Cost-Effectiveness of Idelalisib-Rituximab for the Treatment of Relapsed/Refractory Chronic Lymphocytic Leukemia
Background: A significant survival prolongation was recently reported by adding idelalisib to rituximab (IR) compared with rituximab (R) in the treatment of relapsed/refractory chronic lymphocytic leukemia (CLL). No direct data are available about the relative safety and effectiveness of IR versus other commonly used treatments. The economic impact of novel treatments for CLL is still unknown and no study ever attempted in assessing the benefit-for-cost of IR as compared with the several available treatment options. Aim: To investigate the economic and clinical impact of IR in CLL Objective: To understand the potential clinical and economic advantage of IR in CLL patients who failed one prior treatment line (i.e. refractory to or relapsed after prior treatment lines), as compared with immunotherapy and chemoimmunotherapy. Methods: A treatment-sequence model was developed to estimate the incremental cost per QALY of IR versus R, bendamustine-rituximab (BR) and fludarabine cyclophosphamide-rituximab (FCR) in the second-line treatment setting (i.e. refractory to or relapsed after first-line therapy)in Italy. Tree Age 2015 software was used to simulate second-to-third line treatment sequences by a five-states Markov model: the model was run at monthly steps for 30years.Probabilities of progression were obtained from published randomized and phase II studies (Furman, et al. 2014, Awan, et al. 2014, Fisher, et al. 2011): data were adapted to a second-line setting according to a fixed hazard ratio of 1.4 between subsequent lines. The analysis was performed in the perspective of the Italian national health-care system. Results: Base case analysis reported that IR improved quality-adjusted life expectancy by 1.91, 1.41 and 0.86 years as compared with R, BR and FCR. The incremental cost per quality-adjusted year (QALY) was €2,993, €16,045 and €28,045, respectively. The main drivers of the model were: time horizon, idelalisib unit cost and treatment duration. Deterministic and probabilistic sensitivity analyses showed that treatment with IR was cost-effective at conventional willingness-to-pay threshold (€40,000 per QALY). Conclusion: Based in this model, IR is a cost-effective option for CLL patients who deserve a second-line treatment.
Background
B-cell chronic lymphocytic leukemia (CLL) is the most common adult leukemia in Western countries with a reported prevalence of 27 cases per 100,000 inhabitants [1] and a median age at diagnosis of 68 years in Southern Europe [2] . Patients receiving therapy can now expect disease-free intervals of around 2 years after first-line treatment [3, 4, 5], however, recurrence is still the rule. Furthermore, CLL has frequently become refractory to conventional chemotherapy. All these factors combined make it difficult to choose a safe and successful second-line treatment choice. Idelalisib is an oral selective inhibitor of phosphatidylinositol 3-kinases delta isoform recently approved, in combination with Rituximab (IR), for CLL patients with a relapsed or refractory disease (R/R) [6] and naïve patients carrying 17p deletion or TP53 mutations. Current guidelines and expert consensus recommend IR as a suitable therapeutic option in the second-line setting [7, 8]. In this subset of patients other therapeutic options are also recommended and approved in Italy so far as June 2015, such as bendamustine-rituximab (BR) and fludarabine- cyclophosphamide-rituximab (FCR). However, the above therapeutic options have not been compared in head-to-head studies while indirect comparisons with network meta-analyses [9] might be biased by heterogeneous patient selection. Moreover, the relative cost-effectiveness of IR as compared with the several available treatment options has never been attempted. Therefore, we aimed at estimating the incremental costs and benefits of IR as compared with the commonly prescribed treatments for R/R CLL in the perspective of the Italian HealthCare System. The objective of our study was to inform physicians and decision makers of the incremental costs and quality-adjusted life years of this first-in-class drugby adopting “solid” comparator treatments, including chemoimmunotherapy, and full treatment strategies, that is second-and-third line therapy sequences planned to build a decision model for tracking different treatment sequences including IR in either as a second or a third-line treatment. While the national agencies were evaluating the value for money of this new technology, we used a treatment sequence Markov model to estimate, from the perspective of the Italian HealthCare System, the cumulative health benefits and costs of second to third-line treatment sequences including IR as compared with other commonly prescribed treatments for R/R CLL.
Methods
Analytical Framework
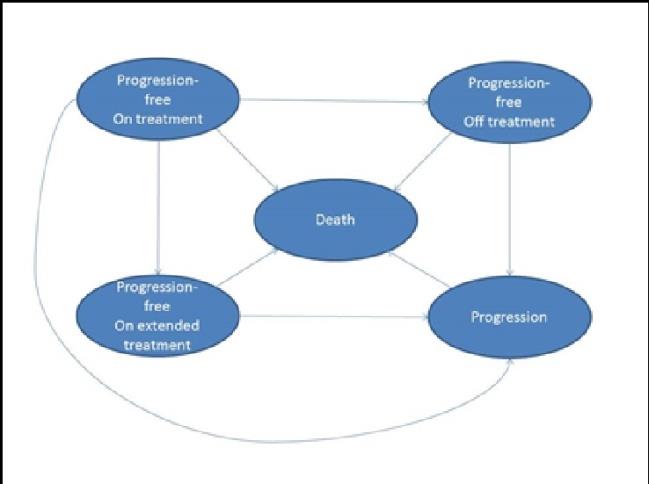
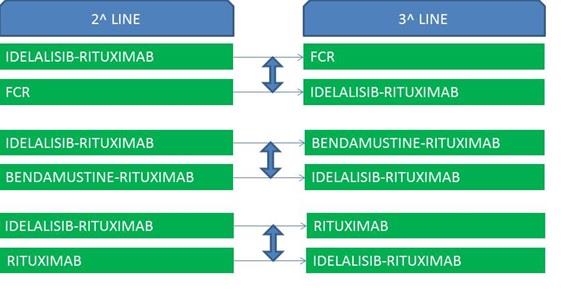
A decision-analytic model was developed with TreeAgePro™ 2015. The model was based on a Markov model framing the natural flow of patients through 5 mutually exclusive health states (Figure 1): (i) progression-free On treatment, (ii) progression-free On extended therapy (idelalisib only), (iii) progression-free Off treatment, (iv) Progression (3rd line therapy), (v) Death. Patients could “move” monthly from one health- state to another, (i.e. cycle, according to input transition probabilities). All patients enter the model in the state “Progression-free On treatment” and receive second- line treatment with one of the four alternative therapies (IR, R, FCR, BR). Patients receiving second-line treatment with IR and not experiencing disease progression during the first 6 months move to the state “Progression-free On extended treatment”. Patients receiving second-line treatment with R, FCR or BR and not experiencing disease progression during treatment move to “Progression-free Off treatment”. It was assumed that patients progressing after 2nd line treatment with IR would possibly start a 3rd line active treatment with the standard therapy being compared with IR. Similarly, patients progressing after 2nd line treatment with standard therapy would possibly cross- over to IR at progression (Figure 2). Patients progressing during or after 3rd line treatment were assigned to palliative sub-continuous chlorambucil.
We retrieved through PubMed all the randomized studies published in the last 5 years (up to march 2016) reporting progression-free survival (PFS) and a detailed description of the frequency of adverse events for R/R CLL patients treated with IR, R, FCR or BR. Phase 2 studies were retrieved if no randomized study addressed the target treatment and setting. We therefore derived data from 2 randomized studies enrolling patients with a median of 3 [6, 12], and 1 [10] previous treatment lines and from one phase II study [11] enrolling patients with a median of 2 previous treatments. We aimed at comparing the selected treatments in patient’s candidates for 2nd line therapy, however, the median number of prior treatment lines in the selected studies was heterogeneous. Therefore, we adopted the hazard ratio of progression according to the treatment line as reported by a large population- based study in the Netherlands [13] and from a randomized trial [14]: a hazard ratio of 1.4 per each further treatment line after the second was therefore used and the resulting transition probabilities are reported in Table 1.
Treatments
Patients were assigned to treatment with IR or one of 3 comparator therapies: R, BR, FCR. The modeled treatment regimens, according to the trial reports, were: a. IR: Idelalisib 150 mg bid plus intravenous rituximab
375 mg/m2 followed by rituximab 500 mg/m2 every Probabilities Data Value Standrd Deviation Source Progression-freeProgression -- IR 1-8 mo 0.020 (4rd line) 0.009 0.005 [6, 12] -- IR >8 mo 0.034 (4rd line) 0.015 0.005 [6, 12] -- R 0.090 (4rd line) 0.039 0.01 [6, 12] -- RB 0.042 (3rd line) 0.028 0.005 [11] -- FCR 0.030 (3rd line) 0.02 0.005 [10] Treatment-related mortality 0.005 0.001 [10, 11] General mortality 0.0033 0.0001 [15] Mortality after progression 0.045 0.005 [13, 14]
2 weeks for 4 doses and then every 4 weeks for 3 doses, for a total of 8 infusions [6]. b. R: intravenous rituximab 375 mg/m2 followed by rituximab 500 mg/m2 every 2 weeks for 4 doses and then every 4 weeks for 3 doses, for a total of 8 infusions [6]. c. FCR: six 28-day cycles including intravenous fludarabine 25 mg/m2 daily for 3 days, intravenous cyclophosphamide 250 mg/m2 daily for 3 days, rituximab 500 mg/m2 on day 1 (except for the 1st cycle during which rituximab dose was split to 50 mg/m2 on day 1plus 450 mg/ m2 on day 3) [10]. d. BR: six 28-day cycles including bendamustine 70 mg/ m2 on days 1 and 2 and intravenous rituximab 500 mg/m2 on day 1 (except for the 1st cycle for which a 375 mg/m2 dose is used) [11].
Progression-Free and Overall Survival
Treatment-related mortality was adopted from two studies enrolling patients with 1 or 2 previous treatment lines [10, 11] and was assumed to be the same for all the compared treatments. Mortality after progression was 0.045 per cycle [13, 14]. General mortality was derived from Italian 2013 life tables [15]. The weighted average life expectancy of the modelled target population, i.e. 68 year old with a male to female ratio of 1.8 [6, 10, 11], was calculated to be 18.25 years: monthly probability of death was estimated according to an exponential model.
Adverse Events
The model considered only febrile neutropenia and the most relevant and specific grade 3-4 adverse events: neutropenia, thrombocythopenia, anemia, diarrohea. The frequencies of adverse events were applied directly from original studies without any adjustment for the median number of previous treatment lines (Table 2). The overall rate of adverse event was equally distributed among treatment cycles, assuming that the whole treatment regimen was completed.
| Event | IR | BR | FCR | R | Cost | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Febrile neutropenia | 30% | 13% | 12% | 22% | 2,956 | ||||||||||||
| Grade 3-4 neutropenia wo fever | 4% | 10% | 59% | 0% | 510 | ||||||||||||
| Grade 3-4 thrombocythopenia | 10% | 28% | 15% | 16% | 1,994 | ||||||||||||
| Grade 3-4 anemia | 4% | 17% | 15% | 14% | 1,322 | ||||||||||||
| Grade 3-4 diarrohea | 4% | 0% | 0% | 0% | 416 |
Table 1: Rates [6,10,11] and unit costs [18] of modelled adverse events.
Costs
The base-case analysis was conducted from the perspective of the national Italian health care system. Costs for drugs, intravenous administration, hospitalisations, out patients resources and management of adverse events were considered. Ex- factory prices for the year 2015 were used for rituximab and idelalisib (Table 3). Since fludarabine, cyclofosphamide and bendamustine, in Italy, are not reimbursed to hospitals on top of day-hospital tariffs, their cost was not considered in the simulation, as already captured by drug administration costs. We assumed that drug dose was always approximated to the next whole vial dose and no waste occurred. Mean charge for intravenous drugs administration was assigned the cost estimated by a large retrospective study conducted in 19 Italian hematology units [16]. The consumption pattern of outpatient resources (visits, medication, diagnostic exams, etc) was based on expert opinion of the clinicians participating in this analysis and was valued at national tariffs [17]. The costs for management of adverse events were derived from an Italian study [18] (Table 2). The cost of 3rd line therapy was calculated based on the portion of patients assigned to IR, R, BR, FCR or chlorambucil. In order to estimate cost of 3rd line idelalisib therapy, we needed to estimate the duration of idelalisib therapy in this setting, therefore we ran the model for a 3rd line setting simulation and calculated that it was 18 months.
| Unit | Cost (€) | S | tandard Deviation | Source | |||||||
| Idelalisib 150 mg (1 tablet) | 66,67a | 10 | [17] | ||||||||
| Rituximab 100 mg (1 vial) | 277,00 a | 50 | [17] | ||||||||
| Administration of ev drugs | 288,00 | 50 | [16] | ||||||||
| Number of intravenous drug administrations in day hospital setting | [6,10,11] | ||||||||||
| n R | |||||||||||
| n BR | 8 | ||||||||||
| n IR | 13 | ||||||||||
| n FCR | 8 | ||||||||||
| 18 |
Table 2: Therapy costs.
aEx-factory price (VAT excluded) Table 3: Therapy costs.
Utilities
Utilities for disease-related health states and tolls for adverse events were derived from a high-quality study conducted in the UK applying standard-gamble interviews [19] (Table 4). Utility for patients on 2nd line therapy was assumed to equal those of progression-free patients, except decrements due to adverse events (pneumonia, diarrohea, anemia).
| Temporary | ||||||||
|---|---|---|---|---|---|---|---|---|
| Health state | Utility | |||||||
| Disutility | ||||||||
| Progression-free | 0.84 | |||||||
| Progressed disease | 0.65 | |||||||
| Febrile neutropenia | -0.2 | |||||||
| Diarrohea | -0.08 | |||||||
| Anemia | -0.09 |
Table 3: Heath state utilities [19].
Distributions
Beta-distributions represented uncertainty for probabilities, rates and utilities, while gamma distributions were used for costs. Time horizon and discount rate: A time horizon of 360 months (30 years) was chosen for base-case analysis. A yearly discount rate of 3% was used for both costs and benefits earned in the future, to calculate their present value [20].
Analysis
According to the quality standards for cost- effectiveness analyses [12], we ran a baseline analysis and calculated incremental costs, incremental quality- adjusted life years (QALYs) and the ratio between the two, i.e. incremental cost-effectiveness ratio (ICER). We also conducted first-order sensitivity analyses for all the input variables. Finally, a Monte-Carlo analysis (200 samples, 500 trials) was run and acceptability curves were plotted. The analysis was run through TreeAge Pro 2015 ™.
Results
Base-case analysis
The results of the model show that patients’ expected life expectancy ranged from 3.09 to 5.34 life years and from 2.31 to 4.22QALYs depending on the strategy being considered (Table 5). Second line treatment with IR was estimated to prolong life expectancy by 1.01- 2.25 life years per patient and to improve outcomes by 0.86-1.91 QALYs per patient, as compared with second- line treatment with FCR or R, respectively. The cumulative discounted lifetime health-care costs ranged from €113,482 to €139,281. The incremental cost per QALY-gained with second-line IR treatment was €2,993, €16,045 and €28,045 compared with second-line treatment with R, BR and FCR, respectively.
| y | Quality- | ) | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lifetime | ) | I | ncrementa | l | c | Incremental | o | |||||||||||||
| Therapeutic | Undiscounted life | adjusted life | Incremental costs | |||||||||||||||||
| Costs per | QALYs per | ost-utility rati | ||||||||||||||||||
| strategy | years per patient | ears (QALYs | per patient (€) | |||||||||||||||||
| patient (€ | patient | (€) | ||||||||||||||||||
| per patient | ||||||||||||||||||||
| FCRIR | 4.33 | 3.36 | 113,482 | |||||||||||||||||
| IRFCR | 5.34 | 4.22 | 137,561 | 0.86 | 24,079 | 28,045 | ||||||||||||||
| BR IR | 3.68 | 2.81 | 116,657 | |||||||||||||||||
| IR BR | 5.34 | 4.22 | 139,281 | 1.41 | 22,623 | 16,045 | ||||||||||||||
| RIR | 3.09 | 2.31 | 131,299 | |||||||||||||||||
| IR R | 5.34 | 4.22 | 137,016 | 1.91 | 5,717 | 2,993 |
Table 4: Baseline analysis.
Sensitivity Analysis
Several one-way sensitivity analyses were run, the most relevant ones being reported in Table 6 and Table 7. The ICER was not sensitive to quality of life adjusting factors, to a reasonable variation of costs related to adverse events and to discounting. The ICER was not sensitive to patients’ age, for ranges between 58 and 78 years. Even survival after progression did not influence the relative cost-effectiveness of IR versus the comparators. Rather, the ICER was sensitive, as expected, to variations of idelalisib unit cost and time horizon, being the ratio more favorable in the long-term run rather than in a short time frame. The results were also sensitive to the duration of idelalisib treatment, which is shorter than PFS, but is a very context- dependent variable, which should be assessed also outside clinical trials. The ICER was also sensitive to relevant variations of the proportion of patients being treated with IR at cross-over, i.e. third-line. The acceptability curve of IR versus FCR and BR (Figure 3) showed that the ICER was lower than the accepted Italian threshold of €40,000/QALY in 67% and 97% of the simulations, respectively [20].
| Baseline | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Range | ICER (€/QALY gained) | ||||||||||
| (€/QALY) | |||||||||||
| Parameter | Lower | Upper | Lower | Upper | |||||||
| Idelalisib unit cost | -30% | +30% | -1,201 | 33,290 | 16,045 | ||||||
| Time horizon | 60 months | 360 months | 46,989 | 16,045 | 16,045 | ||||||
| Median duration of idelalisib treatment (after cross-over) | 10 months | 30 months | 21,323 | 209 | 16,045 | ||||||
| Cross-over portion | 40% | 60% | 18,574 | 3,515 | 16,045 | ||||||
| Febrile neutropenia IR | 12% | 30% | 15,714 | 16,045 | 16,045 | ||||||
| General mortality | 0.0025/month | 0.007/month | 15,146 | 16,193 | 16,045 | ||||||
| Mortality after progression | 0.03/month | 0.06/month | 15,382 | 16,716 | 16,045 |
Table 5: Ranges for parameters and effect on ICER for one-way sensitivity analysis. IR versus BR.
| Baseline | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Range | ICER (€/QALY gained) | ||||||||||
| (€/QALY) | |||||||||||
| Parameter | Lower | Upper | Lower | Upper | |||||||
| Idelalasib unit cost | -30% | 30% | -585 | 56,674 | 28,045 | ||||||
| Time horizon | 60 months | 360 months | 109,624 | 28,045 | 28,045 | ||||||
| Median duration of idelalisib treatment (after cross-over) | 10 months | 30 months | 36,369 | 3,069 | 28,045 | ||||||
| Cross-over portion | 40% | 60% | 48,007 | 8,082 | 28,045 | ||||||
| Febrile neutropenia | 12% | 30% | 27,501 | 28,045 | 28,045 | ||||||
| General mortality | 0.0025/month | 0.007/month | 25,585 | 40,202 | 28,045 | ||||||
| Mortality after progression | 0.03/month | 0.06/month | 27,250 | 29,001 | 28,045 |
Table 6: Ranges for parameters and effect on ICER for one-way sensitivity analysis. IR versus FCR.
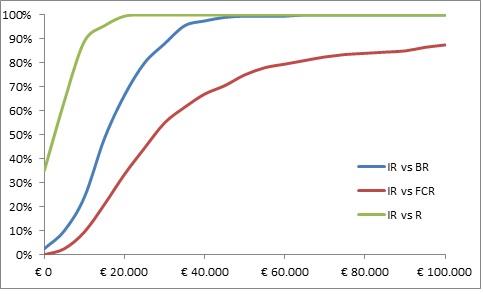
Note: the graph plots on the Y-axis the probability of achieving and ICUR lower than the €/QALY one reported on the X-axis.
Discussion
A wide series of treatments is recommended for R/R CLL [8]. However, which treatments provide reasonable value for money in the specific clinical and economic setting is still to be ascertained. This issue is expected to second-line treatments that are most commonly adopted in Italy, namely BR and FCR as well as with R, which was the control arm of IR in the reported randomized trial. The model estimated that the introduction of IR in second line setting would prolong life expectancy by up to 2 years per patient at an incremental cost that is much lower than €40,000 per QALY gained. The results of our analysis are in line with other economic analyses which were held in Portugal, France, Scotland, England and Canada and that also supported the favorable cost-effectiveness of IR as compared with R, BR, FCR [24, 25, 26, 27, 28]. The results of the present study are also consistent in terms of cost/QALY with the reported cost for value of other anti-leukemic agents [29], since innovative treatments for blood cancers provide a reasonable value for money is achieved so long as treatments prevent future treatment lines and avoid toxicities [30]. Moreover, the higher the number of approved drugs, even belonging to the same class, the higher the survival benefit cancer patients achieve [31]. The present study, however, has several limitations. The treatment-related mortality was assumed to be the same for all the compared regimens without considering the benefit of IR as compared to R in terms of overall survival [6]. Furthermore, in the base-case analysis, it was assumed that only 50% of the patients who progressed after second-line treatment were eligible to receive a third-line therapy, while the other half moved to palliative chlorambucil; results, though, were not sensitive to even wide variations of those percentages. Another limitation was that the frequency of adverse events was not adjusted according to the treatment line, while the rates observed in heavily pre- treated patients might be overestimated. Utilities were derived from a British population, thus possibly not reflecting utility values of Italian CLL patients. However, the results in terms of life years are in line with those of QALYs. Furthermore, the model did not include all the possible therapeutic options which have been studies in relapsed/refractory CLL: in particular, another BTK- inhibitor, ibrutinib, was not included in the simulation because it was not available in Italy by the time the model was developed and could not considered a “standard of care” to be compared with novel drugs, i.e. idelalisib [32]. The present study also addressed a limited sequence of treatments, mainly second and third-line therapy; however, this was aimed at keeping the model more transparent. Finally, the results of the analysis were obtained from the perspective of the Italian health care system, without taking into account possible indirect costs related to lost productivity of CLL patients and their caregivers. We expect that the economic value of IR as compared to the other treatments would be even more favorable in the societal perspective, since idelalisib is an oral treatment.
Conclusion
This study aimed at investigating the relative cost- for-benefit of different treatment options for R/R CLL, including idelalisib, the novel oral inhibitor of phosphatidylinositol 3-kinases delta. The findings of our research showed that treatment with IR for CLL patients who relapsed after or were refractory to first-lines therapies is a cost-effective option in the Italian healthcare setting as compared to the second-line treatments that are most commonly adopted in Italy.
Funding
The study was funded by Gilead Sciences.
Authors’ contributions
MaM conceived the model and ran the analyses. MoM, CA and MFR contributed in selecting clinical studies of progression-free survival after different treatments and contributed to writing the paper (introduction section). Marchetti M and PMP provided the unit cost data for the model and revised the final model.
Competing interests
The study was supported by a grant from GILAD Italy. Marchetti M and PMP were an employees of Gilead Italy at the time of the research.
References
-
(2015) Orphanet: Prevalence of rare diseases: Bibliographic data. Paris: Orphanet.
-
Sant M, Allemani C, Tereanu C, De Angelis R, Capocaccia R, et al. (2010) Incidence of hematologic malignancies in Europe by morphologic subtype: results of the HAEMACARE project. Blood 116(19): 3724-3734.
