Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
Background: Clinical-epidemiological data on SARS-CoV-2 reinfections in endemic period are scarce. Objective: To know the clinical-epidemiological characteristics of current reinfection cases of covid-19. Methodology: An observational, longitudinal and prospective case series study of adult patients with covid-19 reinfections in general medicine from October 1, 2023 to September 30, 2924. Results: 15 cases of covid-19 reinfections were included during the study period. Of these cases, there were 2 that had presented 2 previous reinfections and one case that had presented 3 previous reinfections. 27% of cases had 5 doses of vaccine and 67% had 3 doses. Of the 15 cases of reinfection, 27% were >65 years old, 67% women, and 27% socio-health workers. None presented moderate-severe severity; 80% had chronic diseases (23% Musculo-skeletal, 18% Nervous and Senses, 13% Endocrine). 54% of the symptoms were General, 24% were Respiratory, 15% were Otorhinolaryngology, 5% Neurological, and 2% Digestive. Conclusion: In the context of general medicine in Toledo (Spain), from 2020 to 2024, a period considered endemic, with high levels of vaccination, covid-19 reinfections had mild symptoms. They were more frequent in women, and had chronic diseases, but they do not occur in people with the classic comorbidities of the Circulatory system or Respiratory. There is a considerable frequency of reinfections in socio-health workers, possibly because they are more exposed and undergo diagnostic testing more frequently. Staying up to date with covid-19 vaccinations is still advisable.
Introduction
Five years after the start of the Coronavirus disease 2019 (covid-19) pandemic, for most people, a second (third or fourth) infection with severe acute respiratory syndrome coronavirus (SARS-CoV-2) is almost inevitable. The longer the virus remains in circulation, the more frequent recurrent infections will be. As the virus is currently endemic, the chances of being exposed and re-infected are also higher, as are reinfections after vaccination. At the same time, the level of misinformation about reinfections is at its highest, and the causes and risk factors for covid-19 reinfection are not fully understood [1, 2, 3, 4, 5, 6, 7, 8, 9].
Reinfections were rare until the end of 2021, but became common with the arrival of Omicron [6]. A meta-analysis of global SARS-CoV-2 reinfection rate up to March 16, 2023, showed there was a significant increase in the number of SARS-CoV-2 reinfection reports in various countries since the Omicron variant, e informó de una tasa de reinfección por SARS-CoV-2 agrupada de 0.94% [10].
During the covid-19 pandemic period, very detailed epidemiological surveillance measures were taken. Currently in the endemic phase, many of the community surveillance studies tracking infection levels have ended, as it happens in Spain [11, 12]. Thus, covid-19 case counts are no longer published, and it is not clear how many people are infected, nor can the evolution of the number of infections be known at community level.Therefore, in this scenario, people may experience reinfections of covid-19 over time. It is estimated that at least 30% of the population could be re-infected in successive waves. Continuous waves of infection carry the risk of new emerging variants that can compete with the current ones and be more severe [11]. Furthermore, there is increasing scientific evidence that shows that the protection generated by vaccination decreases over time, although it is re-established with the inoculation of booster doses. Additionally, we must take into account the decline in immunity as a result of the new variants, and that despite vaccines, boosters and natural immunity, the variants appear to be capable of evading any protection that may have been obtained against SARS -CoV-2 [13, 14, 15, 16, 17, 18].
Thus, in this context, knowing the clinical- epidemiological evolution of covid-19 reinfection is crucial to evaluate its trajectory [19].
In summary, there is a lack of community data on the evolution of covid-19 reinfections during endemic period. In this context, we present an observational, longitudinal and prospective study of covid-19 reinfection cases, from October 2023 to October 2024 with the aim of knowing their clinical-epidemiological characteristics.
Material and Methods
Design and Emplacement
Observational, longitudinal and prospective case series study of adult patients with covid-19 reinfections, from October 1, 2023 to October 1, 2024, in a general medicine office in Toledo, Spain. Toledo is a Spanish city, capital of the province of the same name, in the community of Castilla- La Mancha. It has a population of 86,526 inhabitants, and is located 71 km from the country’s capital, Madrid [20]. Toledo has a cold semi-arid climate. Precipitation is scarce, concentrated mainly in spring and late autumn, with a marked summer drought and significant daily temperature oscillation.
The general medicine practice subject to the study has a list of 2,000 patients > 14 years of age (in Spain, general practitioner (GP) care for people > 14 years of age, except for exceptions). The GPs in Spain work within the National Health System, which is public in nature, and are the gateway for all patients to the system, and each person is assigned a GP.
“Cases”of reinfected Covid-19 were collected, not people with reinfection, so if a person had more than one reinfection during the study period, all were included (even if the patient was a repeat patient).
Outcome of Interest
To know and describe a set of selected clinical- epidemiological characteristics of cases of covid-19 reinfection in the endemic period for one year (from October 1, 2023 to October 1, 2024) at primary health care level.
Definition of Reinfection
SARS-CoV-2 reinfection was defined as a documented infection occurring at least 90 days after a previous infection [21, 22, 23].
Diagnosis of Covid-19
The diagnosis was performed with reverse transcriptase polymerase chain reaction oropharyngeal swab tests or antigen testing performed in health services or at home [24].
Collected Variables
The following variables were collected: -Age and sex. -Chronic diseases (defined as “any alteration or deviation from normal that has one or more of the following characteristics: is permanent, leaves residual impairment, is caused by a non- reversible pathological alteration, requires special training of the patient for rehabilitation, and / or can be expected to require a long period of control, observation or treatment” and symptoms covid-19 infection, both classified according to the International Statistical Classification of Diseases and Health-Related Problems, CD-10 Version: 2019 [25, 26]. -Social-occupancy class (according to the Registrar General’s classification of occupations and social status code) [27, 28]. -If they were Health Care Workers. -Problems in the family context based on the genogram and in the experience of the GP for their continuity of care and knowledge of the family (genogram is a schematic model of the structure and processes of a family, which included the family structure, life cycle and family relational patterns. It was understood that “complex” genograms present families with psychosocial problems) [29, 30, 31]. -Ethnic minority (defined as a “human group with cultural, linguistic, racial values and geographical origin, numerically inferior compared to the majority group”) [32]. -Disease severity (classified according to:
- mild cases: clinical symptoms are mild and no manifestation of pneumonia can be found on images;
- moderate cases: with symptoms such as fever and respiratory tract symptoms and the manifestation of pneumonia can be seen on the imaging tests; and
- severe cases: respiratory distress, respiratory rate ≥ 30 breaths / min., pulse oxygen saturation ≤ 93% with room air at rest, arterial partial pressure of oxygen / oxygen concentration ≤ 300 mmHg.); to simplify comparison, moderate and severe cases were counted together [33]. -Vaccination status against covid-19 at the date of reinfection: vaccinated with 2 doses of vaccine, vaccinated with first booster for fall-winter 2021, vaccinated with fourth dose (second booster) for fall-winter 2022 and vaccinated with fifth dose (third booster) for fall-winter 2023 [34, 35, 36, 37, 38].
In our study, only Pizfer / BioNTech, Spikevax (mRNA-1273- Moderna), Vaxzevria, Oxford / AstraZeneca and Janssen (Johnson & Johnson) vaccines were used for the first and second doses. For the first booster, only messenger RNA (mRNA) was used. And only Moderna and Pfizer-BioNTech’s bivalent covid-19 vaccines were used for the second booster. The vaccines adapted to omicron XBB.1.5 Pfizer/BioNTech and Spikevax (Moderna) were used for the third booster in autumn-winter 2023.
Epidemiological Analysis
As much as possible, excessive fragmentation of the data was avoided to avoid low numbers of classes to be compared. The age of 65 years was used as the beginning of old age Figures with decimals were rounded to whole numbers to facilitate a more intuitive comparison [39, 40].
Ethical Issues
No personal data of the patients were used, but only group results, which were taken from the clinical history.
Results
15 cases of covid-19 reinfections were included during the study period. Of these cases, there were 2 that had presented 2 previous reinfections and one case that had presented 3 previous reinfections. 27% of cases had 5 doses of vaccine and 67% had 3 doses. Of the 15 cases of reinfection in the period studied, 27% were >65 years old, 67% women, and 27% socio-health workers.
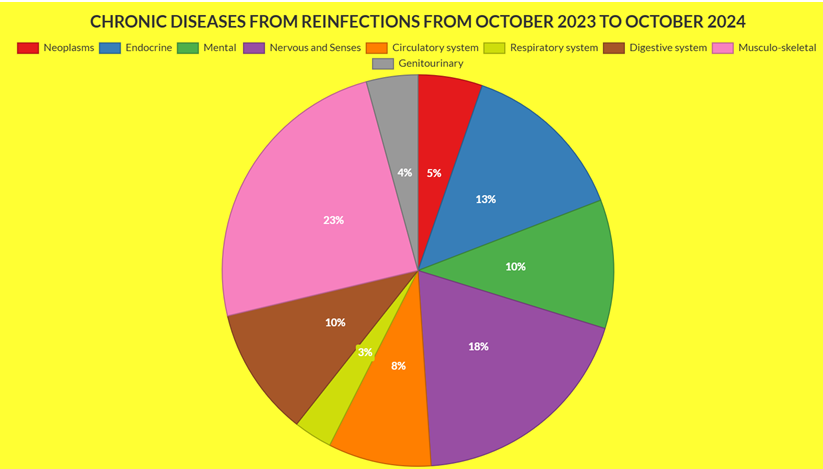
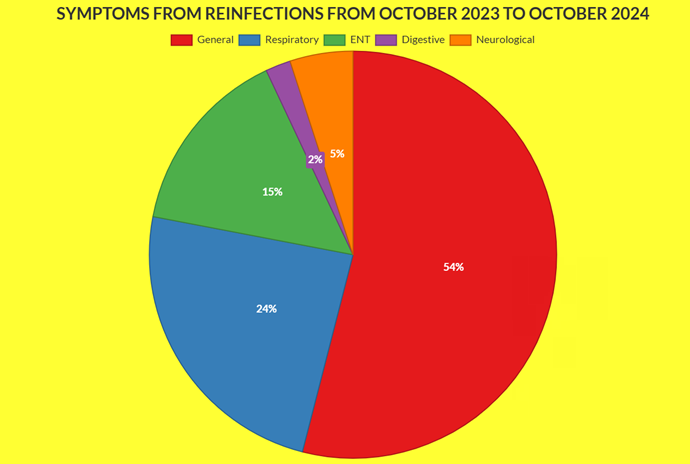
None presented moderate-severe severity. 80% had chronic diseases (23% Musculo-skeletal, 18% Nervous and Senses, 13% Endocrine, 10% Mental, 10% Digestive system, 10% Genitourinary). 54% of the symptoms were General (discomfort, asthenia, myalgia, fever, arthralgia), 24% were Respiratory (cough, dyspnea, chest pain), and 15% were Otorhinolaryngology (odynophagia, dysphonia, rhinorrhea, pharyngeal dryness-mucus), 5% Neurological (headache), and 2% Digestive (diarrhea, abdominal pain) (Tables 1-3, Figures 1 & 2).
| Variables | Reinfections from October 2023 to October 2024 N=15 |
|---|---|
| > = 65 years | 4 (27) |
| Women | 10 (67) |
| Health Care Workers | 4 (27) |
| Moderate-severe severity of reinfection | 0 |
| Chronic diseases presence | 12 (80) |
| Social-occupancy class of patients (people with some type of labor specialization) | 4 (27) |
| Complex family/ Problems in the family context | 2 (13) |
| Ethnic minority | 1 (7) |
| 1, 2 ó 3 doses | 10 (67) |
| 4 doses | 1 (7) |
| 5 doses | 4 (27) |
Table 1: ** Selected Variables from Reinfections from October 2023 to October 2024.
( ): Denotes percentages Table 1: Selected Variables from Reinfections from October 2023 to October 2024.
| Chronic Diseases* | Reinfections from October 2023 to October 2024 N=15 |
|---|---|
| -I Infectious | 0 |
| -II Neoplasms | 2 (5) |
| -III Diseases of the blood | 0 |
| -IV Endocrine | 5 (13) |
| -V Mental | 4 (10) |
| -VI-VIII Nervous and Senses | 7 (18) |
| -IX Circulatory system | 3 (8) |
| -X Respiratory system | 1 (3) |
| -XI Digestive system | 4 (10) |
| -XII Diseases of the skin | 0 |
| -XIII Musculo- skeletal | 9 (23) |
| -XIV Genitourinary | 4 (10) |
| TOTAL chronic diseases* | 39 (100) |
Table 2: ** Chronic Diseases from Reinfections from October 2023 to October 2024.
( ): Denotes percentages; *Patients could have more than one chronic disease. The percentages of chronic diseases are over the total of chronic diseases Table 2: Chronic Diseases from Reinfections from October 2023 to October 2024.
Symptoms Covid-19 Reinfec- tion* According to Who, Icd-10 Groups
Reinfections from October 2023 to Oc- tober 2024 N=15
General (discomfort, asthenia, myalgia, fever, artralgias) 29 (54)
Respiratory (cough, dyspnea, chest pain) 13(24)
ENT (anosmia / ageusia, odyno- phagia, rhinorrhea, pharyngeal dryness-mucus, epixtasis) 8 (15) Digestive (diarrhea, abdominal pain) 1 (2) Neurological (headache) 3 (5) Psychiatric 0 Skin 0 Urological 0 Total, symptoms* 54 (100) ( ): Denotes percentages; * Patients could have more than one symptom. The percentages are over the total of symptoms Table 3: Symptoms from Reinfections from October 2023 to October 2024.
Discussion
Main Findings
- Our main findings were:
- Covid-19 reinfections frequently had mild symptoms.
- They were more frequent in women.
- Most had chronic diseases, but not the classic comorbidities of the Circulatory system or Respiratory.
- There is a considerable frequency of reinfections in social-health workers, possibly because they are more exposed and undergo diagnostic testing more frequently.
Three fundamental factors must be considered to correctly evaluate our data: the local evolution of SARS-CoV variants, local degree of vaccination, and degree of diagnostic testing when symptoms are present.
a) The predominant variants in Spain during 2023 were those of the XBB family [38, 41, 42, 43, 44]. In January 2024 in Spain, XBB.1.5-like + F456L accounted for 42% and BA.2.86 for 44% of positive cases [26]. In July and August 2024, the KP.3 lineage was detected in 84% of cases [45]. In September 2024, the incidence of the XEC variant of the coronavirus, a new Omicron subvariant was increasing markedly in Spain. At that time, it was the second most common strain in cases recorded in September, although still far behind the main KP.3.3, with an incidence of 13% [46, 47].
b) On the other hand, in Spain, in November 2022, more than 60% of people over 80 years of age, and 37% of people over 60 years of age, already had the second booster dose of the covid-19 vaccine [48, 49]. And 60% of the population over 80 years of age has already received the vaccine adapted against the covid-19 subvariants of the 2023/2024 campaign [50].
c) In any case, the results must be evaluated with caution. In Spain, since April 28, 2022 there was a new “Surveillance and Control Strategy Against Covid-19” that included the non-performance of diagnostic tests, which were focused only on those over 60 years of age [12]. This means that positive cases have been counted with tests carried out in health services and with tests carried out at home and later reported to the GP. Thus, there is probably an underreporting. In addition, it is possible that many of the current infections are occurring with few symptoms or are confusing them with those of other mild conditions [41].
Comparison with Other Studies
Before Omicron, reinfections were rare. In the UK, reinfections accounted for 1% of cases in April 2021. With the introduction of Omicron, reinfection rates rose to 11% of all infections. In 2022, reinfections accounted for 25-27% of cases in the UK [6].
Reinfections with the virus that causes covid-19 are usually mild, but there is a chance to become seriously ill. A reinfected can also spread the virus to others. After you have Covid-19, your immune system responds in a number of ways. This immune response can provide protection against reinfection for several months, but it wanes over time. People with weakened immune systems who get an infection may have a limited or no immune response. As the virus evolves, new variants may emerge that are able to evade a person’s existing immunity. This could increase the risk of reinfection [51].
Compared with no reinfection, reinfection appears to contribute to additional risks of death, hospitalization, and sequelae, including pulmonary, cardiovascular, hematologic, diabetes, gastrointestinal, renal, mental health, musculoskeletal, and neurologic disorders. The risks appear to remain evident regardless of vaccination status [52].
In vulnerable populations, such as older people, viral respiratory illnesses often decompensate underlying diseases, such as diabetes, heart failure, chronic bronchitis, kidney disease, or liver cirrhosis. Therefore, as immunity to SARS-CoV-2 declines over time [53, 54], it has been estimated that 4-6 months after a first episode of Covid-19 or after being vaccinated (or both; hybrid immunity) a new SARS-CoV-2 infection is expected to be associated with a higher risk of hospitalization and death in the most fragile population [55].
But for many people who contract Covid-19 multiple times, subsequent infections will be as mild as the first or milder, data show, likely due to partial immunity from previous infections, vaccination, and the fact that the latest circulating variants often cause less severe symptoms [7].
Our data indicate that cases of reinfection are mild, but are frequently occurring in people with chronic diseases, and are showing a spectrum of these diseases different from those initially considered higher risk (such as cardiopulmonary disease) [56]. In our study, patients with reinfection had a wide diversity of infection and vaccination histories, which has been said to mean that greater vaccine exposure has different implications for different people [57].
It is suggested that for now, any new symptoms such as fever, sore throat, runny nose, or changes in taste or smell should be treated as a possible case of covid-19, and tests done to confirm if positive again. Furthermore, most of the existing tests used to detect covid-19 appear to be effective with the currently circulating variants [58].
Given the current situation in many places, such as in Spain, of not performing diagnostic tests in health services, except for those over 60 years of age and healthcare workers, many people with symptoms choose to perform tests at home [9]. In a previous study in the same population as the current one, we reported that women, young people, milder patients and those with lower risk, perform (and report it to the GP) covid-19 tests at home more frequently [59]. Probably related to these facts, in our study we found that reinfections were more frequent in women and social- healthcare workers.
In summary, each new infection with covid-19 carries a certain risk. Although these reinfections are mild, they occur in patients with comorbidity, and that means it is prudent to take steps to reduce the number of times a person is infected. With each reinfection there is an additional opportunity for the virus to cause harm in some way. This may also be true for long covid-19.
Limitations and Strengths of the Study
- The samples were small, so some data may cause misinterpretation.
- Asymptomatic cases were missing because they did not attend GP consultation, as no surveillance or systematic screening was done.
- There may be an underreporting of infections to GP of patients with a positive test at home. But given the situation of the GP as the gateway to the health system, the vast majority of positive covid-19 tests at home, is likely to be reported in GP office.
- The study has the strength of its longitudinality, characteristic of work in general medicine.
Conclusion
In the context of general medicine in Toledo (Spain), from 2020 to 2024, a period considered endemic, with high levels of vaccination, covid-19 reinfectons frequently had mild symptoms. They were more frequent in women. Most had chronic diseases, but they do not occur in people with the classic comorbidities of Circulatory system or Respiratory. There is a considerable frequency of reinfections in socio- health workers, possibly because they are more exposed and undergo diagnostic testing more frequently. Each new infection with covid-19 carries a certain risk. This means that it is prudent to take measures to reduce the number of times a person is infected. Staying up to date with covid-19 vaccines remains advisable.
References
-
News (2024) Experts say COVID-19 is endemic. What does that mean?. Harvard College, USA.
-
Biancolella M, Colona VL, Mehrian-Shai R, Watt JL, Luzzatto L, et al. (2022) COVID-19 2022 update: transition of the pandemic to the endemic phase. Hum Genomics 16(1): 19.
-
Otto SP, MacPherson A, Colijn C (2024) Endemic does not mean constant as SARS-CoV-2 continues to evolve. Evolution 78(6): 1092-1108.
-
Turabian JL (2023) Endemicity, Seasonal Variations, Lack of Epidemiological Surveillance and General Practice in Covid-19. J Cur Tre Inf Dis Res 1(1): 1-3.
-
Turabian JL (2023) COVID-19: From Epidemic to Endemic? The Evolution Remains Unpredictable. New Indicators Needed. J Infect Dise Treat 1(1): 1-4.
-
Zoco M, Jetelina K (2022) Epidemiology of reinfections. Su Epidemiólogo Local.
-
Blum D (2023) How Bad Is a Second (or Third or Fourth) Case of Covid?. The New York Time.
-
Miyo O (2020) Will we see protection or reinfection in COVID-19?. Nature Reviews Immunology 20(6): 351.
-
Ren X, Zhou J, Guo J, Hao C, Zheng M, et al. (2022) Reinfection in patients with COVID-19: a systematic review. Glob health res policy 7: 12.
-
Chen Y, Zhu W, Han X, Chen M, Li X, et al. (2024) How does the SARS-CoV-2 reinfection rate change over time? The global evidence from systematic review and meta- analysis. BMC Infect Dis 24(1): 339.
-
Ye Y (2023) China’s rolling COVID waves could hit every six months-infecting millions. Nature 618(7965): 442- 443.
-
Turabian JL (2022) An ostrich strategy for covid-19 is too risky. BMJ 377: 1112.
-
Crist C (2021) Unvaccinated People Likely to Catch COVID Repeatedly. Medscape.
-
Grant R, Sacks JA, Abraham P, Chunsuttiwat S, Cohen C, et al. (2023) When to update COVID-19 vaccine composition. Nat Med 29(4): 776-780.
-
Callaway E (2022) COVID ‘variant soup’ is making winter surges hard to predict. Nature 611(7935): 213-214.
-
Khoury DS, Docken SS, Subbarao K, Kent SJ, Davenport MP, et al. (2023) Predicting the efficacy of variant- modified COVID-19 vaccine boosters. Nat Med 29(3): 574-578.
-
Thompson D (2022) COVID reinfections are now common. Will getting a booster even help?.
-
Karmakar S (2022) COVID-19 Reinfection Risk Is Real: Pulmonologist Explains Importance of Booster Doses. India Dot.
-
Mallapaty S (2022) COVID reinfections surge during Omicron onslaught. Immunity acquired through previous infection is less effective against Omicron than against other variants, but the risk of severe COVID-19 remains low. Nature.
-
Weekly Epidemiological Report Community of Madrid. Week 40 (2024) SG de Vigilancia en Salud Pública. Dirección General de Salud Pública Consejería De Sanidad – Comunidad De Madrid.
-
Slezak J, Bruxvoort K, Fischer H, Broder B, Ackerson B, et al. (2021) Rate and severity of suspected SARS- Cov-2 reinfection in a cohort of PCR-positive COVID-19 patients. Clin Microbiol Infect 27(12): 1860.e7-1860. e10.
-
Altarawneh HN, Chemaitelly H, Ayoub HH, Tang P, Hasan MR, et al. (2022) Effects of Previous Infection and Vaccination on Symptomatic Omicron Infections. N Engl J Med 387(1): 21-34.
-
Ayoub HH, Tomy M, Chemaitelly H, Altarawneh HN, Coyle P, et al. (2023) Estimating protection afforded by prior infection in preventing reinfection: applying the test-negative study. Am J Epidemiol 193(6): 883-897.
-
CDC (2024) Testing for COVID-19. COVID-19.
-
Strauss AL (1984) Chronic illness and the quality of life. The C.V. Mosby Company, St Louis, USA.
-
WHO (2019) International Statistical Classification of Diseases and Health-Related Problems. ICD-10.
-
Royal Collage of General Practitioners (1986) The Classification and Analysis of General Practice Data. Occasional, pp: 26.
-
Donaldson RJ, Donaldson LJ (1983) Essential Community Medicine. MTP Press, Lancaster, USA.
-
Turabian JL (2017) Family Genogram in General Medicine: A Soft Technology that can be Strong. An Update. Res Med Eng Sci 3(1).
-
Russell LT (2020) Capturing Family Complexity in Family Nursing Research and Practice. J Fam Nurs 26(4): 287- 293.
-
Watts C, Shrader E (1998) How to do (or not to do)… The genogram: a new research tool to document patterns of decision-making, conflict and vulnerability within households. Health Policy Plan 13: 459-464.
-
Diccionario panhispánico del español jurídico (2022) Ethnic minority.
-
Mao S, Huang T, Yuan H, Lin M, Huang X, et al. (2020) Epidemiological analysis of 67 local COVID-19 clusters in Sichuan Province, China. BMC Public Health 20(1): 1525.
-
Ministry of Health (2021) COVID-19 early detection, surveillance and control strategy.
-
(2021) Update 10 Vaccination strategy against COVID-19 in Spain. Recommendations agreed upon in the Public Health Commission after review and proposal made by the Vaccination Program and Registry Report together with the COVID-19 Vaccination Technical Working Group and the COVID-19 Vaccination Working Group in the Child Population 2021.
-
Consejo Interterritorial (2022) COVID-19 vaccination recommendations for autumn in Spain. Sistema National Health.
-
Working Group on Vaccinations of the Spanish Society of Epidemiology (2023) COVID-19 and Flu Vaccination Guide, Autumn 2023.
-
Rodríguez-Artalejo F, Ruiz-Galiana J, Cantón R, Ramos PL, García-Botella A, et al. (2023) COVID-19: On the threshold of the fifth year. The situation in Spain. Rev Esp Quimioter 37(1): 17-28.
-
Reijneveld SA (2003) Age in epidemiological analysis. J Epidemiol Community Health 57(6): 397.
-
Reijneveld SA, Gunning-Schepers LJ (1994) Age, socioeconomic status, and mortality at the aggregate level. J Epidemiol Community Health 48(2): 146-150.
-
Health Alerts and Emergencies Coordination Center (2023) epidemiological situation of SARS-CoV-2 variants in Spain. Ministry of Health, Spain.
-
Viciosa M (2023) If you have covid today, the new variant O EG.5 or ‘Eris’ may have something to do with it (and it is not more serious). Newtral.
-
Pérez B (2023) The new eris variant, more contagious, already alerts doctors to the rebound in covid. The Newspaper.
-
Looi MK (2023) Covid-19: Hospital admissions rise in England amid fears of new variant and waning immunity. BMJ 382: 1833.
-
Smith DG (2023) What to Know About the New Dominant Covid Variant. EG.5 is spreading quickly, but experts say it’s no more dangerous than previous versions. Another new variant, called BA.2.86, is being closely watched because of its mutations. The New York Times.
-
AM (2024) XEC Covid variant: this is the new strain that is spreading across Europe and what its symptoms are. Onda Cero.
-
Jiménez PC (2024) XEC: New COVID variant threatens Europe, leaving 1,115 cases worldwide. Gaceta Médica.
-
Vacuna Covid-19 (2021) Covid-19 vaccination strategy in Spain. Ministry of Health.
-
Press Releases (2022) More than 60% of people over 80 years of age now have a second booster dose against COVID-19. Ministerio de Sanidad 11.11.
-
Noticias (2023) 60% of the population over 80 years old has already been vaccinated against Covid 19 in 2023. Ministerio de Sanidad, Gobierno de España.
-
COVID-19 (2024) About Reinfection. CDC.
-
Bowe B, Xie Y, Al-Aly Z (2022) Acute and postacute sequelae associated with SARS-CoV-2 reinfection. Nat Med 28(11): 2398-2405.
-
Woodbridge Y, Amit S, Huppert A, Kopelman NM (2022) Viral load dynamics of SARS-CoV-2 Delta and Omicron variants following multiple vaccine doses and previous infection. Nat Commun 13(1): 6706.
-
Sheikh K (2022) How long does immunity last against Covid? Is getting sick a second time worse? How can I prepare?. The New York Times.
-
Soriano V (2022) Repeat COVID: worse than the first time? blog.
-
Rosen CJ (2024) Viral Variants, Vaccinations, and Long Covid-New Insights. N Engl J Med 391(6): 561-562.
-
Wise J (2022) Covid-19: Omicron infection is poor booster to immunity, study finds. BMJ 377: o1474.
-
Guenot M (2024) Are covid-19 tests still working?. BMJ 387: q2070.
-
Turabian JL (2024) Covid-19 Infections with Positive Test at Home Versus in Health Services, In the Period from October 2022 to October 2023, In the General Medicine Office, In Toledo (Spain). J General Medicine and Clinical Practice 7(8).
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria
- Evidence of Spatial Clustering Distribution Patterns of Malaria in Epe, Lagos, Nigeria