Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
Background: Hypertension in youth, often linked to the obesity epidemic, is a precursor to future cardiovascular disease. However, data on uncontrolled hypertension and its management in this population are limited. The objective of this study was to examine the awareness and treatment of uncontrolled hypertension among US youths aged 16–24 years by weight status. Methods: This cross-sectional study used data from 812 participants (weighted n=36 million) from the National Health and Nutrition Examination Survey (NHANES) 2021–2023. Weight status was categorized as healthy weight or overweight/obesity. Uncontrolled hypertension, awareness, and treatment were defined according to standard guidelines and published literatures. Unadjusted and adjusted prevalence ratios (PR) and 95% confidence internals (CI) were estimated using Poisson regression models with robust error. Results: Prevalence of hypertension among youths aged 16–24 years was 13.7% (weighted n=4.9 million), and uncontrolled hypertension was 13.3% (weighted n=4.7 million). Overweight/obese youths had a significantly higher prevalence of uncontrolled hypertension than their healthy-weight peers (19.3% vs 7.6%; adjusted PR, 2.3; 95% CI, 1.5–3.7). Awareness was critically low, and treatment was nearly nonexistent. The prevalence of uncontrolled hypertension increased substantially with age (18.6% in ages 20–24 vs. 6.9% in ages 16–19 years) and was much higher in males (18.7% in males vs. 7.8% in females). Conclusions: A large proportion of US youths, particularly those with overweight/obesity, have uncontrolled hypertension. The low rates of awareness and pharmacological treatment identified in this study suggest a need for further evaluation of current screening and management practices within this population.
Jie W¹, Wang Y² MS and Liu X*³
¹The Lawrenceville High School, Lawrence Township, USA ²Axia Global Inc., New York City, USA ³UCLA School of Public Health, Los Angeles, USA
Abbreviations
AHT: Antihypertensive Therapy; BP: Blood Pressure; BMI: Body Mass Index; CDC: Centers for Disease Control and Prevention; CI: Confidence Interval; DBP: Diastolic Blood Pressure; IRB: Institutional Review Board; SBP: Systolic Blood Pressure; NHANES: National Health and Nutrition Examination Survey; NCHE: National Center for Health Statistics; PIR: Poverty-To-Income Ratio; PR: Prevalence Ratio; SE: Standard Error; US: United States
Background
Hypertension, high blood pressure (BP), is a leading modifiable risk factor for cardiovascular disease, stroke, and premature mortality [1]. Based on the most recent United States (US) guidelines, approximately 50% of US adults meet the criteria for hypertension (BP ≥130/80 mm Hg) [2, 3, 4]. Additionally, hypertension prevalence increases markedly with age, affecting 22% of those aged 18–39 years, 54% of those aged 40–59 years, and 75% of those aged 60 and older [4].
To reduce adverse health outcomes, achieving BP control through lifestyle modifications or antihypertensive medications (AHT) is critical [5]. Despite the importance of BP control, more than half of adults with hypertension have uncontrolled hypertension, often due to unawareness or lack of treatment [6].
Although traditionally considered an adult condition, hypertension also affects younger populations, reflecting the growing burden of overweight/obesity among youths [7, 8, 9]. In the US, approximately 40% of adolescents have overweight/obesity [10, 11]. Excess adiposity contributes to increased vascular resistance, altered sympathetic activity, and renal sodium retention, all of which promote higher BP levels even early in life [12, 13]. Although hypertension affects about 5% of US adolescents aged 12–19 years overall, the prevalence doubles to about 10% among those with obesity [10, 11].
Timely detection and effective management of hypertension during adolescence and young adulthood are crucial, as early life hypertension often persists into adulthood and accelerates the development of cardiovascular and renal complications [14, 15]. Despite these risks, hypertension in youth frequently remains underdiagnosed and undertreated, partly due to limited screening, evolving BP definitions, and the perception that hypertension is rare in this age group [16].
The underdiagnosis and undertreatment of hypertension among adolescents and young adults may lead to a large proportion of uncontrolled hypertension; however, previous studies have mainly focused on uncontrolled hypertension among adults [6, 17]. To our knowledge, no study has focused on uncontrolled hypertension among US youths, especially those with overweight/obesity in the post-pandemic era, when lifestyle, healthcare access, and health behaviors have shifted significantly. Understanding uncontrolled hypertension, especially among individuals with comorbid overweight or obesity in this population, can provide important context for evaluating current screening and management practices.
Using the most recent National Health and Nutrition Examination Survey (NHANES) cycle (2021-2023), this study aimed 1) to examine the awareness and treatment of uncontrolled hypertension among US youths aged 16–24 years overall and by weight status and 2) to stratify the results by age groups (16–19 vs. 20–24 years) and sex (females vs. males).
Methods
Study Population
This study utilized data from the most recent publicly available NHANES August 2021–August 2023 cycle [18]. The NHANES is a nationally representative survey designed to assess the health and nutritional status of the noninstitutionalized US population. Approximately 5,000 individuals are examined annually using a complex, multistage, probability-cluster sampling design with unequal selection probabilities. Data collection involves in-home interviews and physical examinations conducted at mobile examination centers.
All NHANES protocols are approved by the National Center for Health Statistics (NCHS) Research Ethics Review Board. Because this study involved a secondary analysis of publicly available, de-identified data, neither Institutional Review Board (IRB) review nor exempt determination was required.
The eligibility criteria for this study were as follows: 1) US youths (16–24 years) who participated in the interviews and physical examinations components of the NHANES 2021–2013; 2) individuals with ≥2 BP measurements at rest; and 3) individuals with height and weight measurements (Figure 1).
Overweight/Obesity
For youths aged 16–17 years, weight status was categorized using age- and sex-specific reference values from the 2000 Centers for Disease Control and Prevention (CDC) growth charts (healthy weight: body mass index (BMI)-for- age ≥5th to <85th percentiles; overweight: ≥85th to <95th percentiles; obesity: ≥95th percentiles) [19]. For young adults aged 18–24 years, weight status was categorized based on BMI (healthy weight: BMI <25 kg/m2; overweight: BMI ≥25 to <30 kg/m2; obesity: BMI ≥30 kg/m2).
Awareness and Treatment of Uncontrolled Hypertension The survey included an in-person examination of resting systolic blood pressure (SBP) and diastolic blood pressure (DBP) taken by certified examiners. The mean SBP and DBP values were used for estimations. For adolescents aged 16–17 years, elevated BP was defined as BP ≥90th to <95th percentile or SBP ≥120 mmHg to <95th percentile [10, 20]. Hypertension was defined as BP ≥95th percentile, BP ≥130/80 mmHg, or AHT use [10, 20].
Uncontrolled hypertension among adolescents was defined as BP ≥95th percentile or BP ≥130/80 mmHg, among those with hypertension [6, 10, 17]. For young adults 18–24 years, elevated BP was defined as SBP ≥120 mm to <130 mm Hg and DBP <80 mmHg. Hypertension was defined as BP ≥130/80 mmHg or AHT use [10, 17, 21]. Uncontrolled hypertension among young adults was defined as BP ≥130/80 mmHg, among those with hypertension [6, 10, 17]. Stage 2 hypertension was defined as BP ≥140/90 mmHg [5].
Hypertension awareness and treatment were only available in individuals ≥16 years. Awareness of hypertension was defined as a “yes” response to the question: “Have you ever been told by a doctor or other health professional that you had hypertension, also called high blood pressure?” Treatment of hypertension was defined by answering “yes” to the following question: “Are you now taking any medication prescribed by a doctor for your high blood pressure?” Awareness and treatment of hypertension were not collected for individuals <16 years [6].
Covariates
Most characteristics were self-reported during interviews, including age (16–19, 18–24 years), sex (male or female), race/ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic, non-Hispanic Asian, or other races), US- born (yes or no), and any health insurance (yes or no). The poverty-to-income ratio (PIR) was calculated using the NCHS as the ratio of self- or proxy-reported family income to the federal poverty threshold, taking family size into account. The PIR was categorized as less than 1.30 (low income), 1.30 to 3.49 (middle income), 3.50 or greater (high income), and unknown [22].
Diabetes (yes or no) was defined by self-report, random glucose ≥200 mg/L, or hemoglobin A1C ≥6.5% [23]. Hyperlipidemia (yes or no) was defined by self-report or total cholesterol ≥200 mg/dL [24]. Self-reported comorbidities were defined as a “yes” response to the question: “Have you ever been told by a doctor or other health professional that you had…”
Statistical Analyses
All analyses accounted for NHANES sampling weights and adjusted variance estimates for NHANES’ multistage, clustered sample design [18]. After applying sampling weights, the weighted results represented the US general population [18].
Weighted proportions and standard errors (SEs) were used to describe categorical variables. Poisson regression models with robust error estimation were used to compare outcomes between those with a healthy weight vs. overweight/obesity. Awareness and treatment were described among individuals with uncontrolled hypertension. Both unadjusted and adjusted prevalence ratios (PRs) with 95% confidence intervals (CIs) were estimated. The adjusted models included age, sex, race/ethnicity, and PIR categories as covariates. Hyperlipidemia and diabetes were not adjusted for, as they might be mediators. The results were stratified by age groups and sex. Interactions between weight status and age group, as well as between weight status and sex, were examined by adding interaction terms to the models.
Statistical significance was set at p-value <0.05. All analyses were conducted using R.4.2.2.
Results
Characteristics by Weight Status
Among 812 (weighted n=36 million) US youths aged 16–24 years, 441 (weighted n=18 million) had healthy weight and 371 (weighted n=17 million) had overweight/ obesity. The weighted proportion of females was 49.8% overall and was similar between the healthy-weight and overweight/obese groups (51.7% vs. 47.9%). Racial and ethnic compositions differed modestly according to the weight status. Youths with overweight/obesity had a higher prevalence of Hispanic (28.4% vs. 20.5%) and a lower prevalence of non-Hispanic Asian (6.2% vs. 11.7%) than those of healthy weight, whereas the proportion of non- Hispanic White (47.5% vs. 48.8%) and non-Hispanic Black (11.2% vs. 11.5%) participants was similar across groups. Most participants were US-born (90.2%) and insured (90.7%), with little variation by weight status. Socioeconomic differences were observed, as participants with overweight/ obesity were less likely to be from high-income households (14.5% vs. 22.0%) and more likely to be from middle-income households (35.9% vs. 27.7%). Hyperlipidemia (15.9% vs. 8.6%) was more common among youths with overweight/ obesity than among their healthy-weight counterparts, and the prevalence of diabetes was low in both groups (1.7% vs. 1.2%) (Table 1).
| Weighted % (SE) | 16-24 years | |||||
|---|---|---|---|---|---|---|
| 2021-2023 | All | Healthy weight | Overweight/obese | |||
| n=812 | n=441 | n=371 | ||||
| Female | 49.8 | 2.5 | 51.7 | 3.0 | 47.9 | 3.0 |
| US born | 90.2 | 1.8 | 89.2 | 2.1 | 91.3 | 2.1 |
| Health insurance | 90.7 | 1.7 | 90.8 | 1.9 | 90.6 | 1.7 |
| Race/ethnicity | ||||||
| Non-Hispanic White | 48.2 | 3.8 | 48.8 | 4.1 | 47.5 | 4.9 |
| Hispanic | 24.3 | 3.8 | 20.5 | 3.5 | 28.4 | 5.0 |
| Non-Hispanic Black | 11.3 | 1.8 | 11.5 | 1.6 | 11.2 | 2.5 |
| Non-Hispanic Asian | 9 | 2.2 | 11.7 | 3.1 | 6.2 | 1.8 |
| Others | 7.1 | 1.0 | 7.5 | 1.5 | 6.7 | 1.3 |
| Poverty to income ratio | ||||||
| High income (3.50 or greater) | 18.4 | 2.6 | 22 | 3.6 | 14.5 | 2.3 |
| Middle income (1.30 to 3.49) | 31.7 | 3.0 | 27.7 | 3.2 | 35.9 | 3.6 |
| Low income (less than 1.30) | 25.1 | 4.1 | 26.2 | 4.4 | 23.9 | 4.1 |
| Unknown | 24.9 | 1.9 | 24.1 | 2.3 | 25.7 | 2.3 |
| Comorbidities | ||||||
| Hyperlipidemia | 12.2 | 1.6 | 8.6 | 2.4 | 15.9 | 2.2 |
| Diabetes | 1.4 | 0.4 | 1.2 | 0.9 | 1.7 | 0.8 |
Table 1: Characteristics of US youths aged 16–24 years by weight status.
Abbreviations: SE, standard error; US, United States. Table 1: Characteristics of US youths aged 16–24 years by weight status.
Hypertension Control, Awareness, and Treatment by Weight Status
Among US youths aged 16–24 years, the weighted prevalence of elevated BP was 11.1%, with no significant difference between those of healthy weight and those with overweight/obesity (unadjusted prevalence, 11.1% vs. 11.0%; adjusted PR, 1.0; 95% CI, 0.5–1.8). Overall, 13.7% of the participants met the criteria for hypertension, including 8.0% of healthy-weight and 19.8% of overweight/obese youths. After adjustment, those with overweight/obesity had more than twice the prevalence of hypertension compared to their healthy-weight peers (adjusted PR, 2.3; 95% CI, 1.5– 3.5). The prevalence of stage 2 hypertension (BP ≥140/90 mmHg) was 2.2%, with higher a prevalence among those with overweight/obesity (3.0% vs. 1.4%), although this difference was not statistically significant (adjusted PR, 1.8; 95% CI, 0.3–12.6).
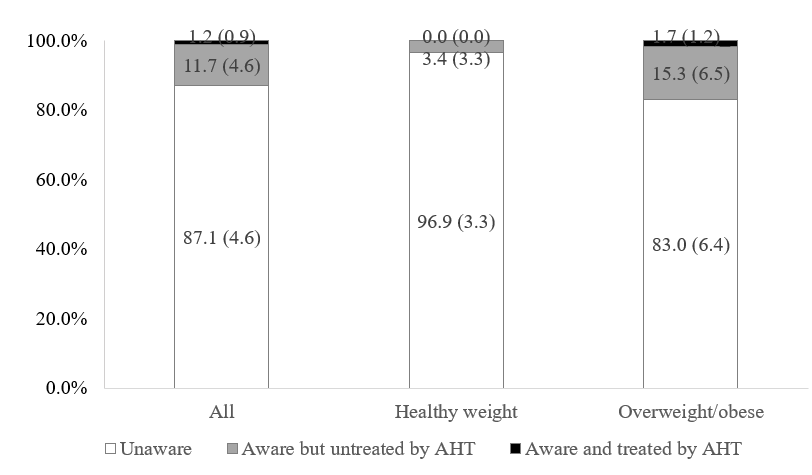
Almost all youths with hypertension had their BP uncontrolled, with the prevalence of 13.3% overall, including 7.6% among healthy-weight youths, and 19.3% among overweight/obese youths (adjusted PR, 2.3; 95% CI, 1.5–3.7). Among uncontrolled hypertension, 87.1% were unaware of their hypertension, 11.7% were aware of but untreated by AHT, and 1.2% were aware of and treated by AHT. In addition, more youths with a healthy weight were unaware of their hypertension than their overweight/obese counterparts (96.9% vs. 83.0%) (Table 2, Figure 2).
| Weighted % (SE) | 16-24 years | Unadjusted PR | Adjusted PR | |||||
|---|---|---|---|---|---|---|---|---|
| 2021-2023 | All | Healthy weight | Overweight/obese | (95% CI) *p<0.05 | (95% CI) *p<0.05 | |||
| n=812 | n=441 | n=371 | ||||||
| Elevated BP | 11.1 | 0.9 | 11.1 | 1.5 | 11 | 1.7 | 1.0 (0.6, 1.7) | 1.0 (0.5, 1.8) |
| Hypertension | 13.7 | 1.3 | 8 | 1.4 | 19.8 | 2.0 | 2.5 (1.7, 3.6)* | 2.3 (1.5, 3.5)* |
| Stage 2 hypertension | 2.2 | 0.8 | 1.4 | 0.8 | 3.0 | 1.3 | 2.1 (0.5, 9.7) | 1.8 (0.3, 12.6) |
| Currently treated by AHT | 0.6 | 0.2 | 0.4 | 0.3 | 0.8 | 0.4 | 2.0 (0.3, 12.5) | 2.4 (0.2, 38.0) |
| Controlled hypertension | 0.4 | 0.2 | 0.4 | 0.3 | 0.5 | 0.3 | 1.2 (0.1, 10.0) | 1.1 (0.1, 18.9) |
| Uncontrolled hypertension | 13.3 | 1.3 | 7.6 | 1.3 | 19.3 | 2.0 | 2.5 (1.7, 3.7)* | 2.3 (1.5, 3.7)* |
Table 2: Hypertension control of US youths aged 16–24 years by weight status.
Hypertension Control, Awareness, and Treatment by Weight Status and Age Groups
The prevalence of both hypertension and uncontrolled hypertension was substantially higher in young adults aged 20–24 years (19.1% and 18.6%, respectively) than in adolescents aged 16–19 years (7.3% and 6.9%, respectively). The interactions between weight status and age groups were not significant, indicating that the association between weight status and hypertension did not differ by age groups. Among youths aged 16–19 years, prevalence of hypertension was 7.3%, which was higher among those with overweight/obesity than among those with a healthy weight (11.4% vs. 4.3%; adjusted PR, 2.8; 95% CI, 1.0–7.7).
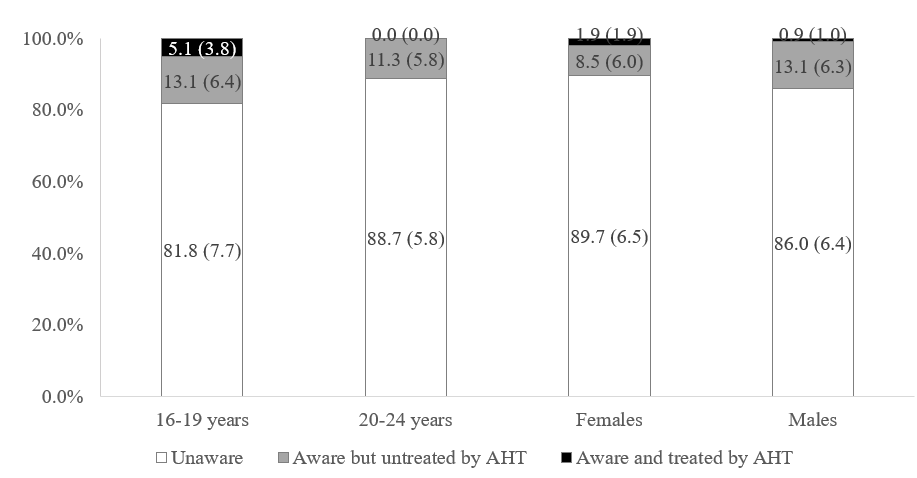
Uncontrolled hypertension affected 10.9% of overweight/ obese adolescents and 4.0% of healthy-weight adolescents. In young adults aged 20–24 years, hypertension prevalence was 19.1% overall, increasing from 12.0% among healthy- weight to 25.1% among overweight/obese participants (adjusted PR, 2.0; 95% CI, 1.0–3.9). Individuals with uncontrolled hypertension showed a similar pattern (24.7% vs. 11.5%; adjusted PR, 2.0; 95% CI, 1.1–3.8). Across both age groups, AHT use was rare (<2%) and stage 2 hypertension was uncommon (<4%). In addition, a large proportion of individuals with uncontrolled hypertension were unaware of their condition in both age groups (16–19 years: 81.8% vs. 20–24 years: 88.7%) (Table 3, Figure 3).
| Weighted % (SE) | 16-19 years | Unadjusted PR | Adjusted PR | |||||
|---|---|---|---|---|---|---|---|---|
| 2021-2023 | All | Healthy weight | Overweight/obese | (95% CI) *p<0.05 | (95% CI) *p<0.05 | |||
| n=524 | n=311 | n=213 | ||||||
| Elevated BP | 12.9 | 1.7 | 12.5 | 2.2 | 13.5 | 2.5 | 1.1 (0.6, 1.9) | 1.2 (0.7, 2.1) |
| Hypertension | 7.3 | 1.7 | 4.3 | 1.2 | 11.4 | 3.6 | 2.6 (1.1, 6.1)* | 2.8 (1.0, 7.7)* |
| Stage 2 hypertension | 1.1 | 0.5 | 0.2 | 0.2 | 2.3 | 1 | 10.1 (1.0, 107.4) | 10.1 (0.6, 158.6) |
| Currently treated by AHT | 0.7 | 0.4 | 0.3 | 0.3 | 1.4 | 0.8 | 4.5 (0.4, 57.9) | 6.0 (0.2, 183.8) |
| Controlled hypertension | 0.4 | 0.3 | 0.3 | 0.3 | 0.5 | 0.5 | 1.7 (0.1, 36.8) | 1.3 (0.2, 11.2) |
| Uncontrolled hypertension | 6.9 | 1.6 | 4 | 1.2 | 10.9 | 3.5 | 2.7 (1.1, 6.9)* | 2.9 (0.9, 9.5)* |
| 20-24 years | Unadjusted PR | Adjusted PR | ||||||
| All | Healthy weight | Overweight/obese | (95% CI) *p<0.05 | (95% CI) *p<0.05 | ||||
| n=288 | n=130 | n=158 | ||||||
| Elevated BP | 9.5 | 1.5 | 9.6 | 2.9 | 9.4 | 1.9 | 1.0 (0.4, 2.3) | 0.9 (0.3, 2.3) |
| Hypertension | 19.1 | 1.9 | 12 | 2.6 | 25.1 | 3.4 | 2.1 (1.1, 3.9)* | 2.0 (1.0, 3.9)* |
| Stage 2 hypertension | 3.1 | 1.2 | 2.7 | 1.6 | 3.5 | 1.9 | 1.3 (0.2, 7.7) | 1.0 (0.1, 10.0) |
| Currently treated by AHT | 0.5 | 0.3 | 0.5 | 0.5 | 0.5 | 0.4 | 0.9 (0.0, 19.4) | 0.8 (0.0, 39.1) |
| Controlled hypertension | 0.5 | 0.3 | 0.5 | 0.5 | 0.5 | 0.4 | 0.9 (0.0, 19.4) | 0.8 (0.0, 41.0) |
| Uncontrolled hypertension | 18.6 | 2.0 | 11.5 | 2.6 | 24.7 | 3.2 | 2.1 (1.2, 3.9)* | 2.0 (1.1, 3.8)* |
Table 3: Hypertension control of US youths aged 16–24 years by weight status and age groups.
Hypertension Control, Awareness, and Treatment by Weight Status and Sex
The prevalence of both hypertension and uncontrolled hypertension was substantially higher in males (18.9% vs. 18.7%, respectively) than females (8.6% and 7.8%, respectively). The interactions between weight status and sex were not significant, indicating that the association between weight status and hypertension did not differ by sex. Among females, hypertension prevalence was 8.6%, which was higher in those with overweight/obesity than in those of healthy weight, although the association was not significant (11.4% vs. 4.3%; adjusted PR, 1.9; 95% CI, 0.7–5.0). Uncontrolled hypertension affected 11.4% of overweight/ obese and 4.8% of healthy-weight females (adjusted PR, 2.1; 95% CI, 0.9–5.0). Among males, hypertension prevalence was 18.9%, increasing from 10.6% among healthy-weight to 27.0% among overweight/obese participants (adjusted PR, 2.4; 95% CI, 1.2–5.0). Uncontrolled hypertension was similarly higher among overweight/obese males (26.7% vs. 10.6%; adjusted PR, 2.4; 95% CI, 1.1–4.9). Across both females and males, AHT use was rare (<1%) and stage 2 hypertension was uncommon (<5%). In both sexes, a large proportion of individuals with uncontrolled hypertension were unaware of their condition (females: 89.7% vs. males: 86.0%) (Table 4, Figure 3).
| Weighted % (SE) | Female | Unadjusted PR | Adjusted PR | |||||
|---|---|---|---|---|---|---|---|---|
| 2021-2023 | All | Healthy weight | Overweight/obese | (95% CI) | (95% CI) | |||
| n=423 | n=116 | n=197 | ||||||
| Elevated BP | 3 | 0.8 | 3.8 | 1.4 | 2.1 | 1.2 | 0.5 (0.1, 2.6) | 2.3 (1.5, 3.5) |
| Hypertension | 8.6 | 1.5 | 4.3 | 1.2 | 11.4 | 3.6 | 2.1 (0.9, 5.3) | 1.9 (0.7, 5.0) |
| Stage 2 hypertension | 1.1 | 0.6 | 0.7 | 0.7 | 1.6 | 1.0 | 2.4 (0.2, 30.1) | 1.7 (0.1, 29.6) |
| Currently treated by AHT | 0.8 | 0.4 | 0.8 | 0.5 | 0.9 | 0.6 | 1.2 (0.1, 10.6) | 1.3 (0.1, 27.1) |
| Controlled hypertension | 0.7 | 0.4 | 0.8 | 0.5 | 0.6 | 0.6 | 0.8 (0.1, 10.7) | 0.7 (0.0, 17.8) |
| Uncontrolled hypertension | 7.8 | 1.6 | 4.8 | 1.6 | 11.4 | 2.6 | 2.4 (1.0, 5.6) | 2.1 (0.9, 5.0) |
| Male | Unadjusted PR | Adjusted PR | ||||||
| All | Healthy weight | Overweight/obese | (95% CI) *p<0.05 | (95% CI) *p<0.05 | ||||
| n=389 | n=215 | n=174 | ||||||
| Elevated BP | 19 | 1.7 | 18.9 | 2.9 | 19.2 | 3.1 | 1.0 (0.6, 1.8) | 1.7 (0.1, 29.6) |
| Hypertension | 18.9 | 2.0 | 10.6 | 2.5 | 27.0 | 3.4 | 2.5 (1.4, 4.6)* | 2.4 (1.2, 5.0)* |
| Stage 2 hypertension | 3.3 | 1.3 | 2.2 | 1.4 | 4.3 | 2.1 | 1.9 (0.4, 10.4) | 2.0 (0.2, 15.9) |
| Currently treated by AHT | 0.4 | 0.3 | 0 | 0 | 0.7 | 0.5 | - | - |
| Controlled hypertension | 0.2 | 0.2 | 0 | 0 | 0.4 | 0.4 | - | - |
| Uncontrolled hypertension | 18.7 | 2.1 | 10.6 | 2.5 | 26.7 | 3.6 | 2.5 (1.4, 4.6)* | 2.4 (1.1, 4.9)* |
Table 4: Hypertension control of US youths aged 16–24 years by weight status and sex.
Discussion
In this nationally representative cross-sectional study of US youths aged 16–24 years, we found a high prevalence of hypertension (13.7%), which was predominantly uncontrolled (13.3%). This burden was disproportionately borne by individuals with overweight/obesity, who had more than double the prevalence of uncontrolled hypertension than their healthy-weight peers (19.3% vs. 7.6%; adjusted PR 2.3). These findings highlight a potential gap in blood pressure management among U.S. youth, particularly those with overweight or obesity.
This study found that overweight/obese youths had a higher prevalence of uncontrolled hypertension, even after multivariable adjustment. This observation aligns with reported correlations between adiposity and BP [10, 11, 12, 13]. In addition, the observed higher prevalence of hyperlipidemia and differences in demographic factors, including a higher proportion of Hispanic ethnicity and lower household income, among youths with overweight/obesity suggests a clustering of cardiometabolic and socioeconomic risk factors that warrants further investigation.
Among US youths with hypertension, almost all of them (>95%) had uncontrolled hypertension. Among them, 87.1% were unaware of their condition, 11.7% were aware but untreated by AHT, and only 1.2% were aware and treated by AHT. These observations differ from those reported in the broader adult population. Among US adults with hypertension, approximately 50% of them had uncontrolled hypertension. Among them, 39% were unaware of their hypertension, 16% were aware of but untreated by AHT, and 45% were aware of and treated by AHT [6].
The potential reasons for these low rates of awareness and control are likely multifactorial. Youths and young adults often have infrequent contact with the healthcare system, and visits might be for acute issues where preventive screenings are overlooked [25, 26]. Underestimation of long- term risk by both youths, parents, and providers, coupled with challenges during the transition from pediatric to adult care, likely contributes to this problem [27, 28].
The management patterns observed in this study are noteworthy given the documented long-term associations of elevated BP in early life. Hypertension during adolescence and young adulthood is an indicator of sustained hypertension in later life and is associated with the early development of subclinical cardiovascular changes [29, 30, 31]. Maintaining uncontrolled BP during this period is linked to an increased lifetime risk for cardiovascular disease, including myocardial infarction and stroke, as well as end-organ damage such as chronic kidney disease [14, 32]. Therefore, the observed levels of awareness and treatment in this population may represent a potential area for intervention to help mitigate the risk of future adverse health outcomes.
A primary strength of this study is the use of a large, nationally representative sample, which enhances the external validity of the findings and allows for the calculation of robust prevalence estimates applicable to the broader US youth population. Additionally, the study employed rigorous clinical definitions for hypertension awareness, treatment, and control. By aligning these definitions with established clinical literature and evidence-based guidelines, the study ensures that the findings are both standardized and comparable to other epidemiological studies. Regarding limitations, the cross-sectional design prevents the establishment of temporal or causal relationships between overweight/obesity and uncontrolled hypertension. However, because the primary objective of this study was to describe the current prevalence of these conditions among US youth, the design remains appropriate.
Conclusions
In summary, these findings indicate that a notable prevalence of US youth, particularly those with overweight/ obesity, have hypertension that remains unrecognized and uncontrolled. These findings highlight several areas for further research, including the investigation of factors associated with these prevalence patterns and the assessment of potential management approaches.
Declarations
- Ethics Approval and Consent to Participate
- All NHANES protocols are approved by the National Center for Health Statistics (NCHS) Research Ethics Review Board. Because this study involved a secondary analysis of publicly available, de-identified data, neither Institutional Review Board (IRB) review nor exempt determination was required.
Consent for Publication
Not applicable.
Availability of Data and Materials
The NHANES datasets used and/or analyzed during the current study are publicly available.
Conflict of Interests
The authors declare that they have no conflict of interests.
Funding
The authors received no funding for the current study.
Authors’ Contributions
WJ and XL designed the study. WJ analyzed the data and was a major contributor in writing the manuscript. All authors read and approved the final manuscript.
References
-
Yusuf S, Joseph P, Rangarajan S, Islam S, Mente A, et al. (2020) Modifiable risk factors, cardiovascular dis- ease, and mortality in 155 722 individuals from 21 high-income, middle-income, and low-income coun- tries (PURE): a prospective cohort study. The Lancet 395(10226): 795-808.
-
Centers for Disease Control and Prevention (2023) Hy- pertension Cascade: Hypertension Prevalence, Treat- ment and Control Estimates Among US Adults Aged 18 Years and Older Applying the Criteria From the American College of Cardiology and American Heart Association’s 2017 Hypertension Guideline - NHANES 2017-2020.
-
Chobufo MD, Gayam V, Soluny J, Rahman EU, Enoru S, et al. (2020) Prevalence and control rates of hypertension in the USA: 2017–2018. International Journal of Cardiol- ogy Hypertension 6: 100044.
-
Ostchega Y, Fryar CD, Nwankwo T, Nguyen DT (2020) Hy- pertension prevalence among adults aged 18 and over: United States, 2017–2018. NCHS Data Brief pp: 1-8.
-
Whelton PK, Carey RM, Aronow WS, Casey DE, Collins KJ, et al. (2018) 2017 ACC/AHA/AAPA/ABC/ACPM/ AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the Ameri- can College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 71(6): 1269-1324.
-
Centers for Disease Control and Prevention (2012) Vi- tal signs: awareness and treatment of uncontrolled hy- pertension among adults-United States, 2003-2010. MMWR: Morbidity & Mortality Weekly Report 61(35): 703-709.
-
Jeong SI, Kim SH (2024) Obesity and hypertension in children and adolescents. Clinical Hypertension 30(1): 23.
-
Falkner B (2017) Monitoring and management of hy- pertension with obesity in adolescents. Integrated blood pressure control pp: 33-39.
-
Rosner B, Cook NR, Daniels S, Falkner B (2013) Child- hood blood pressure trends and risk factors for high blood pressure: the NHANES experience 1988–2008. Hypertension 62(2): 247-254.
-
Jackson SL (2018) Hypertension among youths-United States, 2001–2016. MMWR Morbidity and mortality weekly report 67(27): 758-762.
-
Hardy ST, Sakhuja S, Jaeger BC, Urbina EM, Suglia SF, et al. (2021) Trends in blood pressure and hypertension among US children and adolescents, 1999-2018. JAMA network open 4(4): e213917.
-
Hall JE, do Carmo JM, da Silva AA, Wang Z, Hall ME (2019) Obesity, kidney dysfunction and hypertension: mecha- nistic links. Nature reviews nephrology 15(6): 367-385.
-
Hall JE, Hildebrandt DA, Kuo J (2001) Obesity hyperten- sion: role of leptin and sympathetic nervous system. American journal of hypertension 14(S3): 103S-115S.
-
Yang L, Magnussen CG, Yang L, Bovet P, Xi B (2020) El- evated blood pressure in childhood or adolescence and cardiovascular outcomes in adulthood: a systematic re- view. Hypertension 75(4): 948-955.
-
Liao Y-Y, Ma Q, Chu C, Wang Y, Zheng W-L, et al. (2020) The predictive value of repeated blood pressure mea- surements in childhood for cardiovascular risk in adults: the Hanzhong Adolescent Hypertension Study. Hyper- tension Research 43(9): 969-978.
-
Neuhauser H, Adler C, Sarganas G (2019) Selective blood pressure screening in the young: quantification of pop- ulation wide underestimation of elevated blood pres- sure. International Journal of Hypertension 2019(1): 2314029.
-
Tang R, An J, Bellows BK, Moran AE, Zhang Y (2025) Trends in Hypertension Prevalence, Awareness, Treat- ment, and Control Among US Young Adults, 2003–2023. American Journal of Hypertension 38(8): 551-559.
-
Centers for Disease Control and Prevention (CDC) Na- tional Center for Health Statistics. National Health and Nutrition Examination Survey (NHANES).
-
Flegal KM, Cole TJ (2013) Construction of LMS param- eters for the Centers for Disease Control and Prevention 2000 growth charts. Natl Health Stat (63): 1-3.
-
Flynn JT, Kaelber DC, Baker-Smith CM, Blowey D, Carroll AE, et al. (2017) Clinical practice guideline for screening and management of high blood pressure in children and adolescents. Pediatrics 140(3): e20171904.
-
Carey RM, Whelton PK, 2017 ACC/AHA Hypertension Guideline Writing Committee (2018) Prevention, detec- tion, evaluation, and management of high blood pres- sure in adults: synopsis of the 2017 American College of Cardiology/American Heart Association Hypertension Guideline. Annals of internal medicine 168(5): 351-358.
-
Ogden CL, Lamb MM, Carroll MD, Flegal KM (2010) Obe- sity and socioeconomic status in adults: United States, 2005-2008. NCHS Data Brief (50): 1-8.
-
American Diabetes Association Professional Practice Committee (2022) 2. Classification and diagnosis of dia- betes: Standards of Medical Care in Diabetes-2022. Dia- betes Care 45(Supplement 1): S17-S38.
-
Jellinger PS, Handelsman Y, Rosenblit PD, Bloomgarden ZT, Fonseca VA, et al. (2017) American Association of Clinical Endocrinologists and American College of En- docrinology guidelines for management of dyslipidemia and prevention of cardiovascular disease. Endocrine Practice 23: 1-87.
-
Hassan A, Blood EA, Pikcilingis A, Krull EG, McNickles LQ, et al. (2013) Youths’ health-related social problems: concerns often overlooked during the medical visit. Jour- nal of Adolescent Health 53(2): 265-271.
-
Irwin Jr CE, Adams SH, Park MJ, Newacheck PW (2009) Preventive care for adolescents: few get visits and fewer get services. Pediatrics 123(4): e565-e572.
-
Coyne I, Sheehan A, Heery E, While AE (2019) Health- care transition for adolescents and young adults with long‐term conditions: Qualitative study of patients, par- ents and healthcare professionals’ experiences. Journal of clinical nursing 28(21-22): 4062-4076.
-
McDonagh JE (2005) Growing up and moving on: transi- tion from pediatric to adult care. Pediatric transplanta- tion 9(3): 364-372.
-
Allen NB, Siddique J, Wilkins JT, Shay C, Lewis CE, et al. (2014) Blood pressure trajectories in early adulthood and subclinical atherosclerosis in middle age. Jama 311(5): 490-497.
-
Drukteinis JS, Roman MJ, Fabsitz RR, Lee ET, Best LG, et al. (2007) Cardiac and systemic hemodynamic charac- teristics of hypertension and prehypertension in adoles- cents and young adults: the Strong Heart Study. Circula- tion 115(2): 221-227.
-
Marcon D, Tagetti A, Fava C (2019) Subclinical organ damage in children and adolescents with hypertension: current guidelines and beyond. High Blood Pressure & Cardiovascular Prevention 26(5): 361-373.
-
Robinson CH, Chanchlani R (2022) High blood pressure in children and adolescents: current perspectives and strategies to improve future kidney and cardiovascular health. Kidney international reports 7(5): 954.
- Epidemiological Surveillance and Rumors on Social Media
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria
- Evidence of Spatial Clustering Distribution Patterns of Malaria in Epe, Lagos, Nigeria