Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
Childhood immunization is one of the most cost-effective public health interventions, preventing morbidity and mortality from vaccine-preventable diseases. In Bangladesh, the Expanded Programme on Immunization (EPI) offers free vaccination, yet children in urban slums remain at higher risk of incomplete or delayed immunization. This cross-sectional study investigates parental knowledge, attitudes, and perceptions regarding childhood immunization in selected Dhaka slums to identify strategies for strengthening vaccine coverage and supporting the goals of the Immunization Agenda 2030 (IA-2030). A total of 270 parents of children aged 0–5 years were recruited through purposive sampling, and data were collected using a semi-structured questionnaire administered face-to-face in Bengali. Socio-demographic data, awareness of immunization, knowledge of vaccine schedules, and parental attitudes were assessed. Results indicate that nearly all parents (99.3%) were aware of immunization, with health workers serving as the primary source of information (65.9%), while media and other sources contributed minimally. Most respondents (83.3%) recognized vaccination as protective against infectious diseases, and 75.2% acknowledged its role in reducing child mortality. Awareness of vaccine side effects was reported by 78.1%, and 70.7% were familiar with the term EPI. Knowledge gaps were observed regarding birth doses, multiple dose schedules, and contraindications, with only 11.5% aware of vaccines administered immediately after birth and 58.1% understanding the importance of dose intervals. Attitudes toward immunization were overwhelmingly positive: 80.7% considered EPI vaccines safe, 91.5% recognized their essentiality for child health, and 88.9% indicated willingness to encourage others to vaccinate. Immunization practices were strong, with 98.5% reporting regular vaccination and 86.1% of children aged two and above having completed the EPI schedule. However, 37% of children received additional non-EPI vaccines, highlighting increasing parental engagement beyond routine programs. The study underscores that while parental attitudes toward vaccination are favorable, gaps in knowledge may lead to missed opportunities. Targeted educational interventions, communitybased engagement, and reinforcement through health worker communication are recommended to improve coverage in slum populations. Understanding parental perceptions and addressing misconceptions are pivotal to achieving equitable immunization coverage and reducing preventable child mortality under IA-2030.
Introduction
Childhood immunization remains one of the most effective public health interventions globally, preventing millions of deaths from vaccine-preventable diseases each year [1]. Vaccines stimulate the immune system to develop protection against infectious agents, offering both individual immunity and community-level herd immunity [2]. Before the introduction of systematic immunization programs, childhood infectious diseases such as measles, polio, tetanus, and diphtheria were leading causes of morbidity and mortality among children worldwide [3]. The Expanded Programme on Immunization (EPI), initiated by the World Health Organization (WHO) and implemented in Bangladesh in 1979, has been a cornerstone of national immunization strategies, aiming to achieve high coverage and prevent child mortality due to vaccine-preventable diseases [4]. Despite these efforts, disparities in immunization coverage persist, particularly in marginalized communities such as urban slums, where children are at higher risk of missing routine vaccines [5].
In Bangladesh, the EPI program provides vaccines free of charge, yet coverage remains suboptimal in certain populations. By 1993–94, full protection among children aged 12–23 months had increased to nearly 60%, preventing an estimated 1.2 million child deaths between 1987 and 1997 [6]. Nevertheless, gaps in parental knowledge, misconceptions, and socio-economic barriers continue to challenge the program’s effectiveness [7]. Parental knowledge and attitudes are particularly influential because parents are the primary decision-makers regarding their children’s health. Studies have shown that parental awareness, perceptions, and attitudes toward vaccines strongly determine immunization uptake [8]. Misbeliefs about vaccine safety, religious concerns, and fear of side effects can lead to delayed vaccination or dropout, which undermines the success of immunization programs [9].
Urban slum populations face unique challenges. Slum dwellers often experience overcrowding, poor sanitation, limited access to health services, and economic constraints that hinder routine healthcare access, including immunization [10]. Even when vaccines are freely available, barriers such as lack of awareness, low literacy, and misconceptions persist. Understanding parental knowledge, attitudes, and perceptions (KAP) toward childhood vaccination is crucial for tailoring interventions that improve immunization coverage in these vulnerable populations. While previous studies in Bangladesh have focused on rural areas, urban slums remain underrepresented in immunization research [11]. Therefore, exploring parental KAP in slum settings is essential to strengthen EPI implementation and achieve targets under the Immunization Agenda 2030 (IA-2030), which emphasizes equitable access to vaccines and reducing preventable child deaths globally [12].
This study aims to assess the level of knowledge and attitudes toward childhood immunization among parents of children aged 0–5 years in selected urban slums of Dhaka city. By identifying knowledge gaps, misconceptions, and sources of information, this research seeks to inform strategies for enhancing parental engagement and improving immunization coverage in slum communities.
Methodology
Study Design: A cross-sectional descriptive study was conducted among parents of children aged 0–5 years residing in Moghbazar, Malibag, and Khilgaon slums.
Study Period: January 2022 to December 2022.
Sample: Using purposive sampling, 270 parents were recruited. The intended sample size was 384, but it was reduced due to non-response and COVID-19 constraints.
Inclusion & Exclusion Criteria
Inclusion: Parents residing with children aged 0–5 years in selected slums. Exclusion: Parents living separately from children, children >5 years old, or unwilling participants.
Data Collection: Face-to-face interviews were conducted using a pretested semi-structured questionnaire in Bengali. The questionnaire assessed socio-demographics, knowledge, and attitudes towards immunization.
Data Analysis
Data was checked, coded, and analyzed using IBM SPSS version 25. Parental attitudes were measured on a three- point Likert scale (1 = bad, 2 = undecided, 3 = good).
Ethical Consideration: The study was approved by the Institutional Review Board of Bangladesh Open University. Informed consent was obtained, and confidentiality was maintained.
Results
Socio-Demographics
The study population primarily consisted of women (65.9%) aged between 20 and 30 years (60.4%). Most respondents were Muslim (96.7%) and had completed primary education (50.7%). Occupations were largely domestic, including housewives (37.4%), housemaids (17%), and day laborers (16.7%). Families were predominantly nuclear (71.1%) with 4–6 members, and the majority reported a monthly household income between 10,000 and 15,000 BDT (42.2%). Housing conditions were mainly tin-shed dwellings (78.9%), reflecting the socioeconomic context of Dhaka slums.
Children Profile
The children included in the study were mostly five years old (60.4%), with a higher proportion of females (61.9%) compared to males (38.1%).
Knowledge about Immunization
Awareness of childhood immunization was nearly universal (99.3%), with health workers serving as the primary source of information for 65.9% of respondents, while television and radio accounted for only 8.1%. A significant majority (83.3%) recognized that vaccination protects against infectious diseases, and 75.2% acknowledged its role in reducing child mortality. Awareness of possible side effects was reported by 78.1% of participants, and 70.7% were familiar with the term Expanded Program on Immunization (EPI). Knowledge regarding the timing of vaccination varied: only 11.5% knew about vaccines administered immediately after birth, while 77% understood that most vaccinations occur during the first year of life. The importance of maintaining intervals between multiple doses for effective immunity was understood by 58.1% of respondents. Immunization practices were strong, with 98.5% reporting that their children were immunized regularly, and 86.1% of children aged two years and older had completed all EPI vaccinations. Additionally, 37% of children received non-EPI vaccines, including Rota, Hepatitis-A, and Cholera vaccines.
Attitude towards Immunization
Attitudes toward vaccination were overwhelmingly positive. Most respondents considered EPI vaccines safe (80.7%) and reported vaccinating their children without hesitation (81.1%). The essentiality of vaccines was acknowledged by 91.5%, and 86.7% agreed that vaccination is necessary for a child to lead a healthy life. Over half of the participants (53%) disagreed with circulating vaccine- related rumors, while 57.4% rejected the notion of religious prohibition of vaccination. A strong majority (88.9%) indicated they would encourage others to vaccinate, and 60.7% believed that the provision of free vaccines does not compromise reliability. Finally, 75.9% of respondents perceived vaccines as effective in providing protection against disease.
| Sex | Frequency | Percentage (%) |
|---|---|---|
| Male | 92 | 34.1 |
| Female | 178 | 65.9 |
| Total | 270 | 100 |
| Age Group (years) | ||
| <20 | 31 | 11.5 |
| 20–30 | 163 | 60.4 |
| 31–40 | 51 | 18.9 |
| >40 | 25 | 9.3 |
| Total | 270 | 100 |
| Religion | ||
| Muslim | 261 | 96.7 |
| Hindu | 8 | 3 |
| Buddhist | 1 | 0.4 |
| Total | 270 | 100 |
| Education Level | ||
| Illiterate | 93 | 34.4 |
| Primary | 137 | 50.7 |
| Secondary | 33 | 12.2 |
| Higher Secondary | 7 | 2.6 |
| Total | 270 | 100 |
| Occupation | ||
| Housewife | 101 | 37.4 |
| Housemaid | 46 | 17 |
| Day labor | 45 | 16.7 |
| Service holder | 35 | 13 |
| Businessman | 29 | 10.7 |
| Other | 12 | 4.4 |
| Family Type | ||
| Nuclear | 192 | 71.1 |
| Joint | 78 | 28.9 |
| Total | 270 | 100 |
| Members | ||
| Two | 3 | 1.1 |
| Three | 50 | 18.5 |
| Four | 88 | 32.6 |
| Five | 47 | 17.4 |
| Six | 45 | 16.7 |
| >6 | 37 | 13.7 |
| Total | 270 | 100 |
| Monthly Income (BDT) | ||
| <5,000 | 33 | 12.2 |
| 5,000–10,000 | 72 | 26.7 |
| 10,000–15,000 | 114 | 42.2 |
| >15,000 | 51 | 18.9 |
| Total | 270 | 100 |
| House Type | ||
| Tin shed | 213 | 78.9 |
| Kacha | 38 | 14.1 |
| Semi Pacca | 11 | 4.1 |
| Pacca | 8 | 3 |
Table 1: Socio-Demographic Characteristics of Respondents.
| Age (years) | Frequency | Percentage (%) |
|---|---|---|
| 0–1 | 25 | 9.3 |
| 2 | 12 | 4.4 |
| 3 | 19 | 7 |
| 4 | 51 | 18.9 |
| 5 | 163 | 60.4 |
| Gender | ||
| Male | 103 | 38.1 |
| Female | 167 | 61.9 |
Table 2: Child Profile.
| Awareness | Frequency | Percentage (%) |
|---|---|---|
| Yes | 268 | 99.3 |
| No | 2 | 0.7 |
| Source | ||
| Health worker | 178 | 65.9 |
| Radio/TV | 22 | 8.1 |
| NGO | 14 | 5.2 |
| Neighbors | 16 | 5.9 |
| Billboard | 3 | 1.1 |
| Not informed | 28 | 10.4 |
| Response-Immunization Protects Children | ||
| Yes | 225 | 83.3 |
| No | 45 | 16.7 |
| Response-Vaccination Reduces Child Mortality | ||
| Yes | 203 | 75.2 |
| No | 67 | 24.8 |
| Response- Knowledge of Side Effects | ||
| Yes | 211 | 78.1 |
| No | 59 | 21.9 |
| Response- Knowledge of EPI | ||
| Yes | 191 | 70.7 |
| No | 79 | 29.3 |
| Response- Child Has EPI Vaccination Card | ||
| Yes | 254 | 94.1 |
| No | 16 | 5.9 |
| Response- Child Received Vaccine Just After Birth | ||
| Yes | 31 | 11.5 |
| No | 239 | 88.5 |
| Response- Knowledge About Vaccination in First Year | ||
| Yes | 208 | 77 |
| No | 62 | 23 |
| Response- Knowledge of Multiple Doses | ||
| Yes | 157 | 58.1 |
| No | 113 | 41.9 |
| Response- Child Completed EPI Vaccination (Age ≥2) | ||
| Yes | 211 | 86.1 |
| No | 34 | 13.9 |
| Type of Vaccine | ||
| Only EPI | 170 | 63 |
| EPI + Others | 100 | 37 |
| Response- Minor Illnesses Not Contraindicated | ||
| Yes | 29 | 10.7 |
| No | 241 | 89.3 |
Table 3: Knowledge About Childhood Immunization.
| Statement | Agree (3) | Neutral (2) | Disagree (1) | Mean ± SD |
|---|---|---|---|---|
| EPI vaccines are safe | 218 | 44 | 8 | 2.78±0.48 |
| Vaccinated child without hesitation | 219 | 17 | 34 | 2.68±0.61 |
| Vaccines essential for child health | 247 | 15 | 8 | 2.87±0.44 |
| Childhood immunization necessary for healthy life | 234 | 23 | 13 | 2.81±0.50 |
| Rumors about vaccines are true | 41 | 87 | 142 | 1.66±0.61 |
| Religion prohibits vaccination | 27 | 95 | 148 | 1.60±0.61 |
| Encourage others to vaccinate | 240 | 19 | 11 | 2.85±0.49 |
| Free vaccines are unreliable | 53 | 53 | 164 | 1.83±0.63 |
| Vaccines provide protection | 205 | 43 | 22 | 2.68±0.56 |
Table 4: Attitude Toward Immunization.
- Positive attitude (mean ≥2.5) toward safety, essentiality, and encouragement.
- Neutral on minor rumors and free vaccines.
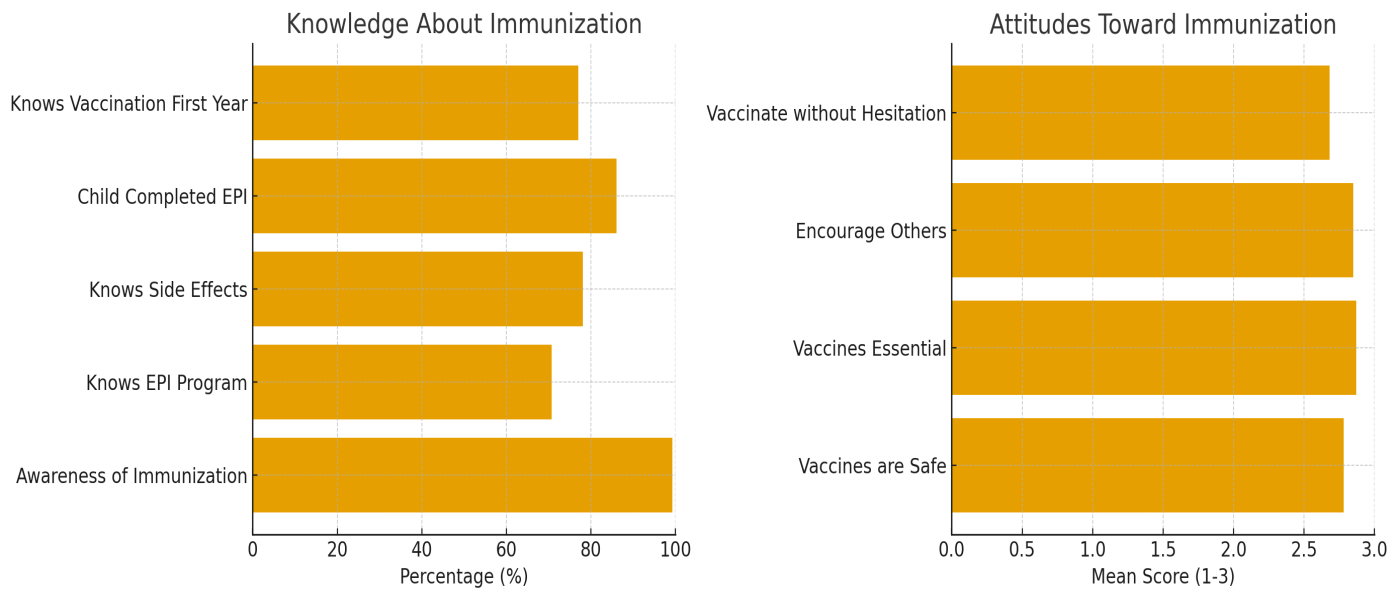
Figure: Knowledge and Attitude Toward Immunization.
Discussion
The present cross-sectional study highlights the knowledge, attitudes, and practices of parents regarding childhood immunization in urban slums of Dhaka. The findings suggest generally positive attitudes toward vaccines, although significant gaps in knowledge remain, particularly regarding vaccine schedules, contraindications, and the timing of birth doses.
The demographic profile of the respondents indicates that the majority of parents were young adults aged 20–30 years, reflecting a population likely to have young children and actively engage in healthcare decision-making. Females predominated in the sample, consistent with the expectation that mothers often accompany children to health facilities and are more directly involved in daily child care [13]. Literacy levels were moderate, with over half completing primary education, yet a substantial proportion (34.4%) were illiterate, which may impact the understanding of vaccine-related information and instructions [14]. The socioeconomic data show that most families had modest incomes and lived in tin-shed houses, highlighting potential structural barriers to accessing healthcare, such as financial constraints and mobility issues [15].
Awareness of childhood immunization was high, with 99.3% of parents acknowledging the importance of vaccines. Health workers emerged as the primary source of information (65.9%), underlining the critical role of frontline healthcare personnel in educating and motivating parents. Other sources, including media, NGOs, and neighbors, played minor roles. This reinforces the necessity for consistent health education delivered by trained personnel, particularly in underserved areas [16]. Despite high general awareness, one-quarter of parents were unaware that vaccination reduces child mortality, and 41.9% did not understand the importance of multiple doses for adequate immunity. Similarly, 89.3% did not know that minor illnesses, such as colds or diarrhea, are not contraindications for vaccination. These gaps could contribute to missed opportunities and vaccination dropouts, highlighting the need for targeted educational interventions [17].
The study also examined parental attitudes using a three-point Likert scale. Overall, attitudes were favorable, with the majority agreeing that EPI vaccines are safe, essential for a healthy life, and capable of protecting children from infectious diseases. Most parents expressed willingness to vaccinate their children without hesitation and to encourage others in their community to do the same. The strong positive attitudes observed may partly reflect the long-standing presence and visibility of EPI programs in Dhaka and the trust placed in health workers [18]. However, misconceptions persist; a small proportion of respondents agreed with rumors about vaccines or doubted the reliability of free vaccines. These findings are consistent with prior studies suggesting that even when overall vaccine acceptance is high, misinformation can influence specific beliefs and behaviors [19].
The study highlights a critical disconnect between knowledge and practice in certain areas. While most parents understood the general importance of vaccination and maintained vaccination cards (94.1%), few were aware of the timing of birth doses, and some lacked understanding of EPI terminology. This gap emphasizes that knowledge alone may not guarantee complete compliance; reinforcement through repeated counseling, community engagement, and simplified communication materials is necessary [20].
In terms of immunization coverage, the results indicate high adherence, with 98.5% reporting regular vaccination and 86.1% acknowledging completion of EPI schedules among children over two years of age. The majority of children received only EPI vaccines, while 37% received additional vaccines such as Rota, Hepatitis-A, or Cholera, reflecting growing parental awareness and the expanding availability of vaccines beyond the national schedule. The findings also show that health problems rarely caused incomplete vaccination, suggesting that dropout is more likely influenced by parental knowledge and attitudes than by child health status [21].
This study explores strengthening the Expanded Program on Immunization (EPI) through active parental engagement in Dhaka’s slums. By understanding caregivers’ knowledge, attitudes, and practices, the initiative aims to increase immunization coverage, address vaccine hesitancy, and generate community-driven strategies, contributing to IA-2030 goals for equitable and sustainable immunization.
The study’s limitations include the non-random sampling technique, the restricted geographical scope, and the relatively small sample size, which may affect generalizability. Additionally, social desirability bias may have influenced responses, particularly regarding attitudes toward vaccination. Nevertheless, the study provides valuable insights for public health practitioners and policymakers aiming to strengthen EPI coverage in urban slums.
Recommendations
Continuous educational campaigns targeting both mothers and fathers can reinforce knowledge about vaccine schedules, side effects, and contraindications. Collaborations with local authorities, NGOs, and community health workers are crucial for ensuring consistent outreach. Technology-based solutions, such as mobile reminders and digital health records, could further support adherence and tracking of vaccination coverage. Future research should involve larger, representative samples across multiple urban slums to provide a comprehensive assessment of parental knowledge and attitudes toward childhood immunization in Dhaka [22].
Conclusion
In conclusion, this study demonstrates that while parental attitudes toward childhood immunization in Dhaka slums are generally positive, gaps in knowledge persist, particularly regarding birth doses, multiple dosing schedules, and contraindications. Health worker engagement remains the most effective channel for information dissemination, and leveraging community-based strategies is essential to achieve full immunization coverage. Understanding and addressing parental perceptions and beliefs are pivotal to the success of EPI programs and the broader goal of reducing preventable child mortality under IA-2030.
References
-
Census of Bangladesh. (2022) Wikipedia.
-
Alshammari SZ, Alfayyad I, Altannir Y, Al-Tannir M (2021) Parental awareness and attitude about childhood immunization in Riyadh, Saudi Arabia: A cross-sectional study. International Journal of Environmental Research and Public Health 18(16): 8465.
-
Andre FE, Booy R, Bock HL, Clemens J, Datta SK, et al. (2008) Vaccination greatly reduces disease, disability, death and inequity worldwide. Bulletin of the World Health Organization 86(2): 140–146.
-
Anichini G, MG Cusi (2022) Immune response analysis to measles virus in subjects vaccinated with MMR vaccine and naturally infected subjects. Vaccines 8(1): 66.
-
Awadh AI, Hassali MA, Al-Lela OQ, Bux SH, Elkalmi RM, et al. (2014) Immunization knowledge and practice among Malaysian parents: A questionnaire development and pilot-testing. BMC Public Health 14: 1107.
-
Bhuiya A, Bhuiya, I, Chowdhury M (1995) Factors affecting acceptance of immunization among children in rural Bangladesh. Health Policy and Planning 10(3): 304–311.
-
Centers for Disease Control and Prevention (CDC) (2022) Causes and how tetanus spreads.
-
Cholera (2022) World Health Organization.
-
Esposito S, Durando P, Bosis S, Ansaldi F, Tagliabue C, et al. (2014) Vaccine-preventable diseases: From paediatric to adult targets. European Journal of Internal Medicine 25(3): 203-212.
-
Haemophilus influenzae Disease (including Hib) (2022) Centers for Disease Control and Prevention.
-
Hepatitis (2022) World Health Organization.
-
Hepatitis A Vaccines Market: Rise in number of hepatitis A cases to drive the market (2022) _BioSpace_.
-
How Do Vaccines Work? (2022) Centers for Disease Control and Prevention.
-
Jamil K, Bhuiya A, Streatfield K (1999) Expanded Programme on Immunization in Bangladesh: Achievements and challenges. Journal of Health, Population and Nutrition 17(3): 211-218.
-
Organization WH, Organization UNC (1995) Expanded Programme on Immunization (EPI) in Bangladesh: Progress and challenges. Geneva: World Health Organization.
-
JL Pimentel, JL Pimentel (2019) Some Biases in Likert Scaling Usage and Its Correction. International Journal of Sciences: Basic and Applied Research (IJSBAR).
-
Talukder K, Islam M, Chowdhury A (1991) Immunization coverage and inequalities in Bangladesh. Bangladesh Medical Research Council Bulletin 17(2): 45-50.
-
Andre FE, Booy R, Bock HL, Clemens J, Datta SK, et al. (2008) Vaccination greatly reduces disease, disability, death, and inequity worldwide. Bulletin of the World Health Organization 86(2): 140–146.
-
Anichini G, Cusi MG (2022) Immune response analysis to measles virus in subjects vaccinated with MMR vaccine and naturally infected subjects. Gabriele Anichini PhD Thesis.
-
Awadh AI, Hassali MA, Al-Lela OQ, Bux SH, Elkalmi RM, et al. (2014) Immunization knowledge and practice among Malaysian parents: A questionnaire development and pilot-testing. BMC Public Health 14: 1107.
-
Bhuiya A, Bhuiya I, Chowdhury M (1995) Factors affecting acceptance of immunization among children in rural Bangladesh. Health Policy and Planning 10(3): 304–311.
-
World Health Organization (2021) Immunization Agenda 2030: A global strategy to leave no one behind.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria
- Evidence of Spatial Clustering Distribution Patterns of Malaria in Epe, Lagos, Nigeria