-
Hallek M, Fischer K, Fingerle-Rowson G, Fink AM, Busch R, et al. (2010) Addition of rituximab to fludarabine and cyclophosphamide in patients with chronic lymphocytic leukaemia: a randomised, open-label, phase 3 trial. Lancet 376(9747): 1164- 1174.
-
Hillmen P, Gribben JG, Follows GA, Milligan D, Sayala HA, et al. (2014) Rituximab plus chlorambucil as first-line treatment for chronic lymphocytic leukemia: final analysis of an open- label phase II study. J Clin Oncol 32(12): 1236- 1241.
-
Goede V, Fischer K, Busch R, Engelke A, Eichhorst B, et al. (2014) Obinutuzumab plus chlorambucil in patients with CLL and coexistent conditions. N Engl J Med 370(12): 1101-1110.
-
Furman RR, Sharman JP, Coutre SE, Cheson BD, Pagel JM, et al. (2014) Idelalisib and rituximab in relapsed chronic lymphocytic leukemia. N Engl J Med 370(11): 997-1007.
-
Eichhorst B, Robak T, Monserrat E, Ghia P, Hillmen, et al. (2015) Chronic lymphocytic leukaemia: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 26(5): 78-84.
-
Zelenetz AD, Gordon LI, Wierda WG, Abramson JS, Advani RH, et al. (2015) Chronic lymphocytic leukemia/small lymphocytic lymphoma, version 2.2015. J Natl Compr Canc Netw 13(3): 326-362.
-
Ladyzynski P, Molik M, Foltynski P (2015) A network meta-analysis of progression free survival and overall survival in first-line treatment of chronic lymphocytic leukemia. Cancer Treat Rev 41(2): 77-93.
-
Awan FT, Hillmen P, Hellmann A, Awan FT, Hillmen P, et al. (2014) A randomized, open-label, multicenter, phase 2/3 study to evaluate the safety and efficacy of lumiliximab in combination with fludarabine, cyclophosphamide and rituximab versus fludarabine, cyclophosphamide and rituximab alone in subjects with relapsed chronic lymphocytic leukemia. Br J Haematol 167(4): 466- 477.
-
Fischer K, Cramer P, Busch R, Stilgenbauer S, Bahlo J, et al. (2011) Bendamustine combined with rituximab in patients with relapsed and/or refractory chronic lymphocytic leukemia: a multicenter phase II trial of the German Chronic Lymphocytic Leukemia Study Group. J Clin Oncol 29(26): 3559-3566.
-
Sharman JP, Coutre SE, Furman RR, Cheson BD, Pagel JM, et al. (2014) Second Interim Analysis of a Phase 3 Study of Idelalisib (ZYDELIG®) Plus Rituximab (R) for Relapsed Chronic Lymphocytic Leukemia (CLL): Efficacy Analysis in Patient Subpopulations with Del(17p) and Other Adverse Prognostic Factors. American Society of Hematology 2015 Meeting. Blood 124: 330.
-
Holtzer-Goor KM, Bouwmans-Frijters CA, Schaafsma MR, de Weerdt O, Joosten P, et al. (2014) Real-world costs of chronic lymphocytic leukaemia in the Netherlands. Leuk Res 38(1): 84-90.
-
Robak T, Dmoszynska A, Solal-Céligny P, Warzocha K, Loscertales J, et al. (2010) Rituximab plus fludarabine and cyclophosphamide Prolongs Progression-Free Survival Compared with Fludarabine and Cyclophosphamide alone in previously treated chronic lymphocytic leukemia. J Clin Oncol 28(10): 1756-1765. $$ http://dati.istat.it/?lang=en&SubSessionId=69f1ab e2-7797-4632-908c-fb264c3a606f&themetreeid=- 200 $$
-
Pasdera A (2013) I costi standard dei ricoveri in Ematologia, Società Italiana di Ematologia, Il Sole 24 ore Sanità, 6-7.
-
(2013) Remunerazione delle prestazioni di assistenza ospedaliera per acuti, assistenza ospedaliera di riabilitazione e di lungodegenza post acuzie e di assistenza specialistica ambulatoriale. Supplemento ordinario alla ‘Gazzetta Ufficiale’ n. 23 del 28 gennaio – Serie generale
-
Capri S, Morabito A, Carillio G, Grossi F, Longo R, et al. (2007) Valutazione economica di erlotinib, docetaxel e pemetrexed nel trattamento di seconda linea del carcinoma polmonare non a piccole cellule. PharmacoEconomics - Italian Research Articles 9(2): 113-124.
-
Beusterien KM, Davies J, Leach M, Meiklejohn D, Grinspan JL, et al. (2010) Population preference values for treatment outcomes in CLL: a cross- sectional utility study. Health and Quality of Life Outcomes 8: 50.
-
Fattore G (2009) Proposta di linee guida per la valutazione economica degli interventi sanitari in Italia. Pharmacoeconomics-Italian Research Articles 11(2): 83-93.
-
Greenberg D, Earle C, Fang CH, Eldar-Lissai A, Neumann PJ (2010) When is cancer care cost- effective? A systematic overview of cost-utility analyses in oncology. J Natl Cancer Inst 102(2): 82- 88.
-
Blankart CR, Koch T, Linder R, Verheyen F, Schreyögg J, et al. (2013) Cost of illness and economic burden of chronic lymphocytic leukemia. Orphanet Journal of Rare Diseases 8: 32.
-
O’Brien SM, Lamanna N, Kipps TJ, Flinn I, Zelenetz AD, et al. (2015) A phase 2 study of idelalisib plus rituximab in treatment-naïve older patients with chronic lymphocytic leukemia. Blood 126: 2686- 2694.
-
Leleu H, Blachier M, Mealing S, Baujat C, Perard R, et al. (2015) Cost-effectiveness of idelalisib plus rituximab in chronic lymphocytic leukemia. PCN 173. Value Health 18: A460.
-
Gouveia M, Silva MG, Alarcao J, Fiorentino F, Carda J, et al. (2015) Cost-effectiveness of idelalisib in combination with rituximab for the treatment of relapsed/refractory chronic lymphocytic leukemia (CLL) in Portugal. Value Health 18(7): A461-462.
-
Kumar G, Morton TD, Padhiar A, Marsh R, Perard R (2015) A Scotland based cost-effectiveness analysis of idelalisib (Zydelig®) in combination with rituximab for the treatment of adults with chronic lymphocytic leukemia (CLL). Value Health 18(7): A455.
-
Sullivan W, Hadlow S, Perard R, Lealing S, Cox L, et al. (2015) The cost-effectiveness of idelalisib in chronic lymphocytic leukemia in England and Wales. Value Health 18(7): A454-455.
-
Yu JS, Seal B, Carlson JJ (2015) IdelalisibPlus Rituximab Versus Placebo Plus Rituximab For Relapsed Chronic Lymphocytic Leukemia: A Cost- Effectiveness Analysis. Value in Health 18: A203.
-
Marsh K, Xu P, Orfanos P, Benedict A, Desai K, et al. (2014) Model-based cost-effectiveness analyses for the treatment of chronic lymphocytic leukaemia: a review of methods to model disease outcomes and estimate utility. Pharmacoeconomics 32(10): 981- 993.
-
Marchetti M (2016) Value of innovation for hematologic malignancies. J Med Econ 19(5): 487- 489.
-
Lichtenberg FR (2015) The impact of pharmaceutical innovation on premature cancer mortality in Canada, 2000-2011. Int J Health Econ Manag 15(3): 339-359.
-
Ysebaert L, Philip BP, Stilgenbauer S (2015) Real- world treatment patterns of Rituximab usage as single-agent therapy or part of combination regimens in chronic lymphocytic leukemia (CLL) in EU5 countries (UK, France, Germany, Italy, and Spain). PSY63. Value in Health 17: A234.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies