Cutaneous Gamma Delta T cell Lymphoma Leading to Hemophagocytic Lymphohistiocytosis that Presented as Posterior Reversible Encephalopathy Syndrome
Cutaneous Gamma Delta T cell Lymphoma (CGDTCL) is an extremely rare and aggressive disease arising from immature T cells with gamma delta T cell receptors. CGDTCL can result in a life-threatening syndrome called Hemophagocytic Lymphohistiocytosis (HLH). HLH is a syndrome of fevers, cytopenia and multiorgan failure resulting from excessive immune activation. Early diagnosis of HLH is vital as a delay in diagnosis/treatment may result in grave outcomes. Our patient presented with Posterior Reversible Encephalopathy Syndrome (a syndrome characterized by headache, confusion, seizures and visual disturbance) prior to the diagnosis of HLH.
Case Presentation
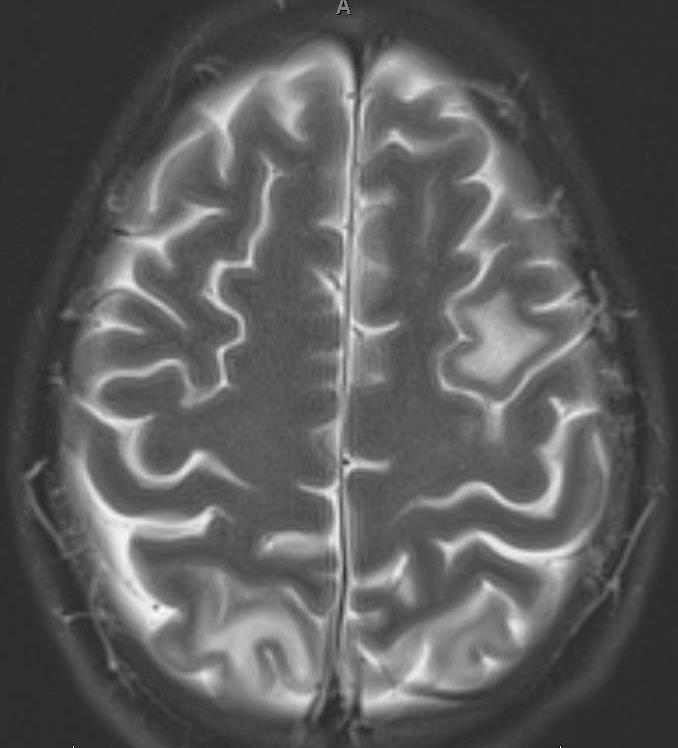
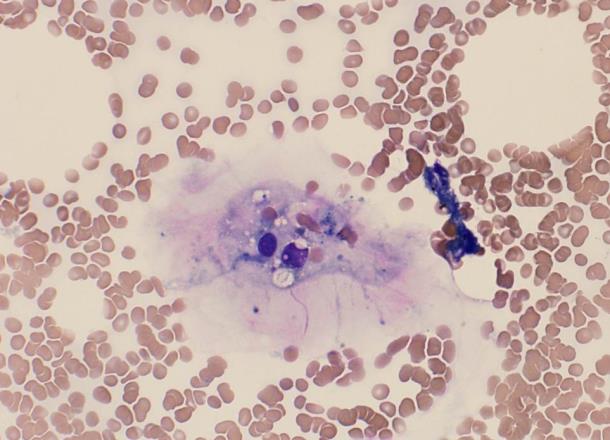
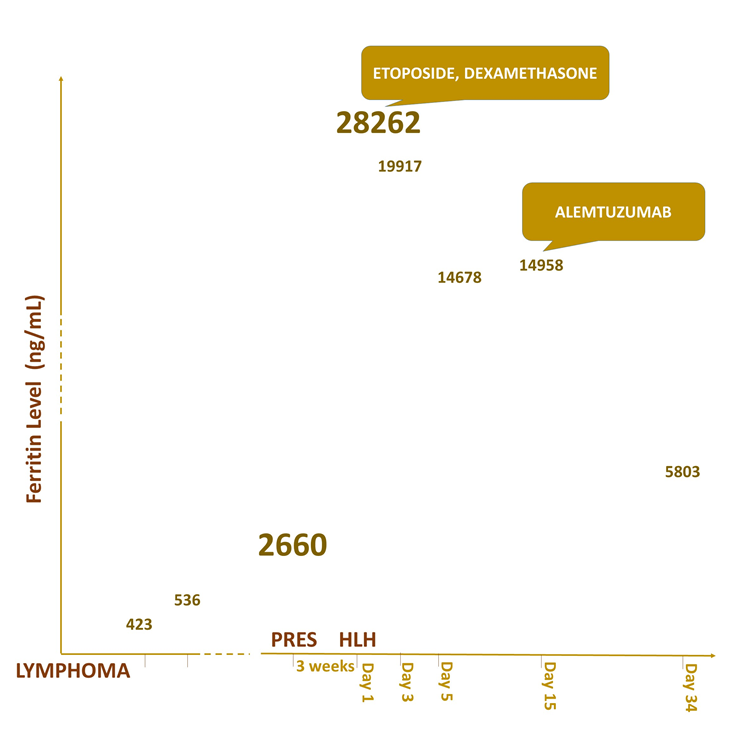
31-year-old man with medical history of vitiligo was diagnosed with cutaneous gamma delta T cell lymphoma when he presented with a skin rash to his PCP. He failed standard therapy and was started on a clinical trial with CPI-613 and Bendamustine. Treatment was complicated by prolonged myelosuppression. Three months later, he was admitted to the Medical ICU for headaches and status epilepticus. MRI Brain revealed multifocal areas of cortical and subcortical edema without contrast Cutaneous Gamma Delta T cell Lymphoma Leading to Hemophagocytic Lymphohistiocytosis that Presented as Posterior Reversible Encephalopathy Syndrome enhancement or hemorrhage consistent with PRES of unknown etiology (Figure 1). As there was no evidence of CNS infection or CNS lymphoma, he was discharged a week later after ensuring clinical stability. Ferritin level checked at that time was 2660. Three weeks later, patient presented to the emergency department with fever and pancytopenia. On presentation, notable labs included WBC- 2.4, Hg-5.5, platelets-22, Na- 128, K- 3.7, creatinine- 2.4 (baseline- 0.9), alkaline phosphatase- 900, AST-300, ALT-108, LDH -2800, ferritin-28262. Under high suspicion for HLH, an urgent bone marrow biopsy (Figure 2) was done and patient was immediately started on dexamethasone and etoposide. Bone marrow biopsy revealed multiple hemophagocytic histiocytes containing predominantly ingested red blood cells and erythroid Haematol Int J
precursors. His H score was 249 with 99.3 % probability of HLH (Figure 3). Patient was also given a dose of alemtuzumab and transferred to bone marrow service for possible allogenic transplantation (Table 1). As patient became progressively more deconditioned with intractable nausea, vomiting, and failure to thrive, patient and family decided to go home with hospice and unfortunately, patient died 2 months after discharge [1, 2, 3, 4, 5].
| H score | PRES | HLH | ||||||
|---|---|---|---|---|---|---|---|---|
| Known Immunosuppression | Yes | Yes | ||||||
| Maximum Temperature | 104.2 | 102.5 | ||||||
| Hepatomegaly | Yes | Yes | ||||||
| Splenomegaly | Yes | Yes | ||||||
| Hemoglobin | 11.3 | 9.6 | ||||||
| WBC | 22.3 | 2.7 | ||||||
| Platelet | 252 | 15 | ||||||
| Ferritin | 2660 | 28262 | ||||||
| Triglycerides | 258 | 331 | ||||||
| Fibrinogen | No data | Present | ||||||
| SGOT/SGPT | <30 | >30 | ||||||
| Hemophagocytes on BM | No data | Present | ||||||
| Sodium | 128 | 129 | ||||||
| H score | 168 | 271 | ||||||
| Probability of HLH | 50% | 99.8% |
Table 1: H Score.
Discussion
Cutaneous T cell Lymphoma has been shown to increase the risk of HLH. Any patient with T cell lymphoma, presenting with fever and pancytopenia, should raise the suspicion of HLH as high index of suspicion is key in diagnosing this aggressive disease. Checking ferritin levels early-on would give us a clue in including HLH in our differential. Previous research [1, 2, 3, 4] has shown that PRES could be a complication of treatment for HLH, but our patient developed PRES before diagnosis of HLH. Further studies must be done to analyze the cause/effect relationship between PRES and HLH. It is reasonable to calculate an H score at the time of diagnosis of PRES in patients with lymphoma or other immunosuppressive disorders to guide clinicians with next best steps in diagnosing this life-threatening disease.
References
-
Gibson JF, Kapur L, Sokhn J, Xu M, Foss FM (2015) A fatal case of primary cutaneous gamma-delta T cell lymphoma complicated by HLH and cardiac amyloidosis. Clin Case Rep 3(1): 34-38.
-
Thompson PA, Allen CE, Horton T, Jones JY, Vinks AA, et al. (2009) Severe neurologic side effects in patients being treated for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer 52(5): 621-625.
-
Lee G, Lee SE, Ryu KH, Yoo ES (2013) Posterior reversible encephalopathy syndrome in pediatric patients undergoing treatment for hemophagocytic lymphohistiocytosis: clinical outcomes and putative risk factors. Blood Res 48(4): 258-265.
-
Mehta RS, Smith RE (2013) Hemophagocytic lymphohistiocytosis (HLH): a review of literature. Med Oncol 30(4): 740.
-
Kumar S, Rajam L (2011) Posterior reversible encephalopathy syndrome (PRES/RPLS) during pulse steroid therapy in macrophage activation syndrome. Indian J Pediatr 78(8): 1002-1004.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies