Formication | 2 | 33.3 | 0.05 |
| Dermatitis artefacta | 1 | 16.7 | 0.03 |
| Venerophobia | 1 | 16.7 | 0.03 |
| Group total | 6 | 100 | 0.2 |
| Miscellaneous | 77 | 100 | 2.4 |
Table 5: Is the breakdown of the specific conditions.
| Miscellaneous skin disorders: | Frequency | ||||
|---|---|---|---|---|---|
| Xanthelasma palpebrarum | 8 | ||||
| Haemangioma | 8 | ||||
| Miliaria | 6 | ||||
| Granuloma telangiectasia | 6 | ||||
| Post bleaching syndrome | 6 | ||||
| Striae distensae | 5 | ||||
| Granuloma annulare | 5 | ||||
| Panniculitis | 3 | ||||
| Erythema nodosum | 3 | ||||
| Xanthoma | 2 | ||||
| Hyperhidrosis | 2 | ||||
| Calcinosis cutis | 2 | ||||
| Dercums disease | 2 | ||||
| Cheilitis | 2 | ||||
| Postherpetic neuralgia | 2 | ||||
| Xeroderma | 2 | ||||
| Abrasions | 1 | ||||
| Atrophoderma | 1 | ||||
| Elastosis | 1 | ||||
| Morphoea | 1 | ||||
| Leg ulcer | 1 | ||||
| Lipodystrophy | 1 | ||||
| Lipomata | 1 | ||||
| Pagets disease | 1 | ||||
| Pearly penile papules | 1 | ||||
| Port wine stain | 1 | ||||
| Purpura | 1 | ||||
| Reiters syndrome | 1 | ||||
| Wound dehiscence | 1 | ||||
| Total | 77 |
Table 6: Miscellaneous Skin Disorders.
Discussion
We discovered that when considered together, infections and infestations were the commonest dermatoses (30.8%) in this study. The study in Ghana by Doe et al in 2000 also noted a high prevalence of infections (46.3%) [9] similar to findings by Husain, Atraide, Fekete and Onayemi [5, 6, 10, 11]. However recent studies by Ogunbiyi, Ukonu et al recorded a higher prevalence of eczematous disorders [3, 7]. The higher prevalence of infectious disorders may be due to poor environmental hygiene occurring among predominantly rural dwellers with low socio-economic status and low level of education as seen among our patients. Fungal skin disorders were the commonest form of infective skin disorder (46.9% of all infective causes and 14.4% of the total). Eczematous disorders ranked second in this study, with non-specific chronic dermatitis being the commonest in this group (47.1%) followed closely by atopic dermatitis (14.4%) and seborrheic dermatitis (12.6%). Chronic dermatitis seen in our patients may have arisen from the effect of treatment which modified the appearance of these dermatoses. In a prospective study by Ukonu, et al., in Benin, they recorded a prevalence of 15.3% for non–specific chronic dermatitis while contact dermatitis ranked highest for eczematous disorders (35.4%) [7]. The study in Port Harcourt recorded atopic dermatitis as the commonest form of eczematous disorders [6]. There was also an increase in the prevalence of contact dermatitis in Ibadan and Kaduna [3, 5]. Acne vulgaris was the commonest pilosebaceous disorder (94.2% of pilosebaceous disorders); similar to findings from other studies [4, 5, 6, 7]. Most of these patients were secondary and university undergraduates. Papular urticaria was the commonest urticarial lesion noted. This occurred in children and teenagers. It related to hypersensitivity to bites from insects. Patients presented with itchy papules, wheals with excoriations and sometimes with secondary bacterial colonization. A number presented with post- inflammatory hyperpigmented macules and papules. Vitiligo, albinism and post-inflammatory hypopigmentation were the commonest pigmentary disorders noted in this study. This is similar to previous studies conducted in Africa [4, 7, 12]. Some of the patients with vitiligo were erroneously labeled as Hansen’s disease by primary care physicians and referred to the leprosy treatment centre in the state before being properly evaluated and referred to the skin clinic. Papulosquamous disorders were also on the increase. The highest numbers were pityriasis rosea, lichen planus and psoriasis. These disorders reduce the overall quality of life due to the discomfort and unsightly cosmetic appearance they give to the patient. Pruritic papular eruption (PPE) was the commonest dermatoses seen in those with HIV/AIDS (occurring in 21.2% of all patients with HIV), followed by herpes zoster and Kaposi sarcoma. Similar studies in Port Harcourt and Kaduna, noted a higher prevalence of PPE [5, 6]. Seborrheic dermatitis was the most prevalent in the study by Nnoruka [4]. The patients with PPE who had itchy papules on the extremities resorted to the use of hydroquinone or steroid based creams for treatment with subsequent development of post-inflammatory hyperpigmented macules and papules. Cutaneous malignancies i.e. basal cell carcinoma, squamous cell carcinoma, malignant melanoma and basal cell epithelioma seen here occurred in those with albinism. The diagnosis was confirmed with the aid of histopathology. These patients were managed in consonance with the plastic surgeons. This finding highlights the need for patients with albinism to be properly educated on the dangers of skin exposure to the damaging effects of ultra-violet rays [13].
Conclusion
This review shows that infective skin disorders ranked highest in prevalence in contrast to more recent findings in other geopolitical zones, where eczematous disorders were the most prevalent. This information is important, as it would assist in proper health planning for management of dermatological conditions.
References
-
King S (2004) Growing awareness of skin diseases starts a flurry of initiatives. Bulletin of World Health Organisation.
-
Rook A, Savin JA, Wilkinson DS (1987) The prevalence, incidence and ecology of diseases of skin, In Rook A, Wilkinson DS, Ebling FJ, Champion RH, Burton JL, editors, Text book of Dermatology. Oxford University Press, Mumbai, 39-53.
-
Ogunbiyi AO, Daramola OOM, Alese OO (2004) Prevalence of skin diseases in Ibadan, Nigeria. Int J Dermatol 43(1): 31-36_._
-
Nnoruka EN (2004) Skin diseases in South-East Nigeria. A current perspective. Int J Dermatol 44(1): 29-33.
-
Husain Y (2007) Change in pattern of skin disease in Kaduna, North- central Nigeria. Int J Dermatol 46(9): 936-946.
-
Atraide AA, Akpa MR, George IO. Pattern of skin disorders in a Nigerian tertiary hospital. J Public Health and Epid 3(4): 177-181.
-
Ukonu BA, Eze EU (2012) Pattern of skin diseases at University of Benin Teaching Hospital, Benin-city, Edo state, South-South, Nigeria: A 12 month prospective study. Global J Health Sci 4(3): 148-157.
-
Official gazette (FGP.71/52007/2500 (0224). Legal notice on publication of the details of the breakdown of the National and State provisional totals. 2006 census. Federal republic of Nigeria. 2006 population census Abuja 2007: 1-10
-
Doe PT, Asiedu A, Acheampong JW, Rowland Payne CM (2001) Skin diseases in Ghana and the UK. Int J Dermatol 40(5): 323-326.
-
Fekete E (1978) The pattern of diseases of the skin in the Nigerian Guinea Savannah. Int J Dermatol 17(4): 331-338.
-
Onayemi O, Isezuo SA, Njoku CH (2005) Prevalence of different skin conditions in an outpatients setting in North-Western Nigeria. Int J Dermatol 44(1): 7- 11.
-
Onunu AN, Kubeyinje PE (2003) Vitiligo in the Nigerian African: A study of 351 patients in Benin City Nigeria. Int J Dermatol 42(10): 800-802.
-
Okoro AN (2006) Albinism in Nigeria: A clinical and social study. Br J Dermatol 92(5): 485-492_._
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria