Prevention of Mother-to-Child Transmission Coverage among HIV Positive Pregnant Women Accessing Antenatal Services in Ondo State, Nigeria
Background: As PMTCT services are being decentralized to primary health centres, it becomes important to understand the disposition of clients at this level to effective coverage and service utilization of its intervention. However despite concerted efforts to scale-up PMTCT interventions in Nigeria, the coverage and uptake of the service by pregnant women remain low. Objective: To determine factors influencing utilization of PMTCT intervention by HIV positive pregnant women assessing ANC services in selected Comprehensive Centres in Ondo State, Nigeria. Study Design: Cross-sectional study. Study Area: The study was conducted at the selected Comprehensive Centres, Ondo State Study Population: All consenting HIV positive pregnant women who attended the antenatal clinic within the four months (Oct.,2019-Jan.,2020) period of the research Methodology: The data was collected using a structured questionnaire through direct interview of the participants. Results: A total of three hundred and eighty-five (385) HIV-positive pregnant women were recruited in the study at the Antenatal clinic in eight (8) selected Comprehensive Centres in Ondo State. PMTCT service utilization among HIV-positive pregnant women revealed strong association with two independent variables in this study; spouse/partner permission to uptake HCT (OR=3.7, CI=2.3-6.1, p=0.00), disclosure of result to spouse (OR=1.5, CI=0.9-2.3, p=0.00). Predictor of PMTCT intervention in this study was evident among those who practice religion. Women who practice Islamic as a religion recorded lower chances of utilizing the services compare to the Christian. Conclusion: Evidence from this study suggests two significant findings. First is that infants to be born to HIV-positive mothers are more likely to become HIV-positive if they have a mother who has failed to disclose her HIV-positive status, and second is that the socio-demographic profile of the study suggests an important relationship between women taking permission from the spouse to uptake HCT and disclosure of HCT results to their spouse. The success of PMTCT of HIV depends on identifying and integrating effective methods through ANC to address safe disclosure, closing gaps in geographical coverage, accessing and utilization of the services.
Introduction
Overtime, the health sector response to HIV/AIDS, prevention, treatment, care and support interventions have continued to expand guided by policies, strategic plans and guidelines [1]. Free HIV counselling and testing as well as Anti-retroviral therapy (ART) is also expanding with improved resource mobilisation and coordination [1]. Despite interventions, there is still a huge gap towards attaining the universal access [2]. This gap needs to be addressed because patients’ satisfaction with health care is an important health outcome which has implications for capacity utilisation. To enhance the utilization of the health services by people, it is most important that they should recognize the need for such services. This need will only be felt if they start to value health as a worthwhile asset [1].
Primary health care, which is supposed to be the bedrock of the country’s health care policy, is currently catering for less than 20% of the potential patients [3]. Although PHC was said to have made much progress in the 1980s, its goal of 90% coverage was probably excessively ambitious, especially in view of the economic strains of structural adjustment that permeated the Nigerian economy throughout the late 1980s [4].
ANC provides avenue to provide pregnant women with information, treat existing social and medical conditions and screen for risk factors. However it is not enough to receive ANC, since majority of the fatal complications occur during or shortly after delivery [5].
Pregnant women susceptibility to HIV and its consequent transmission to the foetus provide a unique opportunity for implementing preventive strategies against HIV infections of the new born babies. Most infant HIV infections could be averted if positive mothers have a high degree of awareness and knowledge about MTCT and the preventive strategies put in place to reduce the transmission during pregnancy and lactation [6].
PMTCT coverage is low in Nigeria despite being one of the countries with the highest burdens. Nigeria alone contributes 30% to the PMTCT gap - the difference between estimated number of HIV-positive pregnant women and those reached with antiretroviral prophylaxis for PMTCT [6]. The coverage of antenatal screening for HIV is 13% (UNICEF, 2010), a far cry from the UNGASS and national targets [7]. This low coverage is not unconnected with the concentration of services in secondary and tertiary level facilities which make up only 12.7% of health facilities offering maternity services in the country and provides access for a limited number of pregnant women [6, 7].
The target of c (PMTCT) is to stop children from being infected during pregnancy, labour or breastfeeding [8]. To achieve this, there is need for accessibility to take up a cascade of interventions like antenatal service, HIV counselling and testing (HCT) during pregnancy was positioned as a key strategy. In recognition of the lopsided distribution of PMTCT services and its resultant effect on coverage, the Government of Nigeria in 2010, started making plans to expand services to PHCs [4]. The commitment of the global community to accelerate the progression of preventing mother to child transmission of HIV virus further justifies the reason why no stone should be left unturned into research areas that will help to achieve such goals [9].
In Nigeria, effective PMTCT programmes is available free of charge and require by all HIV positive pregnant women to take up a cascade of interventions including antenatal services and HIV testing during pregnancy; use of antiretroviral treatment (ART) by pregnant women living with HIV; safe childbirth practices and appropriate infant feeding; uptake of infant HIV testing and other post-natal healthcare services [10].
Lack of adequate knowledge of mother to child transmission (MTCT) will continue to constitute a fundamental reason why mother to child transmission of HIV will be on the increase in our society [11, 12]. Utilization of health facilities are determined by many factors; maternal age, parity, income, standard of living of household, ANC user’s fees, and travel distance to antenatal care provider are common economic factors that have been cited by previous researchers [13].
According to study carried out in the Oromia region of Ethiopia, showed that challenges of the PMTCT program included human resource limitations, inadequate coordination between regional and local health services concerning new policies and guidelines, irregular supplies of laboratory test kits, stigmatization, inadequate counselling, Cultural barriers and ARVs [14, 15].
However despite concerted efforts to scale-up PMTCT services in Nigeria, the coverage and utilization of the service by pregnant women remain low and unevenly distributed. In spite of this, only a limited number of pregnant women actually use these services. The researcher is curious to find out why there was low PMTCT Utilisation despite government’s effort to increase access, factors influencing utilisation and possible interventions to increase access. This study was therefore designed to explore the factors affecting utilization of PMTCT intervention among HIV positive pregnant women attending ANCs at Comprehensive Health centres.
Methodology
Study Design
It was a health facility- based descriptive cross sectional study which was carried out to determine the utilization and the factors affecting the uptake of mother-to-child transmission of HIV among pregnant women. The study sample included 8 comprehensive health centres in the LGAs which were selected by simple random sampling using a table of random numbers. These facilities are involved in HIV screening and provision of prevention of mother-to-child- transmission services. The study population included only pregnant women attending the antenatal booking clinic (first ANC visit in current pregnancy) at the facilities over a period of four month (Oct., 2019 and Jan., 2020).
Sampling Technique
The sample size was calculated using the formula: N= z2pq/d2 where: z=Standard normal deviate set at 1.96 p=prevalence of PMTCT utilization was taking as 35%. d=A confidence level of 95% was used with a tolerance margin set at 5%. N= (1.96)2X 0.35X0.65 (0.05)2 N= 350, Adjusting for 10% NR (Non-response rate) 10/100 X 349.58 = 34.958 Therefore, N = 349.58+34.958 N= 384.538 N= 385.
A systematic sampling technique was used to select the 385 pregnant women who participated in the study by using multistage stratified sampling method.
A multistage sampling was used after compiling the sample frame. This approach was appropriate for this study because each person has equal chance of being selected for the sample.
Sample size were allocated to each selected health centre based on the estimated number of ANC attendees for the previous four months, since the researcher could not get the estimate of PMTCT clinic attendee’s due to uncoordinated referral services. Participants were randomly selected from the list of those attending PMTCT clinic on the day of visitation. They were administered questionnaire to fill from selected centres in the ratio of 75:25 for urban and rural dwellers, respectively. This ratio was arrived at based on the last National Demographic Health survey conducted in 2008, where ANC is received more by urban women (84%) than rural women (45%) [16]. The study was explained to each selected patient and only those who gave a verbal consent were recruited into the study.
Data Collection
Data was collected using interviewer administered questionnaire by research assistants who had a day training on the research tool. The questions were adapted partly from the Nigeria Demographic Health Survey 2013 and from the study of Hailu M, et al. [17] who did a similar study in Sebeta Town, Central Ethiopia [17, 18]. The questions consisted of mainly close-ended questions but also had some open-ended questions addressing the respondents socio-demographic characteristics (age, marital status, tribe, religion, occupation, educational status); the occupation of the partners and their HIV testing status; reproductive history, knowledge on mother-to-child-transmission of HIV, Utilization and experience of PMTCT services (if they accept to be tested for HIV, if they received PMTCT services, satisfaction with the PMTCT services, partners HIV status and their reasons for accepting screening), information on the barriers to the uptake of PMTCT services were all obtained.
Data Management
Data obtained was entered using SPSS Windows 20 by inputting all the variables this was carefully checked to ensure all variables had been entered before the analysis. For the descriptive aspects of the analysis, frequency distributions were generated for all categorical variables. Means and standard deviations were determined for quantitative variables.
The Chi-squared test was applied for the comparison of proportions. Binary logistic regression was performed to identify socio-demographic factors independently associated with dependent variable. Strength of association between knowledge score and willingness to test was examined by measuring odd ratio, 95% confidence intervals and applying the T-test with level of significance set at 5% (p<0.05) was considered statistically significant.
Measures
The main outcome variable in this study was PMTCT service utilization. It was measured by participants who responded to having been counselled, offered voluntary HIV testing and took the HIV test.
Composite knowledge scores were computed for PMTCT services and HIV-related knowledge responses to the five knowledge related questions on HIV/MTCT, correct responses were given a value of “1” and incorrect responses given “2.” The sum and mean were computed. These scores were then summed up and divided by the total number of test items to arrive at an average knowledge score per person. A respondent who scored equal to or above the mean was considered as having good knowledge or otherwise they were labelled as having poor knowledge.
Knowledge about PMTCT coverage/utilization was measured by the participants’ responses by scoring 1 for correct answer and 2 for an incorrect answer. These scores were then summed up and divided by the total number of test items to arrive at an average utilization score per person. A respondent who scored equal to or above the mean was considered as good user or otherwise they were labelled as having poor user.
Ethical Consideration
Ethical approval was obtained from the State Ministry of Health, Akure Ethics Committee. Written informed consent was obtained from each study participant after reading the consent form which contained information about what the study was all about and the benefit to the participants. The purpose of the study and the rights of the participant to withdraw at any time was discussed prior to the interview. The questionnaire did not bear any name of the participant and confidentiality of the information obtained was ensured throughout the interview.
Results
Socio-Demographic Characteristics of the Respondents
The socio-demographic characteristics of the data showed that 385 respondents were interviewed and majority, (79.3%) were within the age group of 21 – 40 years with a mean age of 17.6 years ± 3.5 standard deviation. 183 (47.5%) and 140 (36.4%) respondents had tertiary and secondary education as the highest level of education respectively, and 42 (10.9%) had primary education. Most of the women (43.4%) and their partners (61.8) were self- employed, married (85.2%), they were mostly Yoruba ethnicity (81.2%) and most of them practiced Christianity as a religion (74.8%) (Table 1).
| Frequency (n) | Percentage (%) | |
|---|---|---|
| Age of the respondent | ||
| ≤ 20 | 24 | 6.2 |
| 21-30 | 160 | 41.6 |
| 31-40 | 145 | 37.7 |
| > 40 | 56 | 14.5 |
| Marital Status Christianity | ||
| Single | 44 | 11.4 |
| Married | 328 | 85.2 |
| Divorced | 6 | 1.6 |
| Widowed | 4 | 1 |
| Separated | 3 | 0.8 |
| Religion | ||
| Islam | 97 | 25.2 |
| Christian | 288 | 74.8 |
| Ethnic Group | ||
| Yoruba | 315 | 81.8 |
| Apoi-Ijaw | 20 | 5.2 |
| Hausa | 19 | 4.9 |
| Ibo | 31 | 8.1 |
| Educational Status | ||
| No formal Education | 20 | 5.2 |
| Primary Education | 42 | 10.9 |
| Secondary Education | 140 | 36.4 |
| Tertiary Education | 183 | 47.5 |
| Occupational status | ||
| House wife | 58 | 15.1 |
| Government employee | 88 | 22.9 |
| Farmer | 25 | 6.5 |
| Self employed | 167 | 43.4 |
| Petty trader | 47 | 12.2 |
| Number of alive children (if any) | ||
| 113 | 29.4 | |
| 01-Feb | 262 | 68.1 |
| 03-Apr | 1 | 0.3 |
| 05-Jun | 9 | 2.3 |
| Husband’s Occupation | 74 | 19.2 |
| Government employee | 74 | 19.2 |
| Private employee | 73 | 19 |
| Self employed | 238 | 61.8 |
Table 1: Socio-demographic characteristics of respondents (n = 385).
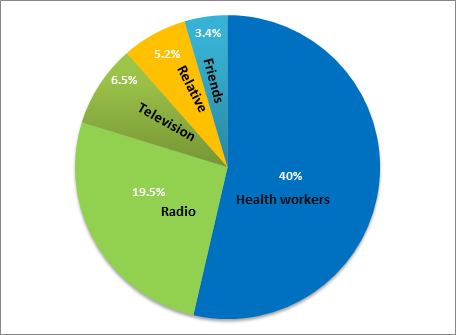
On the knowledge of respondents about MTCT/PMTCT as shown in Table 2, majority of the respondents 260 (67.5%) have heard about PMTCT and its intervention. Most of the respondents had good knowledge of mode of transmission of HIV from mother-to-child during delivery (75.1%), during breastfeeding (73.2%) and during pregnancy (71.7%) from an infected mother respectively; with the main source of information being the health workers (40.0%). This is shown in figure 1.
| Frequency(n) | Percentage(%) | |
|---|---|---|
| Have you heard of PMTCT before | ||
| Yes | 260 | 67.5 |
| No | 125 | 32.5 |
| Can HIV be transmitted from Mother to Baby during pregnancy | ||
| Yes | 276 | 71.7 |
| No | 55 | 14.3 |
| Don’t know | 54 | 14 |
| Can HIV be transmitted from Mother to Baby during delivery | ||
| Yes | 289 | 75.1 |
| No | 33 | 8.6 |
| Don’t know | 63 | 16.4 |
| Can HIV be transmitted from Mother to Baby during breastfeeding | ||
| Yes | 282 | 73.2 |
| No | 38 | 9.9 |
| Don’t know | 65 | 16.9 |
Table 2: Knowledge of MTCT and PMTCT of HIV among the respondents.
- Can HIV Pregnant woman still look healthy
- Yes
- 315
- 81.8
- No
- 22
- 5.7
- Don’t know
- 48
- 12.5
- Do you think that every pregnant woman should be screened for HIV
- Yes
- *326
- 84.7
- No
- 16
- 4.2
- Don’t know
- 43
- 11.2
Table 3: Knowledge of MTCT and PMTCT of HIV among the respondents.
After scoring of outcome variables, 72.2%, 67.5% and 60.3% of the respondents had knowledge scores up to and above the group’s average score for MTCT related knowledge, PMTCT Knowledge and PMTCT coverage/utilization respectively (Table 3).
| HIV/AIDS/MTCT RELATED KNOWLEDGE | |
|---|---|
| Variable | Values |
| Knowledge score | |
| Mean(Average) | 11.1 |
| Standard deviation | 10.5 |
| Categorized knowledge scores (%) | |
| Average and above | 72.2 |
| Below average | 27.8 |
| PMTCT KNOWLEDGE | |
| Knowledge score | |
| Mean(Average) | 1.3 |
| Standard deviation | 0.5 |
| Categorized knowledge scores (%) | |
| Average and above | 67.5 |
| Below average | 32.5 |
Table 4: PMTCT Knowledge and Utilization scores (n=385).
| PMTCT COVERAGE/UTILIZATION | |
| User score | |
| Mean(Average) | 13.1 |
| Standard deviation | 1.7 |
| Categorized user scores (%) | |
| Average and above | 60.3 |
| Below average | 39.7 |
Table 5: PMTCT Knowledge and Utilization scores (n=385).
Utilization of PMTCT Services among the Respondents and their Partners/Relatives
The PMTCT experience of respondents was also assessed given that this experience would impact on their ability to utilise the available PMTCT services. This is a health facility based study and the respondents were those that are just registering at the day of data collection. These experiences include: type of HCT received, disclosure of result to spouse and relatives, follow-up counselling received and willingness to continue with the services.
Of the one hundred and ninety-seven, 197(51.2%) mothers reported being tested, 169(43.9%) and 64 (16.6%) reported to uptake the pre-test and post-test counselled respectively. When respondent were asked whether they need permission from their spouse/partner to do HCT. Majority of the respondents 72.7% (n = 280) responded No while 27.3% (n = 105) responded Yes (Table 4).
| Status | Frequency (%) | |
|---|---|---|
| Types of HCT received | Pre-test counselling | 169(43.9) |
| Types of HCT received | HIV testing | 197(51.2) |
| Types of HCT received | Post-test counselling | 64(16.6) |
| Types of HCT received | Referral for care and support | 27(7.0) |
| Do you need permission from your spouse/partner to do HCT | Yes | 105(27.3) |
| Do you need permission from your spouse/partner to do HCT | No | 280(72.7) |
| Did you disclose your result to your spouse and relative | Yes | 167(43.4) |
| Did you disclose your result to your spouse and relative | No | 218(56.6) |
| Reasons for non-disclosure | Afraid of been abandoned/divorced | 64(16.6) |
| Reasons for non-disclosure | Physically violated/abused | 92(23.9) |
| Reasons for non-disclosure | Separated from the children | 31(8.1) |
| Reasons for non-disclosure | Thrown out of home | 61(15.8) |
| Which type of pretest counselling did you receive | Group counselling. | 68 (17.7) |
| Which type of pretest counselling did you receive | One-on-one. | 317 (82.3) |
| Which type of posttest counselling did you receive | Group counselling | 58(15.1) |
| Which type of posttest counselling did you receive | Individual counselling | 327(84.9) |
| Was follow up counselling done | Yes | 237(61.6) |
| Was follow up counselling done | No | 148(38.4) |
| Was couple counselling done | Yes | 302(78.4) |
| Was couple counselling done | No | 83(21.6) |
| If No why | Scared of disclosing to partners | 24(6.2) |
| If No why | Partners refused to come | 15(3.9) |
| If No why | We were not encourage to do so | 22(5.7) |
| If No why | It was not necessary | 53(13.8) |
| Before commencing PMTCT was adherence counselling done | Yes | 260(67.5) |
| Before commencing PMTCT was adherence counselling done | No | 125(32.5) |
| Reasons for non-adherence | Afraid of Stigmatization | 47(12.2) |
| Reasons for non-adherence | Scared of people seeing me with the drug | 27(7.0) |
| Reasons for non-adherence | Don’t like the drug | 20(5.2) |
| Reasons for non-adherence | So busy to remember timing | 9(2.3) |
| Willingness to continue with PMTCT service | Yes | 48(12.5) |
| Willingness to continue with PMTCT service | No | 326(84.7) |
| Willingness to continue with PMTCT service | Don’t know | 11(2.9) |
| Were your drugs readily available each time you need it: | Yes | 298(77.4) |
| Were your drugs readily available each time you need it: | No | 87(22.6) |
| Far distance to health facility | Yes | 227(59.0) |
| Far distance to health facility | No | 158(41.0) |
| Does the attitude of health workers discourage you to continue accessing PMTCT Services | Yes | 78(20.3) |
| Does the attitude of health workers discourage you to continue accessing PMTCT Services | No | 264(68.6) |
| Does the attitude of health workers discourage you to continue accessing PMTCT Services | Don’t know | 43(11.1) |
| If yes, what are the attitudes? | Verbal Abuse. | 41(10.6) |
| If yes, what are the attitudes? | Confidentiality not ensured. | 8(2.1) |
| If yes, what are the attitudes? | Stigmatization/discrimination. | 17(4.4) |
| If yes, what are the attitudes? | Long waiting time for ANC. | 12(3.1) |
| If yes, what are the attitudes? | Cost. | 2(0.5) |
| If yes, what are the attitudes? | Unfriendliness/Aggressiveness | 1(0.3) |
Table 6: Utilization of PMTCT Services among the respondents.
Following HCT, respondents were asked if they disclosed their HIV result to their spouse/relative. Majority of the respondents 56.6% (n=218) did not reveal their HIV status to their partners/relatives while 43.4% (n=167) of them did, and reasons for non-disclosure of result to partners/ relatives include; physically violated/abused (23.9%), afraid of been abandoned/divorced (16.6%), will be thrown out home (15.8%), and separate from the children (8.1%) When asked about the type of pre-test counselling received. Majority of the respondents 82.3% (n= 317) received 0ne-on-one counselling, 17.7% (n = 68) received group counselling. Majority of the respondents 84.9% (n = 327) received individual counselling, 15.1% (n = 58) received group counselling. Follow – up counselling is an important aspect of counselling that helps consolidate all the previous counselling received in the course of hospital visits. More than half 61.6% (n = 237) of the respondents received follow-up counselling, 38.4% (n = 148) did not receive. This is a necessity as some naive mothers might change their mind after such post-test counselling; hence follow up counselling helps to internalize the importance of PMTCT services to them The number of couple counselling done were 78.4% (n=302) while some respondents 21.6% (n=83) did not receive any couple counselling. The main reasons given by the 83 respondents who did not do couple counselling were that it was not necessary (13.8%), they were scared of disclosing their status to their partners(6.2%), we were not encourage to do so (5.7%) and Partners refused to come (3.9%).
Adherence counselling is important because failure to comply with medication can lead to resistance and treatment failure. Once a patient’s test is reactive, adherence counselling is done before commencement of therapy. The respondents were asked whether they were compliant to therapy, 67.5% (n= 260) respondents answered Yes while 32.5% (n= 125) said No. The main reasons given by the 32.5% non-complaints respondents were; afraid of stigmatization (12.2%), Scared of people seeing me with the drug (7.0%), Do not like the drugs (5.2%) and so busy to remember timing (2.3%) Attitude of health workers did not really discourage respondents from continuing access to PMTCT services as attested to by 68.6% (n=264) of the respondents. Only 20.3% (n=78) of the respondents responded that health workers attitude will affect their continued access of the services based on the following reasons; verbal abuse (10.6%), stigmatization/discrimination (4.4%), Long waiting time for ANC (3.1%), confidentiality not ensured (2.1%), cost (0.5%) and unfriendliness/aggressiveness (0.3%) as shown in table 4.
Socio-Demographic Characteristics Predicting Utilization of PMTCT Services
Using binary logistic regression, the respondents who practiced Christianity as a religion were 3.7 times more likely to utilize the service more than those who practiced Islamic as a religion{OR=3.7(95% CI: 2.3-6.1)} P=0.00, this was statistically significant as shown in Table 5. Also women who failed to disclose their HIV-positive status to their spouse/ partners/relatives were 1.5 times more likely to utilize the service more among those who practiced Christianity compared to Islamic religions {OR=1.5(95% CI: 0.9-2.3)} P=0.01, this was statistically significant as shown in table 5.
| Predictors | Spouse permission for HCT uptake | Disclosure of HCT result to spouse | ||
|---|---|---|---|---|
| OR(95%CI) | P-Value | OR(95%CI) | P-Value | |
| Age of the respondent | 0 | 0.84 | ||
| ≤ 20 | ||||
| *21-30 | ||||
| 31- 40 | ||||
| > 40 | ||||
| Marital Status | 0.03 | 0.14 | ||
| Single | ||||
| *Married | ||||
| Divorced | ||||
| Widowed | ||||
| Separated | ||||
| Religion | 3.7(2.3-6.1) | 0 | 1.5(0.9-2.3) | 0.01 |
| Islam | ||||
| *Christian | ||||
| Ethnic Group | 0.06 | 0.8 | ||
| *Yoruba | ||||
| Apoi-Ijaw | ||||
| Hausa | ||||
| Ibo | ||||
| Educational Status | 0.01 | 0.24 | ||
| No formal Education | ||||
| Primary Education | ||||
| Secondary Education | ||||
| *Tertiary Education | ||||
| Occupational status | 0 | 0.14 | ||
| House wife | ||||
| Government employee | ||||
| Farmer | ||||
| *Self employed | ||||
| Petty trader | ||||
| Number of alive children (if any) | 0 | 0.41 | ||
| *1-2 | ||||
| 03-Apr | ||||
| 05-Jun | ||||
| Husband’s Occupation | 0.22 | 0.82 | ||
| Government employee | ||||
| Private employee | ||||
| *Self employed |
Table 7: Predictive factors of assessing PMTCT utilization for permission from spouse to do HCT and disclosure of the result to s
*reference category used for the categorical variables, *Significant values at P<0.05 and 95% Confidence Interval Table 5: Predictive factors of assessing PMTCT utilization for permission from spouse to do HCT and disclosure of the result to spouse.
Discussion
There are nearly 1.72 million women and girls living with HIV in Nigeria and the prevalence continues to increase despite efforts by the Nigerian Ministry of Health [19]. Furthermore, 60,000 new HIV infections occurred among children, making Nigeria the country with the largest number of children acquiring HIV through mother-to- child transmission of HIV (MTCT) [20]. Although PMTCT interventions can be highly successful in reducing the risk of HIV transmission, access to and utilization of PMTCT services is still limited in many parts of sub-Saharan Africa owing to a variety of factors that facilitate or hinder PMTCT service uptake in Nigeria by extension in Ondo State.
If the national targets of ensuring that at least 90% of all pregnant women have access to voluntary counselling and testing, 80% of all HIV-exposed infants have access to early infant diagnosis services, 80% of all HIV-positive pregnant women and HIV-exposed infants have access to efficacious ARV’s and 80% of HIV-positive pregnant women have access to infant feeding counselling are to be met by 2015 [21].
The study was designed to investigate why pregnant women do not use PHCs for PMTCT services in some urban parts of Ondo State in Southern Nigeria. We based the study on the premise that PHCs offer the best opportunity for women in Nigeria to enter the health care system to receive the most optimal evidence-based access to skilled delivery care [22, 23].
The socio-demographic profile of the women showed that majority of the respondents were under 34 years old with the highest age range being 21-40 (79.3%; n=305); this is in line with the finding by Nnamdi Okagbue (2009) in a different study conducted in Anambra State of Nigeria where the highest age range were 25-29 years old accounted for 36.3% of the respondents [24]. This shows that less than 34 years is still a high risk age group according to this study and it means that this age group should be the target for campaigns against unsafe sex, the most common source of contracting HIV in Nigeria. Early marriage is predominant especially in the rural setting where they do not have the opportunity to attend higher education. Thus it is important that HIV/AIDS awareness should be directed to higher institutions (universities and polytechnics) where these age groups are found.
Of all the respondents, 85.2% (n=328) were married, this signifies that marriage is a factor especially where pre- marital HCT is not considered a priority. This is in keeping with Olanrewaju AM, et al. [25] where they find marital status (>80%) significantly associated with HIV status. This result is not out of place in an environment where pregnancy outside marriage is not acceptable. Still HIV testing before marriage should be encouraged so that those willing not to get pregnant upon knowing there status can have access to family planning method of their choice.
Of the respondents, 83.9% (n=323) had achieved secondary and tertiary education, this collaborates with the 2010 ANC sentinel survey (FMOH 2010) where 34% of the women had secondary education, closely followed by primary education (22.4%) with only 19% having higher education [26]. Katushabe J [27] reveals that majority of the respondents were within the range of higher primary and ordinary Level. Some 43.4% (n=167) were self-employed, 22.9% (n=88), house wife 15.1% (n=58) and trader, 12.2% (n=47).Though majority of the respondents had secondary and tertiary education, only few (43.4%) are in one form of employment or another. This supports Nnamdi Okagbue where 31.4% were housewives, while 19.6% were either students or unemployed 25% were traders, and 23.5% were in permanent employment Shangula MN [28] in his study reveals that majority of the mothers are unemployed (80%) with only 20% employed.
In the study 84.7% among pregnant women screened for HIV were aware MTCT was possible through breastfeeding by lactating mothers, during delivery and pregnancy while 77.4% were aware that the risk of MTCT can be reduced through the use of readily available drug(anti-retroviral), this in keeping with Asefa A, et al. [29] reveals that only 60.7% of all interviewed pregnant women who were aware of HIV/AIDS transmission knew about the risk of MTCT [29]. The possibility of MTCT during pregnancy, delivery and breastfeeding was known by 48.4%, 58.6% and 40.7% of the respondents, respectively.
Third-fifths of the respondents heard about HIV/AIDS from either the health workers or the radio, with others source of information less than 10% about HIV/AIDS. The two most important sources of information about HIV/ AIDS in this research were through health workers and radio. This is related to the outcome of a 2006 study which reported electronic media as the main source of information on HIV/AIDS [30]. This is lesser than the study conducted by Artwinne et al in Uganda where information regarding HIV and PMTCT was 69.66% from health workers, 32.58% from the mass media and 9% from schools [31]. Exposure to mass media was generated with frequency of listening to radio, watching television and health care workers were identified as key sources of information regarding HIV and PMTCT.
After scoring of outcome variables for knowledge about HIV/AIDS/MTCT, PMTCT and PMTCT utilization, more than half of respondents, 72.2%, 67.5% and 60.3% respectively had good comprehensive knowledge about HIV/AIDS/MTCT, PMTCT and PMTCT utilization. This is much higher than the reported regional (South-west) and national values of 26.5% and 23.4% respectively for women of reproductive age [32]. The present study, therefore, lends credence to previous evidence showing better ANC/PMTCT utilization in South- West region in the country [33, 34]. Also, the percentage average score of 72.2%, which translated to average knowledge about HIV/AIDS, varies from the 2012 Indian research that reported 63.2% having good knowledge score [35]. This may not be unconnected with the high literacy level of the respondents with about 83.9% of mothers in our study having post primary school education. Thus, Education is the key to mother’s survival and enables a woman to know what to do in determining illness, health condition and making child bearing safer.
Concerning taking permission from spouse before doing HCT, 27.3% (n=105) of the respondent stated that they need permission while 72.7% (n = 280) responded they do not. This contradicts Okonkwo KC, et al. [35] where 82.9% responded they did not need permission to undergo testing while 17.1% answered they did needed permission.35 Our result is consistent with Nnamdi-Okagbue findings that showed only 33% of respondents’ needed husband permission while 65% does not need husband’s permission.24 Culture can influence access through inherent inequalities in the social system. Gender also affects access, pushing women into gender specific roles that negatively influence their health or force to seek permission to obtain healthcare. This shows the dominance of men over their spouses. This is where couple counselling plays a vital role in uniting the family.
On the issue of disclosure, 43.4% (n = 167) disclosed their result while 56.6% (n = 218) did not. Many were of afraid of abandonment or divorced and some were afraid of being separated from their children and thrown out of home. This can be related to the previous question on permission. The situation can degenerate to physically violated or abused in the family especially for discordant couples where accusations and counter-accusations will manifest. Also 74.8% of women that practise Christian religion disclosed their results to their spouse. This contradicts Okonkwo KC, et al. [35] where 69.2% of their respondents responded that they would be discriminated against socially and/or culturally if they tested HIV positive. According to Talam NC, et al. [36], they identified stigma (28.9%) as one of the factors affecting adherence to treatment with ARVs [36]. According to health service utilisation, stigma, fear and disclosure are some of the identified socio-economic factors influencing PMTCT utilisation.
The socio-demographic variables found to be significantly associated with utilization of PMTCT services were the practiced religions of the women for spouse permission to uptake HCT (OR 3.7, 95% CI: 2.3-6.1, P=0.00) and for disclosure of result to their partners (OR 1.5, 95% CI: 0.9-2.3, P=0.01) which is different from the study of Okonofua NL, et al. [37] in Nigeria.
Also Dairo MD, et al. [38] conducted a study in Ibadan Nigeria to determine the factors affecting the utilization of ANC/PMTCT services in Ibadan, Nigeria. Women who were Muslims or other religions were more than 2 times likely to attend ANC clinic than women who were Christians [(OR=2.398, 95%CI, 1.264-4.557) [38]. The variations might be due to the difference in methodologies. Effort towards ensuring the utilization of PMTCT should be targeted towards ANC, the importance of maternal care should be emphasized even in the religious settings among reproductive age.
Conclusion
Evidence from this study suggests two significant findings. First is that infants to be born to HIV-positive mothers are more likely to become HIV-positive if they have a mother who has failed to disclose her HIV-positive status, and second is that the socio-demographic profile of the study suggests an important relationship between women taking permission from the spouse to uptake HCT and disclosure of HCT results to their spouse. It was revealed that religion is the predictor of accessing and utilizing PMTCT intervention in this study. Women who practice Islamic as a religion recorded lower chances of utilizing the services. The positive influence on utilization of health service acceptability may be responsible for higher utilization of PMTCT intervention among those who practice Christianity as a religion. Given the important role played by socio-economic factors in PMTCT, stakeholders need to re-examine policies on disclosure and male partner involvement with a view to addressing behavioural contributors to MTCT. The success of PMTCT of HIV depends on identifying and integrating effective methods through ANC to address safe disclosure, closing gaps in geographical coverage, accessing and utilization of the services. Efforts devoted toward addressing these factors can be achieved using innovative approaches like increasing pregnancy care services and PMTCT utilization in PHCs to reduce child transmission and maternal mortality.
References
-
Oxford Medical Publications (1983) Practising health for all. pp: 319-26.
-
Universal Access: Background, Global Commitment and Strategic Framework UNAIDS (2010) presentation at 5th National Conference on HIV & AIDS Abuja.
-
Gupta MD, Gauri V, Khemani S (2004) Decentralised Delivery of Primary Health Services in Nigeria: Survey Evidence from the States of Lagos and Kogi. Washington: The World Bank, pp: 86.
-
Joint United Nations Program (2012) on HIV/AIDS, Nigeria. HIV/AIDS Estimates.
-
Safe Motherhood Inter Agency Group (IAG) (2002) Fact Sheet: The Safe Motherhood Initiative. Family Care International (FCI).
-
UNICEF (2010) Nigeria PMTCT Factsheet.
-
World Health Organisation (2009) Global picture of PMTCT gap, Towards Universal Access Progress Report.
-
Ghana AIDS Commission (2010) Prevention on of M other to Child Transmission on of HIV in Ghana: Scale-up Plan.
-
WHO (2008) List of indicators proportion of births occurring in rural and urban areas. National Demographic Health Survey.
-
Padian NS, McCoy SI, Karim SA, Hasen N, Kim J, et al. (2011) HIV prevention transformed: the new prevention research agenda. Lancet. 378(9787): 269-278.
-
United Nations (2010) Integrated and coordinated implementations of and follow up to the outcome of major United Nations Conferences and Summits in the economic.
-
UNAIDS (2011) Joint United Nations Programme on HIV/AIDS, World AIDS Day Report.
-
Mekonnen Y, Asnaketch M (2002) Utilization of Maternal Health Care Services in Ethiopia. USA: ORC Macro pp: 24.
-
Federal Ministry of Health of Ethiopia (2012) Country progress report on HIV/AIDS response. pp: 70.
-
Balcha TT, Lecerof SS, Jeppsson AR (2011) Strategic challenges of PMTCT program implementation in Ethiopia. Journal of the International Association of Physicians in AIDS Care 10(3): 187-192.
-
Federal Government of Nigeria (2008) National Demographic and Health Survey Abuja, Nigeria.
-
Hailu M, KifleWolde M, Lamessa D (2016) Utilization of prevention of mother-to-child transmission of HIV services and associated factors among antenatal care attending mothers in Sebeta Town, Central Ethiopia. Advances in Public Health.
-
ICF International Rockville (2013) Nigeria Demographic Health Survey.
-
NACA: National Agency for the Control of AIDS (2011) Update on the HIV/AIDS Epidemic and Response in Abuja, Nigeria.
-
UNAIDS: UBRAF 2012-2015 Country Case Study: Nigeria Geneva.
-
NACA: National Agency for the Control of AIDS (2011) Fact Sheet-PMTCT in Abuja, Nigeria.
-
World Health Organization (1978) Declaration of Alma- Ata: International Conference on Primary Health Care, Alma-Ata.
-
Federal Government of Nigeria (2013) Integrating primary health care governance in Nigeria (PHC under one roof): implementation manual.
-
Nnamdi O, Rosemary U (2009) An Investigation into the factors affecting the utilization of mother to child transmission services by Human Immuno-Deficiency virus Positive women in Onitsha, Anambra State, Nigeria.
-
Olanrewaju AM, Fatusi AO, Akintunde AE, Ibrahim B, Fakunde I (2006) HIV voluntary counselling and testing of pregnant women in primary health care centre in Ilesa, Nigeria. Internet Journal of Third World Medicine 6(1): 29.
-
Federal Ministry of Health (2010) National AIDS/STI Control program Technical Report on National HIV Sero- Prevalence Sentinel Survey.
-
Katushabe J (2007) Knowledge and attitude pregnant women have on use of PMTCT services in Mbale Region, Uganda.
-
Shangula MN (2006) Factors Affecting Voluntary Counselling and HIV Testing among Pregnant Women in Tsumeb district, Oshikoto region, Namibia. An MPH Thesis presented to the University of Western Cape. South Africa.
-
Asefa A, Beyene H (2013) Awareness and knowledge on timing of mother-to-child transmission of HIV among antenatal care attending women in Southern Ethiopia: a cross sectional study. Reprod Health pp: 10-66.
-
Okonta PI, Oseji MI (2006) Relationship between knowledge of HIV/AIDS and sexual behaviour among in-school adolescents in Delta State, Nigeria. Nigerian Journal of Clinical Practice 9(1): 37-38.
-
Artwine BR, Rukundo A, Sebikali JM, Mutibwa D, Tumusiime D, et al. (2012) Knowledge and Practices of Women Regarding PMTCT in Mwizi Sub County 17(3): e211-212.
-
NPC (National Population Commission) [Nigeria] and ICF Macro (2009) Nigeria Demographic and Health Survey Abuja, Nigeria.
-
Babalola BI (2014) Determinants of urban-rural differentials of antenatal care utilization in Nigeria. African Population Studies 28(3).
-
Fagbamigbe AF, Idemudia ES (2017) Wealth and antenatal care utilization in Nigeria: Policy implications. Healthcare for Women International 38(1):17-37.
-
Okonkwo KC, Reich K, Alabi AI, Umeike N, Nachman SA (2007) An evaluation of awareness: Attitudes and beliefs of pregnant Nigerian women toward voluntary counselling and testing for HIV. AIDS Patient Care and STDs 21(4): 252-260.
-
Talam NC, Gatongi P, Rotich J, Kimaiyo S (2008) Factors affecting antiretroviral drug adherence among HIV/AIDS adult patients attending HIV/AIDS Clinic at Moi teaching and referral hospital, Eldoret, Kenya. East African Journal of Public Health 5(2): 74-78.
-
Okonofua Ntoimo L, Ogungbangbe J, Anjorin S, Imongan W, et al. (2018) Predictors of women’s utilization of primary health care for skilled pregnancy care in rural Nigeria. BMC Pregnancy and Childbirth 18(106).
-
Dairo MD, KE Owoyokun (2010) Factors affecting the utilization of antenatal care services in Ibadan, Nigeria. Journal of Postgraduate Medicine 12(1).
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria