SARS-Cov-2 in Families Comparison between Symptomatic and Asymptomatic Secondary Cases: Study of 39 Families and 70 People
Background: The number and characteristics of asymptomatic SARS-CoV-2 infections remains questionable, and their differences are even less understood in the family setting. Objective: To compare in families the characteristics of asymptomatic and symptomatic COVID-19 patients. Methodology: An observational and retrospective study of families in which there was at least two polymerase chain reaction. (PCR) confirmed COVID-19 cases -one primary case or index and one secondary case-, was conducted March 15 to December31, 2020 in a general medicine office, in Toledo (Spain). Socio-demographic and clinical variables were compared between symptomatic vs . asymptomatic secondary cases in the family. Results: 39 families with 132 cohabitants with a primary case of COVID-19 were included. There were 70 secondary cases with positive PCR, 45 symptomatic (64%) and 25 (36%) asymptomatic. The only statistically significant variables in the comparison between symptomatic and asymptomatic secondary cases in the families were that asymptomatic patients were younger, students, presented fewer chronic diseases, and the family was larger. Conclusion: In the context of general medicine in Toledo (Spain), the prevalence of asymptomatic secondary cases is high (36%). Being an asymptomatic versus symptomatic secondary COVID-19 case in the family was associated with being younger, healthier, student, and living in a family with a greater number of members. Young students in large families are a risk group for asymptomatic secondary cases, which may favor the transmission of SARS-CoV-2 in family and extra-family contexts. The focus of testing programs for SARS-CoV-2 should be expanded to include young, healthy, and COVID-19 symptom-free individuals, especially all contacts from large families and in school settings.
Introduction
Since December 2019 to date, more than 98 million reported cases and more than 2 million deaths have been reported from coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [1, 2]. Person-to-person transmission has been established [3, 4, 5, 6, 7], and asymptomatic transmission of SARS-CoV-2 has been reported [8, 9]. Control of spread in particular has been limited by the variable incubation period, presymptomatic transmission (approximately 25-40% of transmission occurs before the onset of symptoms) [10, 11, 12], and a heterogeneous transmission dynamics, in which clusters and superpropagation events play an important role in the spread of the pandemic, although many infections do not lead to subsequent cases [12, 13, 14].
But, the number of asymptomatic SARS-CoV-2 infections remains questionable, and uncertainty remains about how much they have contributed to the pandemic. The range of estimates of asymptomatic SARS-CoV-2 infection reported in studies using a wide variety of designs ranges from 4% to more than 80% [13, 15, 16, 17, 18]. Despite criticism of their different methodologies, these data as a whole are not far from what seroprevalence studies say: a third of patients do not develop symptoms [19]. However, the importance of these asymptomatic infections in the transmission of SARS-Co-2 has been questioned, highlighting the differences between presymptomatic and asymptomatic patients [20, 21]. In this setting, it seems accepted that these asymptomatic (or initially presymptomatic) infections act as a “silent driver” of the pandemic [22]. Also, the asymptomatic infectious case is a “silent client”, one of the most complex and damaging types of “client”: it is someone who does not provide information; of which we have no information [23, 24]. Viral loads have been reported to be similar between asymptomatic (including presymptomatic) and symptomatic patients. Furthermore, viral loads tend to decrease more slowly in asymptomatic patients [25]. Thus, presymptomatic and asymptomatic transmission significantly reduces the effectiveness of control measures that begin with the onset of symptoms, such as isolation and follow-up of contacts [26].
Differences in the magnitude and amplitude of individual adaptive immune responses to SARS-CoV-2, and correlations with patient morbidity, highlight the need to identify factors that predict disease severity. It is unclear why some infected people are asymptomatic while others experience severe COVID-19 symptoms. Our current knowledge of the immune correlates of disease severity is limited by sample size and the diverse study populations of patients. Factors such as gender and age must also be considered. In older people (> 65 years), who are at greatest risk for severe disease, dysregulated adaptive responses are seen more frequently during acute SARS-CoV-2 infection than in younger people. Thus, the possibility of identifying predictive factors would improve with the inclusion of asymptomatic individuals infected with SARS-CoV-2 [27].
On the other hand, most people with COVID-19 receive care at home, which increases the likelihood of exposure for household members. However, less attention has been paid to family members and others who care for people with COVID-19 in the community [28]. The long incubation and high presymptomatic infectivity of COVID-19 make transmission between family members a particular risk. In this sense, modeling of viral shedding suggests that the highest viral load is found at or just before the onset of symptoms, and that 44% of transmission occurs before symptoms [26, 28].
In this context, where the number and characteristics of asymptomatic SARS-CoV-2 infections remain questionable, the relationship between household and non-household contacts remains unclear, and most people with COVID-19 receive care at home (which increases the probability of exposure of family members), a study is presented, which was part of other more general ones [29], and whose objective is to compare in the families the characteristics of secondary cases (after diagnosis of a primary or index case) that were asymptomatic vs. symptomatic COVID-19, based on a retrospective analysis, in a General Medicine office, in Toledo (Spain) from March to November 2020, to assess possible epidemiological differences and their implications.
Material and Methods
An observational and retrospective study of families in which there was at least two polymerase chain reaction (PCR) confirmed COVID-19 cases -one primary case or index and one secondary case-, was conducted March 15 to December 31, 2020 in a general medicine office, in Toledo (Spain). The outcome of interest was to analyze the possible differences in the characteristics of secondary cases (after the diagnosis of a primary or index case) that were asymptomatic vs. symptomatic COVID-19 in families. In part the general methodology has already been published [29].
Diagnosis of COVID-19
The diagnosis was confirmed with PCR oropharyngeal. PCR was performed on all household contacts of the primary case. The cases included confirmed symptomatic cases and asymptomatic carriers. Information on COVID-19 patients and their contacts was obtained from the registry systems used by general medical services in the office.
Household Contacts
Household contacts were defined as people who shared a residence with the COVID-19 index case. We defined family members as those who had lived with primary cases in a house 4 days before and for more than 24 hours after the primary cases developed illness related to COVID-19. Families with secondary transmission were defined as those where some or all of the family members become infected within one incubation period (2 weeks) of symptom onset of the primary case. The onset date of a confirmed case was defined as the date of the first appearance of self-reported clinical symptoms [28]. The onset date for an asymptomatic carrier was defined as the date a positive COVID-19 PCR test was obtained [30]. Contacts were quarantined shortly after the index case was diagnosed, thereby reducing the risk of transmission (a provision not available in all circumstances).
Collected Variables
Data on the index case and close contacts were extracted from the medical records of the general medicine practice under study. The following variables were collected: age; sex; chronic diseases (defined as “any alteration or deviation from normal that has one or more of the following characteristics: is permanent, leaves residual impairment, is caused by a non- reversible pathological alteration, requires special training of the patient for rehabilitation, and/or can be expected to require a long period of control, observation or treatment” [31], classified according to the International Statistical Classification of Diseases and Health-Related Problems, CD- 10 Version: 2019 [32]; social-occupancy class (according to the Registrar General’s classification of occupations and social status code) [33, 34], which were grouped for greater simplicity of the results in workers with or without some type of specialization; problems in the family context and low income household based on the genogram and in the experience of the general practitioner for their continuity of care and knowledge of the family (genogram is a schematic model of the structure and processes of a family, which included the family structure, life cycle and family relational patterns. It was understood that “complex” genograms present families with psychosocial problems) [35, 36, 37, 38]; and severity of the disease (mild cases: clinical symptoms are mild and no manifestation of pneumonia can be found on images; moderate cases: with symptoms such as fever and respiratory tract symptoms, and the manifestation of pneumonia can be seen on the imaging tests; and severe cases: respiratory distress, respiratory rate ≥ 30 breaths/min;
pulse oxygen saturation ≤ 93% with room air at rest; arterial partial pressure of oxygen / oxygen concentration≤300 mmHg) [30]; to simplify comparison, moderate and severe cases were counted together.
Sample
A convenience sampling was used. The families participating in the study were chosen because they had their members in the same consultation and all medical information was available. The families were included in the study in a longitudinal and prospective way as primary and secondary cases were diagnosed in them; but the evaluation was carried out retrospectively in this cohort of families, at the end of data collection.
Sample Size
Sample size was calculated for an unpaired study for a Two-sided Confidence Level (1-alpha) of 95, a Power (% probability of detection) of 80, a Ratio of asymptomatic cases / symptomatic cases of 1: 2, a hypothetical proportion of asymptomatic secondary cases with the presence of chronic diseases of 15%, and a hypothetical proportion of symptomatic secondary cases with the presence of chronic diseases of 50%. Thus total Sample Size (Fleiss) should be 63; 21 asymptomatic secondary cases and 46 symptomatic secondary cases in families [39].
Statistical Analysis
The bivariate comparisons were performed using the Chi Square test (X2), X2 with Yates correction or Fisher Exact Test when necessary, (according to the number the expected cell totals) for percentages, and the Student t test for the mean.
Results
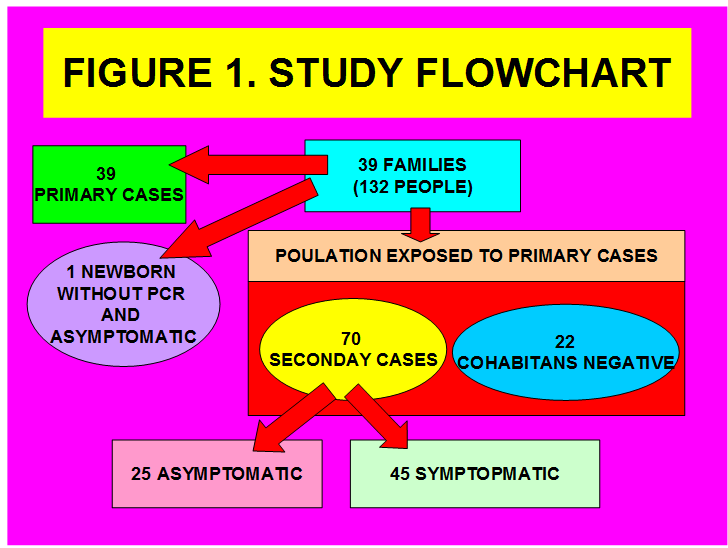
39 families with 132 cohabitants with a primary case of COVID-19 were included, and whose members were treated in the same consultation and all medical information was available. There were 70 secondary cases with positive PCR, 45 symptomatic (64%) and 25 asymptomatic (36%) (Figure 1). The only statistically significant variables in the comparison between symptomatic and asymptomatic secondary cases in families were that asymptomatic patients were younger, students, with fewer chronic diseases, and the family was larger (Tables 1 & 2).
| Symptomatic Secondary Cases (N=45) | Asymptomatic Secondary Cases (N=25) | Statistical Significance | |
|---|---|---|---|
| -Woman | 34 (75) | 17 (68) | X2= 0.4639. p= .495789. NS |
| -Age (years) (arithmetic mean and standard deviation) | 38.08 +-20.38 | 21.92+-18.51 | t= 3.28268. p= .000813. Significant at p < .05. |
| ->> = 65 years | 5 (11) | 1 (4) | Fisher exact test= 0.4102. NS |
| -Social-occupancy class con algún tipo de especialización | 18 (40) | 11 (44) | X2= 0.106. p= .744778. NS |
| -Students | 12 (27) | 15 (60) | X2= 7.5366. p= .006046. Significant at p < .05. |
| -Ethnic minority | 15 (33) | 8 (32) | X2= 0.013. p= .909394. NS |
| -Low income household | 17 (38) | 6 (24) | X2= 1.3829. p= .239612. NS |
| -Complex family | 9 (20) | 3 (12) | X2= 0.0819. p= .774777. NS |
| -Familiar size | 3.28+-0.81 | 4.16+-1.02 | t= -3.8971. p= .000113. Significant at p < .05. |
| Number of family members => 4 | 17 (38) | 19 (76) | X2= 9.3994. p= .002171. Significant at p < .05. |
Table 1: ** Comparison between Symptomatic Secondary Cases And Asymptomatic Secondary Cases In The Family (39 Families; N = 70).
( ): Denotes percentages of total in in secondary cases NS: Not significant at p< .05. Table 1: Comparison between Symptomatic Secondary Cases And Asymptomatic Secondary Cases In The Family (39 Families; N = 70).
| Chronic Diseases According To Who, Icd-10 Groups | Symptomatic Secondary Cases (N=45) | Asymptomatic Secondary Cases (N=25) | Statistical Significance |
|---|---|---|---|
| Cases with presence of chronic diseases | 25 (56) | 3 (12) | X2= 12.7037. p= .000365. Significant at p < .05. |
| -II Neoplasms* | 0 | 1 (4) | Fisher exact test = 0.0606. NS |
| -IV Endocrine* | 20 (32) | 1 (4) | Fisher exact test= value is 1. NS |
| -V Mental* | 8 (13) | 2 (8) | Fisher exact test= 0.1058. |
| -VI-VIII Nervous and Senses* | 6 (10) | 0 | Fisher exact test= value is 1. NS |
| -IX Circulatory system* | 5 (8) | 0 | Fisher exact test= value is 1. NS |
| -X Respiratory system* | 3 (5) | 0 | Fisher exact test= value is 1. NS |
| -XI Digestive system* | 5 (8) | 0 | Fisher exact test= value is 1. NS |
| -XII Diseases of the skin* | 3 (5) | 0 | Fisher exact test= value is 1. NS |
| -XIII Musculo-skeletal* | 7 (11) | 1 (4) | Fisher exact test= 0.4113. NS |
| -XIV Genitourinary* | 5 (8) | 0 | Fisher exact test= value is 1. NS |
| TOTAL* | 62 (100) | 4 (100) |
Table 2: ** Comparison Chronic Diseases between Symptomatic Secondary Cases and Asymptomatic Secondary Cases in the Family (39 Fa
( ): Denotes percentages *Patients could have more than one chronic disease. The percentages are over the total of chronic disease of primary and secondary cases NS: Not significant at p< .05. Table 2: Comparison Chronic Diseases between Symptomatic Secondary Cases and Asymptomatic Secondary Cases in the Family (39 Families; N = 70).
Discussion
Data published in China suggest that most of the person-to-person transmission of SARS-CoV-2 has occurred in families [3]. On the other hand, one of the most striking aspects of COVID-19 is the marked differences in experiences of the disease. Some people never develop symptoms, while others, some apparently healthy, have severe or even fatal pneumonia [40]. Many studies have focused on characterizing the heterogeneity of COVID-19 in demographic terms, with clear evidence of higher mortality in men and older people. Although doubts remain about additional determinants of the disease, such as pre-existing comorbidities, viral variants, genetic risk factors of the disease host, as well as adaptation or tolerance to infection [41, 42].
Importance and Epidemiology of Asymptomatic Infections. Prevalence of Asymptomatic SARS Co-V-2 Infections While it has been reported in a study in Wuhan, when the outbreak was being controlled, that asymptomatic cases of COVID-19 may not be infectious, as researchers found no “viable viruses” in cultures of asymptomatic samples, these findings are not applicable as a general rule, nor do they rule out that the virus can be transmitted by asymptomatic carriers. What’s more, there is plenty of evidence elsewhere showing that people infected with COVID-19 can be temporarily asymptomatic and infectious, before developing symptoms. Moreover, using antibody tests, it has been shown that almost two-thirds of asymptomatic cases have previously had COVID-19 [43].
Current evidence suggests that about one in five infected people will experience no symptoms and will transmit the virus to significantly fewer people than someone with symptoms. But researchers are divided on whether asymptomatic infections act as a “silent driver” of the pandemic [22]. It is recognized that the risk of an asymptomatic person transmitting the virus to others in their household is about a quarter of the risk of transmitting from symptomatic person [44, 45]. But, although there is a lower risk of transmission from asymptomatic people, they could still present a significant risk to public health because they are more likely to be in the community than isolated. The actual public health burden of this massive group of ‘asymptomatic’ interacting in the community probably suggests that a considerable part of transmission events stem from asymptomatic transmissions [22].
In this regard, a modeling study in the United States estimated that more than half of the transmissions come from presymptomatic and asymptomatic individuals, indicating that symptom-based detection will have little effect on spread. Carriers of SARS CoV-2 occur most frequently in middle-aged people who had close contact with infected relatives [46]. About half of adults with COVID-19 report that they had no known close contact with an infected individual in the 2 weeks prior to their illness; among those who reported close contact with an infected person, that person was most often (45% of cases) a family member [47]. Children seem to have less risk of becoming infected; however, their stool samples and nasopharyngeal swabs may remain positive for SARS-CoV-2 for more than two weeks after resolution of symptoms, although its role in transmission has not yet been established [48].
Symptomatic and asymptomatic cases must be studied separately to understand the dynamics of infection [30]. While many factors beyond viral load can contribute to infectivity, viral loads have been reported to be similar between asymptomatic and symptomatic (including presymptomatic) patients. Furthermore, viral loads tend to decrease more slowly in asymptomatic patients [25, 49, 50].
The prevalence of asymptomatic cases in the general population has been reported to be around 20%, with a wide range that ranged from 3 to 67%; if the population bias is analyzed, the percentage of asymptomatic patients rose to 31% [51]. Our study in families found a prevalence of asymptomatic secondary cases of 36%. In relation to the previously published prevalence of asymptomatic cases in the same general population, which was 23% [18], the frequency of secondary cases in families is clearly higher.
Asymptomatic Secondary Cases Vs. Symptomatic In Families: Younger, Healthier and Students It is known that transmission is more likely to occur indoors than outdoors. The cumulative risk to household contacts of an infected person is likely to be substantial during the peak of viral shedding. Household members who are older, have underlying medical conditions, or share a bed or vehicle with the index case are the most susceptible. The dominant scientific view of asymptomatic patients is that their immune systems are especially well tuned. This could explain why children and young adults make up the majority of people without symptoms because the immune system naturally deteriorates with age. It is also possible that the immune system of the asymptomatic has been primed by a previous infection with a milder coronavirus, such as those that cause the common cold [52].
In our study it is also found in the field of family contacts, as occurs in the general population, that asymptomatic secondary cases compared to symptomatic cases were younger, students, they presented fewer chronic diseases, and the family was larger. These data follow what has been shown in other studies: asymptomatic infections are more common in populations of young individuals and in middle age (average age according to different studies, between 26 and 49 years). Age can play an important role in the severity of COVID-19, and this is related to different immune responses [15, 30, 53, 54]. Regarding children and adolescents (which includes variable ages: 0-22 years in some study; 3-18 years in others, etc.), it has been reported that they can develop COVID-19 and can be a potential source of contagion of the SARS-CoV-2, although most remain asymptomatic or experience mild illness [55, 56]. And it has been suggested that the prevalence of asymptomatic infections in children correlates with the overall incidence of COVID-19 in the local population [57].
Family Size and Frequency of Asymptomatic Secondary Cases: More Asymptomatic Secondary Cases in Larger Families
SARS CoV-2 doesn’t need a huge crowd to wreak havoc. A small gathering in a small space can be just as risky. Since the virus is known to be transmitted from person to person [3, 4, 5, 6, 7] and travels through the air in tiny droplets when an infected person speaks, coughs, laughs, sings, or even breathes, physical distance is an important factor in helping to prevent the spread of the virus [58].
Outbreaks in cities, which likely involve transmission within large multigenerational households, show the importance of implementing appropriate public health measures to prevent sudden increases in infections [47]. Large families have been described as posing a risk for transmitting SARS-CoV-2 [59]. Likewise, it has been reported that the secondary attack rate of COVID-19 in domestic contacts is closely associated with family size [60, 61], and this pattern also seems to occur in asymptomatic cases in the family [62]. We also found that the families of asymptomatic secondary cases were larger in size.
Comorbidities
The proportion of asymptomatic or presymptomatic infections in the population with medical comorbidities and an increased risk of severe disease is unclear. A study showed that 40% of skilled nursing facility SARS-CoV-2 infections were asymptomatic; a relatively high proportion of asymptomatic infections in a population expected to have multiple risk factors for severe COVID-19 [63]. Our study found that there were fewer asymptomatic secondary cases in the family with the presence of chronic diseases, but without differences by disease groups. Another previous study in the same setting and referred to the general population did not find statistically significant differences in comorbidities between asymptomatic and symptomatic patients, neither by their total number, nor by groups of diseases [18].
Implications of Asymptomatic Infections
Transmission of SARS-CoV-2 from asymptomatic or presymptomatic people complicates public health measures aimed at controlling the pandemic. In view of the substantial prevalence of asymptomatic infections, routine testing of close contacts regardless of symptoms will reduce missed diagnoses. Until an effective vaccine is widely available, strategies to prevent home transmission and to support people in quarantine will be vital and should be a critical part of any strategy [64, 65].
The indications of numerous international organizations have led to antigen tests being used in symptomatic cases, where they were best studied by manufacturers. But some studies suggest that they could also be used for close contacts without symptoms [64, 65]. Therefore, the focus of testing programs for SARS-CoV-2 should be expanded to include people who do not have symptoms of COVID-19. In this way, opportunistic detection with rapid response tests for COVID-19 available to everyone, specifically for those who do not have symptoms in the family and at home, would be advisable; but also in the doctor’s office, and even in concerts, in the cinema, in large commercial areas, etc., administered by anyone (and maintaining the rest of the public health measures: masks, social distancing, hand washing, mobility limitation). In summary, families with asymptomatic COVID-19 should be proactively searched for, especially with a greater number of young, healthy members, and students, because they can transmit SARS-CoV-2 and it will be necessary to contain them if the objective of the policy is to minimize cases and transmission [24, 66, 67, 68].
Limitations and Strengths of the Study
- The study has the strength of its longitudinality, characteristic of work in general medicine.
- It has the limitations of being a retrospective design, being an opportunistic sample and of small size, although considering the statistical requirements for the results of the main variables. Furthermore, there are no apparent reasons that the families and individuals included could differ from, or be over, or underrepresented from those who would have been included in a probability sample.
Conclusion
The true burden of asymptomatic disease is not yet known, but it is emerging as both PCR and antibody tests to establish seroprevalence have become more available. In the context of general medicine in Toledo (Spain), during March 15 to December 31, 2020, the prevalence of asymptomatic secondary cases in families is high (36%). Being an asymptomatic versus symptomatic secondary COVID-19 case in the family was associated with being younger, healthier, being a student, and living in a family with a greater number of members. Young students in large families are a risk group for secondary cases, which may favor the transmission of SARS-CoV-2 in family and extra-family contexts. The focus of testing programs for SARS-CoV-2 should be expanded to include young, healthy, and COVID-19 symptom-free individuals, especially all contacts from large families and in school settings.
References
-
Zhu N, Zhang D, Wang W, Li X, Yang B, et al. (2020) A Novel Coronavirus from Patients with Pneumonia in China, 2019. N Engl J Med 382(8): 727-733.
-
Coronavirus COVID-19 Global Cases by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins. The Center for Systems Science and Engineering (CSSE) at JHU.
-
Wang Y, Tian H, Zhang L, Zhang M, Guo D, et al. (2020) Reduction of secondary transmission of SARS-CoV-2 in households by face mask use, disinfection and social distancing: a cohort study in Beijing, China. BMJ Global Health 5(5): 002794.
-
Tong ZD, Tang A, Li KF, Li P, Wang HL, et al. (2020) Potential Presymptomatic Transmission of SARS-CoV-2, Zhejiang Province, China, 2020. Emerg Infect Dis 26(5): 1052-1054.
-
(2020) The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Zhonghua Liu Xing Bing Xue Za Zhi 41(2): 145- 151.
-
Rothe C, Schunk M, Sothmann P, Bretzel G, Froeschl G, et al. (2020) Transmission of 2019-nCoV Infection from an Asymptomatic Contact in Germany. N Engl J Med 382(10): 970-971.
-
Wang L, Didelot X, Yang J, Wong G, Shi Y, et al. (2020) Inference of person-to-person transmission of COVID-19 reveals hidden super-spreading events during the early outbreak phase. Nature Communications 11: 5006.
-
Bai Y, Yao L, Wei T, Tian F, Jin DY, et al. (2020) Presumed Asymptomatic Carrier Transmission of COVID-19. JAMA 323(14): 1406-1407.
-
Lee S, Meyler P, Mozel M, Tauh T, Merchant R (2020) Asymptomatic carriage and transmission of SARS-CoV-2: What do we know?. Can J Anaesth 67(10): 1424-1430.
-
Yu P, Zhu J, Zhang Z, Han Y (2020) A Familial Cluster of Infection Associated With the 2019 Novel Coronavirus Indicating Possible Person-to-Person Transmission During the Incubation Period. J Infect Dis 221(11): 1757- 1761.
-
Wei WE, Li Z, Chiew CJ, Yong SE, Toh MP, et al. (2020) Presymptomatic Transmission of SARS-CoV-2-Singapore, January 23- March 16, 2020. MMWR Morb Mortal Wkly Rep 69(14): 411-415.
-
Gandhi M, Yokoe DS, Havlir DV (2020) Asymptomatic Transmission, the Achilles’ Heel of Current Strategies to Control Covid-19. N Engl J Med 382: 2158-2160.
-
Meyerowitz EA, Richterman A, Bogoch II, Low N, Cevik M (2020) Towards an accurate and systematic characterisation of persistently asymptomatic infection with SARS-CoV-2: Lancet Infect Dis.
-
Carvalho T (2020) Silent spread. Nat Med 26: 1807.
-
Oran DP, Topol EJ (2020) Prevalence of Asymptomatic SARS-CoV-2 Infection: A Narrative Review. Ann Intern Med 173: 362-367.
-
Buitrago-Garcia D, Egli-Gany D, Counotte MJ, Hossmann S, Imeri H, et al. (2020) Occurrence and transmission potential of asymptomatic and presymptomatic SARS- CoV-2 infections: A living systematic review and meta- analysis. Plos Medicine 17(9): 1003346.
-
Byambasuren O, Cardona M, Bell K, Clark J, Mclaws ML, et al. (2020) Estimating the extent of asymptomatic COVID-19 and its potential for community transmission: systematic review and meta-analysis. MedRxiv.
-
Turabian JL (2020) Prevalence and Comparison of Asymptomatic and Symptomatic Patients with SARS- CoV-2 Infection in a General Medicine Office in Toledo, Spain. Epidemol Int J 4(2): 1-11.
-
Pollán M, Gómez BP, Barriuso RP, Oteo J, Hernan MA, et al. (2020) Prevalence of SARS-CoV-2 in Spain (ENE-COVID): a nationwide, population-based seroepidemiological study. The Lancet 396(10250): 535-544.
-
Pollock AM, Lancaster J (2020) Asymptomatic transmission of covid-19. BMJ 371: 4851.
-
Engler JHW (2020) Rapid Response: Evidence of asymptomatic spread is insufficient to justify mass testing for Covid-19. BMJ 371: 4436.
-
Nogrady B (2020) What the data say about asymptomatic COVID infections. People without symptoms can pass on the virus, but estimating their contribution to outbreaks is challenging. Nature.
-
Turabian JL (2020) The Importance of Asymptomatic Coronavirus Disease-19 Patients: Never Trust a “Silent Customer”. J Community Prev Med 3(2): 1-7.
-
Turabian JL (2021) Casos Familiares Asintomáticos de Covid-19 Asymptomatic Family Cases of Covid-19. Archivos De Medicina 17(1): 1-3.
-
Lee S, Kim T, Lee E, Lee C, Kim H, et al. (2020) Clinical course and molecular viral shedding among asymptomatic and symptomatic patients with SARS-CoV-2 infection in a community treatment center in the Republic of Korea. JAMA Intern Med 180(11): 1447-1452.
-
He X, Lau EHY, Wu P, Deng X, Wang J, et al. (2020) Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat Med 26: 672-675.
-
Hope JL, Bradley LM (2021) Lessons in antiviral immunity. Science 371(6528): 464-465.
-
Little P, Read RC, Amlôt R, Chadborn T, Rice C, et al. (2020) Reducing risks from coronavirus transmission in the home-the role of viral load. BMJ 369: 1728.
-
Turabian JL (2021) SARS-COV-2 infection prevalence and characteristics in domestic contacts: Study of 39 families and 132 people in a general medicine clinic in Toledo (Spain): Implications for the general practitioners. Int J Epidemiol Health Sci 2(1).
-
Mao S, Huang T, Yuan H, Li M, Huang X, et al. (2020) Epidemiological analysis of 67 local COVID-19 clusters in Sichuan Province, China. BMC Public Health 20: 1525.
-
Strauss AL (1984) Chronic illness and the quality of life. St Louis: The CV Mosby Company.
-
WHO (2019) International Statistical Classification of Diseases and Health-Related Problems. ICD-10 Version.
-
Royal Collage of General Practitioners (1986) The Classification and Analisis of General Practice Data.
-
Donaldson RJ, Donaldson LJ (1983) Essential Comunity Medicine. Lancaster: MTP Press.
-
Turabian JL (2017) Family Genogram in General Medicine: A Soft Technology that can be Strong. An Update. Res Med Eng Sci 3(1): 186-191.
-
Russell LT (2020) Capturing Family Complexity in Family Nursing Research and Practice. J Fam Nurs 26(4): 287- 293.
-
Watts C, Shrader E (1998) How to do (or not to do)…The genogram: A new research tool to document patterns of decision-making, conflict and vulnerability within households. Health Policy and Planning 13(4): 459-464.
-
McIlvain H, Crabtree B, Medder J, Stange KC, Miller WL (1998) Using practice genograms to understand and describe practice configurations. Fam Med 30(7): 490- 496.
-
Open Source Epidemiologic Statistics for Public Health.
-
Callaway E, Ledford H, Mallapaty S (2020) Six months of coronavirus: the mysteries scientists are still racing to solve. Nature 583(7815): 178-179.
-
Beck DB, Aksentijevich I (2020) Susceptibility to severe COVID-19. Science 370(6515): 404-405.
-
Young BE, Fong SW, Chan YH, Mak TM, Ang LW, et al. (2020) Effects of a major deletion in the SARS- CoV-2 genome on the severity of infection and the inflammatory response: An observational cohort study. Lancet 396(10251): 603-611.
-
Griffin S (2020) Covid-19: Asymptomatic cases may not be infectious, Wuhan study indicates. BMJ 371: 4695.
-
Bi Q, Lessler J, Eckerle I, Lauer SA, Kaiser L (2020) Household Transmission of SARS-CoV-2: Insights from a Population-based Serological Survey. MedRxiv.
-
Johansson MA, Quandelacy TM, Kada S, Prasad PV, Steele M, et al. (2021 ) SARS-CoV-2 Transmission From People Without COVID-19 Symptoms. JAMA Netw Open 4(1): 2035057.
-
Wang Y, Liu Y, Liu L, Wang X, Luo N, et al. (2020) Clinical Outcomes in 55 Patients With Severe Acute Respiratory Syndrome Coronavirus 2 Who Were Asymptomatic at Hospital Admission in Shenzhen, China. J Infect Dis 221(11): 1770-1774.
-
Tenforde MW, Rose EB, Lindsell CJ, Shapiro NP, Files DC, et al. (2020) Characteristics of Adult Outpatients and Inpatients with COVID-19-11 Academic Medical Centers, United States, March-May 2020. MMWR Morb Mortal Wkly Rep 69(26): 841-846.
-
Haroon S, Chandan JS, Middleton J, Cheng KK (2020) Covid-19: breaking the chain of household transmission. BMJ 370: 3181.
-
Stadnytskyi V, Bax CE, Bax A, Anfinrud P (2020) The airborne lifetime of small speech droplets and their potential importance in SARS-CoV-2 transmission. Proc Natl Acad Sci USA 117(22): 11875-11877.
-
Laurie Barclay (2020) COVID-19: What Is the Primary Route of Transmission? Medscape Education Clinical Briefs.
-
Bloom JA, Erlichman Z, Tian T, Doron S, Chen L, et al. (2020) The prevalence of asymptomatic carriers of COVID-19 as determined by routine preoperative testing. J Infect Prev 22(1): 7-11.
-
Laber-Warren E (2020) Why Do Some People Weather Coronavirus Infection Unscathed? Medscape.
-
Gao Z, Xu Y, Sun C, Wang X, Guo Y, et al. (2020) A Systematic Review of Asymptomatic Infections with COVID-19. J Microbiol Immunol Infect 54(1): 12-16.
-
Yang R, Gui X, Xiong Y (2020) Comparison of Clinical Characteristics of Patients with Asymptomatic vs Symptomatic Coronavirus Disease 2019 in Wuhan, China. JAMA Netw Open 3(5): 2010182.
-
Yonker LM, Neilan AM, Bartsch Y, Patel AB, Regan J, et al. (2020) Pediatric Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2): Clinical Presentation, Infectivity, and Immune Responses. J Pediatr 227: 45-52.
-
Lordan R, FitzGerald GA, Grosser T (2020) Reopening schools during COVID-19. Science 369(6508): 1146.
-
Sola AM, David AP, Rosbe KW, Baba A, Ramirez Avila L, et al. (2020) Prevalence of SARS-CoV-2 Infection in Children Without Symptoms of Coronavirus Disease 2019. JAMA Pediatr 175(2): 198-201.
-
WHO (2020) Q&A: How is COVID-19 transmitted? Feature story. Ha Noi.
-
Lovett I, Frosch D, Overberg P (2020) Covid-19 Stalks Large Families in Rural America. Remote regions with crowded households have turned deadlier than some city blocks. The Wall Street Journal.
-
Madewell ZJ, Yang Y, Longini IM, Halloran ME, Dean NE (2020) Household Transmission of SARS-CoV-2: A Systematic Review and Meta-analysis. JAMA Netw Open 3(12): 2031756.
-
Shah K, Kandre Y, Mavalankar D (2021) Secondary attack rate in household contacts of COVID-19 Paediatric index cases: a study from Western India. J Public Health.
-
Zhang H, Hong C, Zheng Q, Zhou P, Zhu Y, et al. (2020) A multi-family cluster of COVID-19 associated with asymptomatic and pre-symptomatic transmission in Jixi City, Heilongjiang, China, 2020. Emerging Microbes & Infections 9(1): 2509-2514.
-
White EM, Santostefano CM, Feifer RA, Kosar CM, Blackman C, et al. (2020) Asymptomatic and presymptomatic severe acute respiratory syndrome coronavirus 2 infection rates in a multistate sample of skilled nursing facilities. JAMA Inter Med 180(12): 1709- 1711.
-
The European Commission (2020) Commission Recommendation of 18.11.2020 on the use of rapid antigen tests for the diagnosis of SARS-CoV-2 infection.
-
Alemany A, Baro B, Ouchi D, Ubals M, Corbacho-Monne M, et al. (2020) Analytical and Clinical Performance of the Panbio COVID-19 Antigen-Detecting Rapid Diagnostic Test. MedRxiv.
-
Turabian JL (2021) Rapid antigenic tests to detect asymptomatic covid-19 infections. Arch Community Med Public Health 7(1): 17-20.
-
Turabian JL (2021) Asymptomatic Covid-19: A Model Kit. Int Res Med Health Sci (4-1): 1-7.
-
De Reuters E (2021) Madrid begins to carry out massive tests to young people to detect COVID-19. Medscape.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria