Dysergonomic Evaluation: Based on ISO 11226-2000, in Oil Production Operators
Introduction: In ergonomics, adaptation to the work area concerns the man. In the oil production areas, it requires diverse work, adopting different forced positions in each of the tasks, causing musculoskeletal pathologies or musculoskeletal disorder (SMD). In a study carried out on several operators of the production plants, the different postures per exposure are identified, in order to determine some clinical occupational picture. when applying the ISO 11226-2000 methodology for forced postures and based on the calculation of the finite sample of 411 operators, 63.5% represent low back pain, while 24.9% present an occupational clinical picture of cervical problems and 11.6% tolerate TME. Results and Conclusions: In the main dysergonomic pains, they are analyzed according to the work cycles per task to be performed, certain pathologies such as thoracolumbar spine (waist), cervical spine (neck), rotator cuff syndrome or capium tunnel syndrome. Therefore, these symptoms over time become chronic, affecting health, since an occupational health plan with an emphasis on postural biometrics reduces exposure to forced postures.
Guillermo Neusa Arenas1*, Jeanette del Pilar Ureña Aguirre2, Ramiro Vicente Saraguro3 and Jessica Karina Freire Soria4
Introduction
When I studied applied ergonomics from my professional principles, I read many dialogical contexts about the study and concepts of Ergonomics, since then when I read the book, Ergonomics: what for, from the German psychologist [1]; a chain of interest and knowledge transcended me and led me to the development of research projects in the field of Applied Ergonomics in general. Through each paragraph in its pages, different studies are analyzed, both cognitive, practical and theoretical, creating a discipline that should be developed in all areas of work in the sciences of safety and health at work. Then, when analyzing the book, I was not in the nomological and competent, as to describe the integration towards other sciences of technical and scientific study, which addresses a more transcendental discipline in Ergonomics and its branches.
Before carrying out an ergonomic study or analysis of the dimensional conditions of one or several systems, it is necessary to consider the work methodologies that are or will be in the future; “if the methods are not considered optimal we must redesign them” [2].
According to the European Agency for Safety and Health at Work (EASH). The musculoskeletal disorder (MSD) of occupational origin, acquires a clinical picture in the health of workers both in Latin American countries and in the European Union, causing economic losses in all productive sectors and public organizations [3].
On the other hand, the SGRT-IESS-Ecuador, defines that, “the parts of the body that are most affected in work accidents are: the upper limb with 33.4% and the lower limb with 25.5%. In the case of the upper limb, the fingers of the left hand are most affected with 25.0% and the fingers of the right hand with 22.7%. The lower limb was most affected by the right ankle with 14.7% and the left with 11.6%. Five types of injuries were identified as the most representative: Superficial injuries, with 32.1%, fractures, with 20.2%, other injuries, with 20.0%, contusions and crushes, with 7.6% and finally sprains and strains, with 6.6%; the remaining injuries represented less than 5.0%. However, 5 types of injuries were identified as the most representative and they were Superficial trauma with 32.1%, fractures with 20.2%, other injuries with 20.0%, contusions and crushes with 7.6% and finally sprains and strains with 6.6%; the remaining injuries represented less than 5.0% [4].
Physical Ergonomics applied to the workforce of engineers, technicians or operators, who assume responsibility in production processes, shows that they are exposed to dysergonomic risks, which is why, “MSDs are, for years, one of the problems that affect massively all professional categories, causing significant economic losses in organizations. In view of this environment, it is necessary to focus efforts and provide instruments of adequate preventive control in the worker, to minimize the effective and decrease of occupational disease or accidents in the workplace [5].
MSDs cause clinical occupational symptoms that especially affect the back, shoulders, neck and in many cases the upper extremities. However, in several studies carried out on operators of crude oil production plants, they also affect the lower extremities, such as knee pain, achilles’ heel or the palm of the foot, producing pain in the short, medium or long term, according to the operator’s work cycles. Some MSDs, which can produce clinical occupational disease of origin such as carpal tunnel syndrome, their symptoms can become very sensitive to health considerations because of their constant exposure by repetition. Others may not be severe, as you may only have pain or fatigue with no clear symptoms due to a specific disorder.
In the study, approximately four out of six operators in the production plants claim to have repetitive movements in their hands and arms, while six out of four operators withstand the vibration of machines, motors and/or equipment in the production areas; These scenarios institute an important risk factor for the appearance of MSDs or SCIs (musculoskeletal injuries) of occupational origin, originating pathologies in the neck and upper extremities such as TMOLCES (Musculoskeletal Disorders of Occupational Origin). A large number of operators in the different areas tolerate this type of SCI or MSD, in the neck or upper extremities, which causes occupational pathologies related to the most common cycles of exposure to work in the production areas with 45% of all occupational diseases.
Materials and Methods
Valued Population
During the research (In-Situ) by work cycles in the operators of the different areas or jobs, several methodological aspects of application are analyzed in the three phases such as: sample calculation, risk factor identification, application of the method for risk assessment, expected results according to the analyses, occupational pathologies identified according to the activities by tasks, and conclusions.
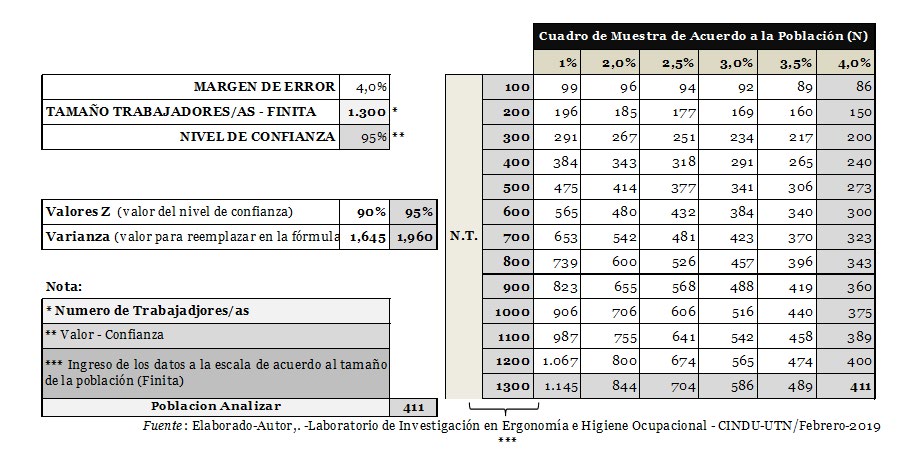
However, based on 1300 operators to calculate the finite sample of men and women from different areas in the crude oil production plants, an average of 411 operators was established, with a 4.0% margin of error and 95% reliability. Figure 1 shows the calculation of the finite sample, according to the Vallejo method [6].
Once the sample size is chosen, the selection criteria are established, establishing a random or systematic method, reaching the evaluation of the interval between the sample applied according to the dysergonomic risk factor for exposure.
Identification of Study Areas
When determining the total number of operators in each area, various aspects of anthropometry and sizing are taken into account, such as the height of the workstation level that corresponds to the anthropometric1 measurements of the operator, times and work cycles for musculoskeletal movement and types of movement due to the force of the body during its activity, determining work times and spaces. However, in table 1, the population of operators in the areas of operation in the production plant is characterized.
| Area | Job Title |
| Warehouse | Materials technician |
| Energy | Topping Plant CoordinatorAsep EngineerGeneration operatorCrude oil generation operatorGas and diesel generation operatorTopping plant operator |
| Maintenance | Coordinator of auxiliary services and rights of way.Static maintenance coordinatorTechnical inspection and coating engineer.Crane operatorWelderConstruction SupervisorGas and diesel instrumentation and control technicianElectrical Maintenance TechnicianRotary maintenance technicianOverhaul TechnicianPiping TechnicianSupervising Technician |
| Operations | Field Manager |
| Production | Transport Production ManagerProduction operatorSupervisor TowVacum Technician |
| P Y O | Camp CoordinatorP and O Manager and Social WorkCamp TechnicianAdministrative Assistant |
| Community Relations | Construction Supervisor |
| TI | CoordinatorTechnical user supportEngineeringCoordinator |
Table 1: Identification by work area.
¹ Anthropometry is considered, the science that studies and analyzes the measures of the human body.
Interpretation of Initial Data
Based on the Nordic Questionnaire (NC) of Kuorinka [7], a postural biometry analysis was performed at each work station of the plant operators, with the aim of establishing the validity and reliability of the Clinical Functional Assessment (CFA) for dysergonomic exposure, taking into account both pathological and occupational clinical factors.
The diagnosis by dysergonomic health, is really a diagnosis of approach to the physiological context of the worker by its exposure, that is to say, of approach to the great variety of certain consequences as much psychological, biological and social that, to the use of a combination of the two can produce an alteration in the health of the operator or collective, creating a pathological picture, disability or death. However, by insisting on a clinical-pathological or epidemiological approach to the solution of problems caused by MSDs or SCIs, the situation is analysed in terms of the specific health-disease of the operators, identifying their difficulties during or after each work cycle. Therefore, establishing the measurement of these dysergonomic risk factors is prioritized and prioritized both qualitatively and quantitatively, as a previous step to achieving the fundamental purpose of health prevention, which allows us to improve the health status of all operators with specific measures and determined deadlines. In table 2, the most frequent pathologies with TLV2 formation are defined (Table 2).
| TME (ECF) | FRO (CN) | Evaluated (n)= | |
|---|---|---|---|
| Posture of the trunk | Acceptable | 2% | 411 |
| Not recommended | 5% | ||
| Head Posture | Acceptable | 2% | |
| Not recommended | 5% | ||
| Shoulder and arm position | Acceptable | 4% | |
| Not recommended | 3% | ||
| Forearm and hand position | Acceptable | 3% | |
| Not recommended | 4% | ||
| Knee and Ankle Posture | Acceptable | 5% | |
| Not recommended | 2% |
Table 2: Occupational Risk Factor (ORF) of symptoms due to pain in the body, based on the analysis of the Nordic Questionnaire (N
Table 2: Occupational Risk Factor (ORF) of symptoms due to pain in the body, based on the analysis of the Nordic Questionnaire (NC) and its Clinical Functional Assessment (CFA), the estimation by cases of pathologies or clinical picture with pain in the last 3 months. (n=411). Source; Laboratory for Research in Ergonomics and Occupational Hygiene-2019.
Prevention is defined as the set of activities or measures foreseen in all phases of activity of an organization, in order to avoid or reduce risks derived from work [8].
There are different aspects of biomechanical measurement analysis, according to the application of ISO 11226-2000, allowing the evaluation of the body by standard and inclination movements, which allow setting both repetitive and force or no force cycles. Therefore, in exposures by age, osteomuscular movement and the alteration by MSD or SML3, in each of the tasks to be performed, will depend on the work cycles.
According to the COA, the different musculoskeletal
2 Threshold Limit Values (TLV) 3 It is related to discomfort, pain or muscle tension from some type of injury. 4 It is the analysis of the measures and standards of living beings.
alterations have many names, for example: carpal tunnel syndrome, tendonitis, tenosynovitis, herniated discs, contractures, epicondylitis, bursitis, lumbago, cervicalgia. However, we refer to all kinds of pathologies by these injuries, we use the term SCI [9].
Dysergonomic Risk Factor Considerations by Postural Biometry
To determine the assessments by postural biometrics4 in the operators, we can define it mainly or by reference to other methods such as OWAS Ovako Working Analysis System, which allows the assessment of the physical load by the biomechanics of the body, derived from the different inappropriate postures during the work cycle. As opposed to the method by postures such as RULA or REBA, estimating individual postures, OWAS, is characterized by its ability to assess globally all the postures adopted during the performance of the task. As compensation, OWAS provides less accurate assessments than the previous ones. However, when considering multiple postures over time, which makes OWAS a relatively old method, it remains one of the most widely used methods of evaluating postural burden [10].
On the other hand, the REBA method (it is the acronym of Rapid Entire Body Assessment), considers to determine if inadequate postures are adopted in the work cycles in a continuous or repetitive way in the activity, task or during the work [11].
Fatigue or prolonged task times can lead to health difficulties; a dysergonomic risk factor is the appearance of musculoskeletal disorders, when excessive postural stress exists. Therefore, the evaluation made to the operators by the postural load and the static load, determined several fundamental factors for the measures to be adopted in improvement of the areas or jobs.
By applying the method of the ISO 11226: 2000- Ergonomics - Evaluation of static working postures, in the Operators of Raw Material Production Plants, it aims at evaluating and estimating postures by working cycles and their static exposure. Therefore, in figure 2, in the application by tasks and time cycles in the operations, it provides enough difference both in the physical and mental part. “This means that every work cycle has enough variety for tasks to be performed”; for example: an adequate number of organized activities, is an appropriate combination of tasks by work cycles to long, medium and short cycles of osteomuscular movement, which is distributed or balanced in the simple and complex tasks. Therefore, “there is sufficient autonomy and possibilities for communication, information and learning” [12].
The analyses by ISO 11226: 2000, are more suitable for each of the studies by operator. Therefore, the biomechanical movement of the body and, for the precision located as the estimation and evaluation, aspects of time and space of the osteomuscular displacement are defined; because, in many cases, it is enough to see and observe both directly and in- situ, (without equipment or measurement systems), the better the evaluation of observation, it is established through the observation of videos and photographs in their different activities by work cycles, because, it is more punctual to determine the analysis of the cycles of duration of the task and the space during the task.
Results
In the evaluation of postures by work cycles, applying the method of ISO Standard 11226: 2000, several aspects of movement by postural biometry were established as a) Posture of the trunk: it is evaluated considering aspects of movement in the trunk. A symmetrical trunk posture implies that there is no axial rotation (or rotation), nor lateral flexion of the upper part of the trunk (thorax) with respect to the pelvis. However, the angle α is determined by the posture of the trunk during the performance of the task (continuous stroke) with respect to the reference posture (dotted line), as shown in Figure 2.
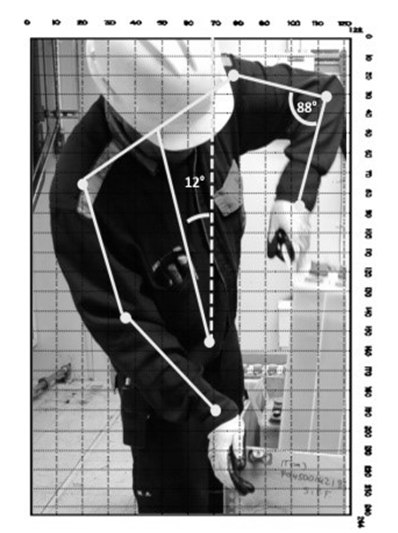
Therefore, the convex curvature of the lumbar spine, this posture often occurs when: 1st to the lumbar spine, where it is not supported by a backrest, and 2nd, when a small hip angle is adopted, in table 3
| Acceptable | Go to step 2 | Not recommended | |
|---|---|---|---|
| 1) Symmetrical trunk position (a) | |||
| No | X | ||
| Yes | X | ||
| 2) Log Tilt α (b) | |||
| > 60° | X | ||
| 20° - 60° without full support of the troco | X | ||
| 20° - 60° with full support of the troco | X | ||
| 0° - 20° | X | ||
| < 0° without full support of the troco | X | ||
| < 0° with full support of the troco | X | ||
| 3) For sitting position: convex lumbar zone position (c) | |||
| No | X | ||
| Yes | X | ||
| Duty Cycle Time | Acceptable | Not recommended | |
| > maximum acceptable cycle time | X | ||
| ≤ maximum acceptable cycle time | X | ||
Table 3: Postural exposure of the trunk.
b) Head position: For the evaluation of the head position the following procedure is followed: The head position must be evaluated considering both the angle inclination, β that, determines the accomplishment of the task (continuous line) with respect to the reference position (dotted line). Based on figure 2, in the case of the following figure, β has a positive sign. as well as the posture with respect to the posture of the trunk, see table 4: Assessment criteria for head posture:
| Acceptable | Go to step 2 | Not recommended | |
|---|---|---|---|
| 1) Symmetrical neck posture (a) | |||
| No | X | ||
| Yes | X | ||
| 2) Log Tilt β (b) | |||
| > 85° | X | X | |
| 25° - 85° without full trocar support (c); go to item 3 | |||
| 25° - 85° with full trunk support | X | ||
| 0° - 25° | X | ||
| < 0° without full head support | X | ||
| < 0° with full head support | X | ||
| 3) Neck flexion/extension (β-α) (b) | |||
| > 25° | X | ||
| 0° - 25° | X | ||
| <0° | X | ||
Table 4: Postural exposure of the assessment criterion by shoulder and arm posture.
c) Posture of the upper extremities: The posture of the shoulder and arm, should be evaluated by the posture of the shoulder and arm applying table 5; in figure 2, the retroflexion is represented (elbow behind the trunk, when we rotate the profile), the adduction (elbow not visible when looking from behind the trunk) and the extreme external rotation of the arm (the rotation of the shoulder outwards around the longitudinal axis of the arm). However, the angle determines the posture during the execution of the task (in line of posture) with respect to the reference postural biometry (dashed line).
| Acceptable | Not recommended | |
|---|---|---|
| 1) Extreme bend/extension of the elbow (a) | ||
| No | X | |
| Yes | X | |
| 2) Extreme forearm pronation/supination (a) | ||
| No | X | |
| Yes | X | |
| 3) Extreme posture of the wrist (b) | ||
| No | X | |
| Yes | X | |
Table 5: Postural exposure of the assessment criterion by shoulder and arm posture.
d) Posture of the lower extremities: These postures of the lower extremities are evaluated according to the table 6. Item 3 of the table refers only to the standing position, except when a “foot support” is used (i.e., a device that allows part of the body’s weight to rest on a small seat while standing). Item 4 of the table refers only to the “sitting” position.
However, special attention should be paid to providing:
- a balanced distribution of the body’s weight on both feet when standing or using a “stand”;
- adequate support of the body by means of a stable seat, footrest, or “stand”, whichever is applied; and
- a favourable position of the ankle and knee when operating a pedal while sitting, see table 6.
| Acceptable | Not recommended | |
|---|---|---|
| 1) Extreme knee flexion (a) | ||
| No | X | |
| Yes | X | |
| 2) Dorsiflexion/plantar extreme ankle flexion (a) | ||
| No | X | |
| Yes | X | |
| 3) Standing (except when a foot support is attached): bent knee (b) | ||
| No | X | |
| Yes | X | |
| 4) Sitting: Knee angle (c) | ||
| >135° | X (d) | |
| 90°-135° | X | |
| <90° | X | |
Table 6: Postural exposure assessment for the lower extremities.
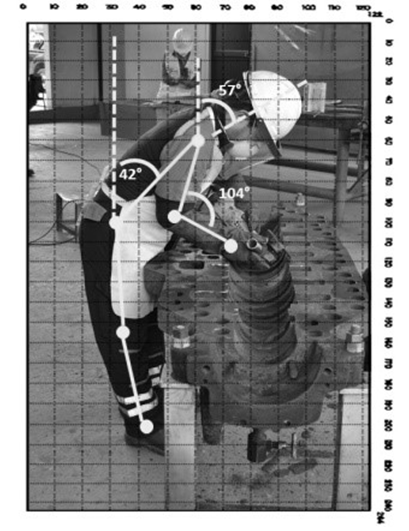
e) Postural Estimation by Exposure Cycles: In Image No. 3, and table No. 7: several aspects of assessment by postural biometry are correlated, based on the results of the ISO 11226: 2000 Standard Method, considering the pathological intensity by clinical picture with pain, in the last 6 months and during the 14 days per shift of work in the body area, in the application and analysis of the CN and the ECF, maintained the (n=411 operators).
| Bursitis | Epicondylitis | Tendinitis | Tenosynovitis | Osteoarthritis | Carpal tunnel syndrome | Hearing loss | |
|---|---|---|---|---|---|---|---|
| Machine operators | 27,10 | 12,40 | 16,20 | 12,40 | 12,00 | 24,10 | 34,30 |
| Machinery Assistants | 19,50 | 21,10 | 23,10 | 15,60 | 15,10 | 11,90 | 11,30 |
| Site personnel | 19,00 | 12,90 | 16,00 | 21,00 | 17,00 | 19,10 | 12,20 |
| Service personnel | 17,10 | 24,10 | 12,40 | 14,20 | 16,20 | 13,70 | 14,60 |
| Yard staff | 9,30 | 10,40 | 11,20 | 19,60 | 23,30 | 13,10 | 15,40 |
| Others | 8,00 | 19,10 | 21,10 | 17,20 | 16,40 | 18,10 | 12,20 |
Table 7: CN and ECF conditions.
f) Most common dysergonomic symptomatologies due to posture: Poor posture at the time of the task, can contribute to a pathological clinical picture, affecting the spine, upper and lower extremities of operators, who spend most of their work cycles in front of an operating activity or the computer. In theory, every work cycle is established at eight hours a day, although in many cases in the oil sector, these cycles are prolonged in accordance with rest times, which is frequently the case with symptoms of MSDs or SCIs.
Other clinical occupational hobbies of operators are the hours without osteomuscular movement, where the joints can create an SCI such as spasms, numbness or tingling, causing problems in the nervous system, muscles and bones, which can be aggravated over time, if there is not adequate posture and spaces in the appropriate work cycles.
Conclusion
In the prevention of the dysergonomic risk factor by organizations, whether they are micro, small, medium or large enterprises, or whether they are public or private, the tools of the new technologies can bring about a change in the quality of life at work. The key to accepting change must come from good motivation and leadership in the entire work team, from the directors, managers, administrators and operational staff, who achieve the development of productivity in each of the organization’s processes. However, by accepting the change, we find ourselves immersed in different paradigms, where it has been indisputable in most of the operators of the crude oil production plants. Therefore, creating a culture of safety and prevention in ergonomics in the organization, is a responsibility and commitment of all those who do prevention. Likewise, when intervening with exaltation, the impact of some operators was uncertain because they used both electronic and manual resources, while in others they expressed some apprehension when they said that they did not master the equipment according to the movement by work cycles with mechanical aids. The results obtained from the method applied by the ISO 11226: 2000 Standard, gave rise to three aspects: a) to carry out epidemiological surveillance follow-up, with special medical examinations of x-rays, which are very advantageous for detecting occupational clinical pictures such as bone anomalies; it evaluates those bone areas that may present ailments, deformities or in many cases, suspicion of some pathology. Frequently, these X-rays or radiographs diagnose tumors, trauma, fractures, deformities and infections (such as hip dysplasia); b) implement mechanical aids, both manual and electrical, that allow operators to minimize forced postures during tasks in the work cycles; c) define an Ergonomics plan with emphasis on postural biometry, with active training and breaks in the short, medium and long term;
Finally, first of all, an information program should be implemented to raise awareness of the use of new technologies or electronic means among all plant personnel. In the second place, it is suggested to motivate the operators, in the business perspective, that allows a process of cognitive and organizational development as a tool, for the health and well-being of all the collaborators of the company.
References
-
Kulka H (1988) Work sciences for engineers - Textbook: 116 images, 81 tables and an appendix. Leipzig, VEB Fachbuchverlag, Berlin.
-
Mondelo PR (2000) Design of Workstations and Work Spaces, Volume 1, Printed in Colombia, Bogota.
-
European Agency for Safety and Health at Work (2019) Work-related musculoskeletal disorders: prevalence, costs and demographics in the EU. Publications Office of the European Union, Luxembourg.
-
General Insurance of Work Risks - IESS-Ecuador (2018) Bimonthly Statistical Bulletin. IESS, Quito.
-
Instituto Canario de Seguridad Labora (2016) Muculosoleptic Disorders of Labour Origin. Directorate General of Labour, Canary Islands Institute of Labour Safety, Canary Islands.
-
Vallejo PM (2012) Sample size required: How many subjects do we need? Statistics applied to Social Sciences.
-
Martinez MM (2017) Validation of the Standardized Nordic Questionnaire of Musculoskeletal Symptoms for the Chilean Working Population, Adding a Scale of Pain. Public Health Journal 21(2): 41-51.
-
Francisco A Sanchez (2007) The Genesis of MSDs: a New Way of Analysis. Ergonomics and Psychocology, pp: 21- 30.
-
Workers’ Commissions of Asturias (2008) Musculoskeletal injuries. Careaga Graphics, Salinas.
-
Diego-Mas JA (2020) Ovako Working Analysis System. Universidad Politécnica de Valencia, España.
-
Diego-Mas JA (2020) Método REBA. Universidad Politécnica de Valencia, España.
-
Fernández MF (2015) Posturas de Trabajo: Evaluación del Riesgo. Instituto Nacional de Seguridad e Higiene en el Trabajo (INSHT), Madrid, pp: 37-50.
- The Expanding Landscape of Road Rage: A Systematic Review of Conflicts Involving Drivers, Pedestrians, and Micromobility
- Validating Cognitive Models of Royal Navy Performance on Control Systems
- Comparing Standard and State-of-the-art Firefighter Coats on Postural Balance and Gait in a Live Burn Environment
- Investigating the Integration of Telemedicine into Clinicians Workflow: A Review of Methods
- Risk Assessment of Ergonomic Factors in a Textile Firm by RULA, REBA and Fine Kinney Methods
- Impact of Self-Esteem Training on Individuals with Disabilities Aged 17-30