Pfizer, Moderna and Janssen vaccine InflammoThrombotic and Prion Type Effect on Erythrocytes When Added to Human Blood
Background: Three EUA approved drug vaccine biologics have been approved for use by the United States Food and Drug Administration (FDA) for SARS-CoV-2. Their effect upon erythrocytes has not previously been reported. Methods: Seven individuals (4 men; 3 women) including two people with prior SARS-CoV-2 infections, one previously vaccinated with the Pfizer vaccine (two doses), and one previously vaccinated with the Moderna vaccine (three doses including one booster) provided blood drawn by venipuncture for analysis. In the first part of the study, one male subjected provided blood by venipuncture analysis. This blood was microscopically analyzed before and after the administration of the Pfizer BioNTech vaccine and normal saline. In the second part of the study, 3 men and 3 women provided blood samples obtained by venipuncture. Each of the individual’s blood was directly examined microscopically before and after administration of the Pfizer, Moderna, and Janssen vaccines to the blood. In the third part of the study the vaccines were independently analyzed for extraneous material. Results: Seven individuals including 4 men and 3 women showed normal erythrocyte coloration when their blood was drawn by venipuncture. Each individual’s blood when analyzed microscopically demonstrated normal morphology and appearance. In each instance, the administration of the Pfizer, Moderna, or Janssen vaccines directly into the blood on peripheral blood smear demonstrated an almost immediate loss of red color. This loss of red color persisted throughout the examination and was only seen where the vaccines mixed with erythrocytes. As the vaccines spread across the blood smear, the erythrocytes demonstrated (a) a loss of red color that was not transient, (b) clumping of erythrocytes not observed during the same time period following the administration of normal saline to the blood, and (c) alterations in the morphology of erythrocytes. While several of the vials had extraneous material; none of them had evidence of significant graphene oxide, living organisms, or nanotechnology. Conclusion: Administration of Pfizer, Moderna, and Janssen vaccines resulted in the immediate loss of red coloration present in erythrocytes. This loss of red coloration indicates that there is a disruption of the hemoglobin binding of oxygen. Since atmospheric oxygen is immediately available to re-saturate the hemoglobin molecules restoring the red color responsible for the function and name of erythrocytes; the results of this investigation suggest that there is an alteration in the hemoglobin molecule preventing the hemoglobin from binding with oxygen. This alteration of the hemoglobin molecule could be explained if the vaccines merge with the erythrocytes and release their genetic material (RNA or DNA) directly into the erythrocytes; having a prion altering effect upon the hemoglobin molecule. Some of the vaccine samples included extraneous materials. The vaccines did not include observable graphene oxide, eggs or living organisms.
Richard M Fleming*, Matthew R Fleming, Rena D Salyer and Kevin W McCairn
Keywords: SARS-CoV-2 vaccines; Pfizer BioNTech; Moderna; Janssen; Erythrocytes; De-saturation; Hemoglobin
Key Points
• Erythrocytes appear red when they are saturated with oxygen. This effect is immediately seen when partially de-saturated blood is exposed to air with oxygen during venipuncture.
• When the Pfizer, Moderna and Janssen vaccines are added to erythrocytes, the erythrocytes begin to lose their red color within 10-15 seconds. This effect increases over a minute where the vaccines have contact with the erythrocytes.
• This de-saturation appears to be permanent with a failure of the erythrocytes to return to their normal red color seen when the hemoglobin molecule combines with oxygen.
• This failure of the hemoglobin molecule to combine with oxygen, present in atmospheric air, suggests an alteration in the hemoglobin molecule resulting in a permanent loss of oxygen carrying capacity and a permanent loss of red color in the exposed erythrocytes.
• Some of the vaccine samples contained extraneous material including crystals, fibrous material and precipitated lipid nanoparticles. They do not appear to have significant graphene oxide, nanotechnology, or biologic organisms; unless the vaccine vials are contaminated.
Introduction
Atmospheric oxygen is 20.946% by volume and 23.14% by weight [1]. This amount of atmospheric oxygen is more than sufficient to re-oxygenate hemoglobin molecules that are partially de-saturated when exposed to atmospheric oxygen. This is demonstrated every day by patients undergoing venipuncture. Consequently, any blood exposed to atmospheric oxygen should immediately re-saturate unless the hemoglobin molecule, responsible for binding to oxygen as the transport mechanism within erythrocytes, is damaged.
Efforts to address the Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) have included the use of Emergency Use Authorization (EUA) [2, 3, 4] drug vaccine biologics designed to elicit an immune response to the virus. While efforts to elicit innate and humoral response to the viruses have primarily focused on T-cells and B-cells; little or no information exists as to the effect upon erythrocytes.
Since erythrocytes are the only non-nucleated cells in the human body and there are approximately 25 trillion erythrocytes in each person composing approximately 80% of the cells in our bodies [5], this investigation looked at the effect of adding these drug vaccine biologics directly to tissue samples of erythrocytes.
Methods
This study was carried out between September and December of 2021. All subjects participated following informed consent. Blood was obtained from each subject by venipuncture, either by butterfly 20-gauge needle for subject 1 or by 18-gauge needle for subjects 2-7. In each instance blood was obtained using syringe aspiration and not vacutainer. Blood samples were not subjected to anti-coagulant or other chemicals. The blood was immediately transferred to glass slides for microscopic examination. Microscopic examination of the peripheral blood smear was then carried out using 20 x to 1500x. Microscopic evaluations of the blood were made following the administration of normal saline, Atropine, Domitor, Pfizer BioNTech, Moderna, and Janssen vaccines; the first three for control purposes. Each of the three vaccines was independently analyzed under the microscope to look for evidence of extraneous material.
During first part of the study subject 1’s blood was microscopic analyzed using a SWIFT Tricular Biological microscope. Opitical recordings were made using a HAYEAR 14 MP HDMI 1080 high definition 30mm/30.5 mm lens. During the second part of the study subjects 2-7 blood was analyzed using a Keyence microscope and recording equipment using a VH-ZST with 20x to 2000x RZ lens. The final part of the investigation included the same microscopic equipment and analysis employed for the first two parts of the study. During this part of the study the vaccines were examined independently. Additional supporting evidence was provided by adding graphene oxide directly to microscopic samples.
Study participants affirmed on videotape that the vaccine samples and all venipuncture materials used in this study were all sealed prior to beginning the study. All vaccines were kept under refrigerated conditions as called for by Pfizer, Moderna and Janssen.
Results
Each of the following images was obtained within minutes of applying the blood and individual vaccines. No changes were made to the optics or software between baseline and vaccine microscopic examination. No changes were made at any time to the acquired video or images between baseline and vaccine microscopic examination.
The first part of this study looked at the blood of a 48-
year old Caucasian male with known history of coronary artery disease (CAD). This subject had recovered from SARS- CoV-2 infection and was unvaccinated. The result of his microscopic analysis is shown in Figure 1.
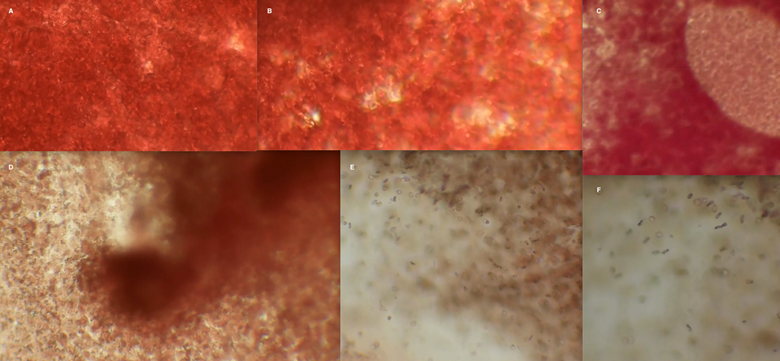
Figure 1: Microscopic examination of erythrocytes, erythrocytes plus normal saline, and erythrocytes plus Pfizer BioNTech. 100x microscopic analysis of subject 1 included analysis of (A) erythrocytes without added saline or Pfizer vaccine, and (B) erythrocytes with addition of normal saline solution to determine if changes in coloration of the erythrocytes were a dilutional effect. Further microscopic analysis following addition of Pfizer BioNTech with changes in erythrocytes seen at 30-seconds (C), and 1-2 minutes (D, E, F). Erythrocyte coalescence is seen in (E) and (F). Sequential imaging of erythrocytes exposed to normal saline did not reveal coalescence or reduction in red color (B) during this same time period. Images were taken from the recorded video of the investigation.
Figure 1A shows this subjects blood at 40x with expected coloration (red oxygenated erythrocytes) followed by the introduction of normal saline in Figure 1B to look for evidence of changes in color due to dilutional effect. No changes in coloration were seen. The same result was seen when atropine and medetomidine hydrochloride (Domitor) were added as controls. Figure 1C shows a region of blood at 100x following the addition of Pfizer vaccine. There is an almost immediate loss of red color noted within the droplet of vaccine and surrounding tissue.
Several days later blood was again obtained from the subject to compare with the initial results shown in Figure 1A-C. The results shown at 100x demonstrated a reduction in red coloration consistent with reduction in oxygen saturation of the erythrocytes within minutes of application of the Pfizer vaccine to the blood. As shown in Figure 1D-F, there was both a discoloration of the erythrocytes and coalescence of erythrocytes, not seen during the same time period when normal saline was added (Figure 1B).
Given these findings, six additional individuals were recruited and all three of the currently used EUA vaccines for SARS-CoV-2 (COVID-19) were analyzed. Subject 2 is a 50- year old Caucasian female who had recovered from SARS- CoV-2 and is unvaccinated with no known comorbidities. Figure 2 shows her results in the first series of microscopic images. At 200x discoloration of the erythrocytes are seen with the addition of Pfizer. Discoloration is seen with the Moderna vaccine at 50x immediately upon contact with the vaccine. Microscopic analysis at 200 x within the first minutes showed clumping of erythrocytes; not seen with normal saline.
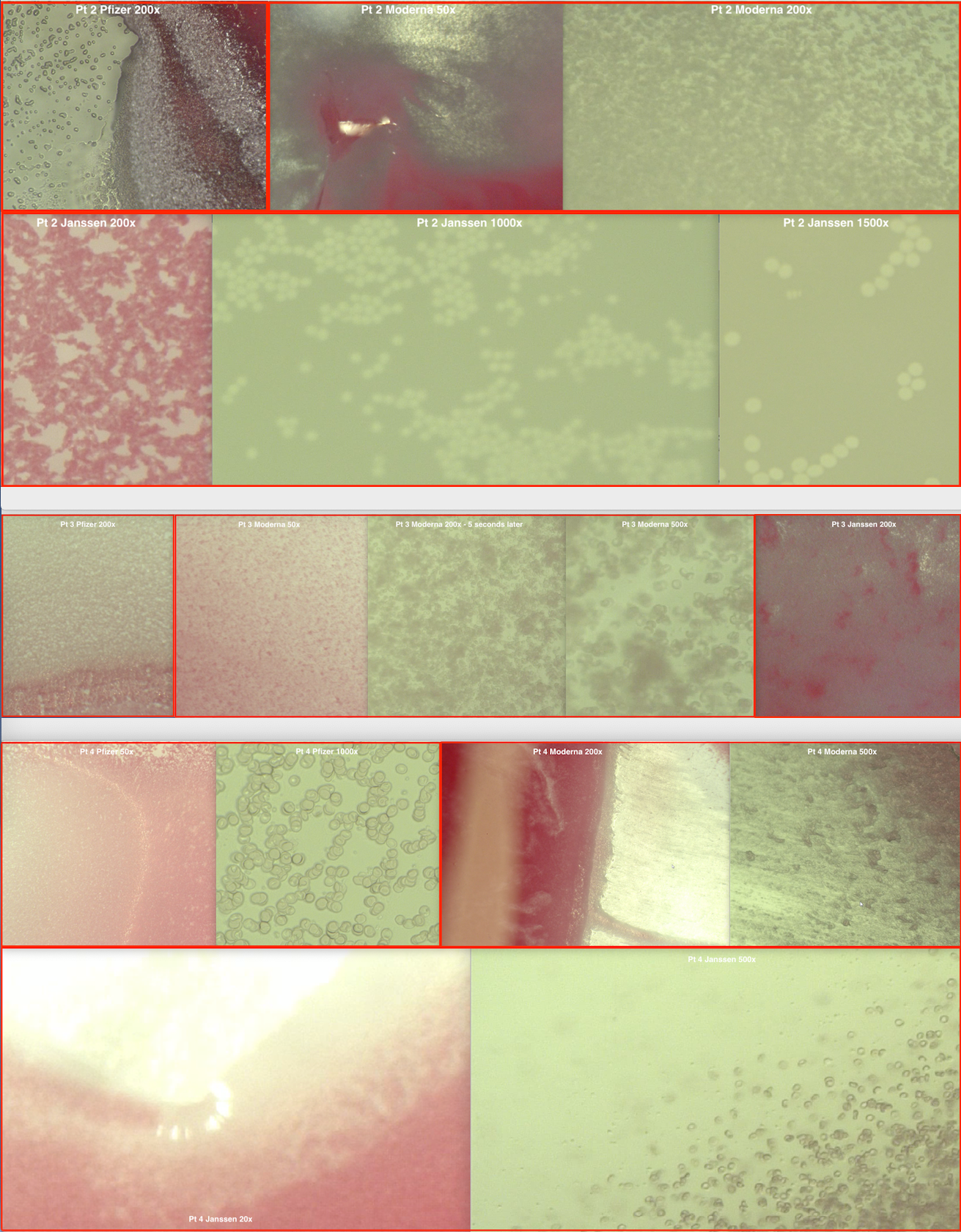
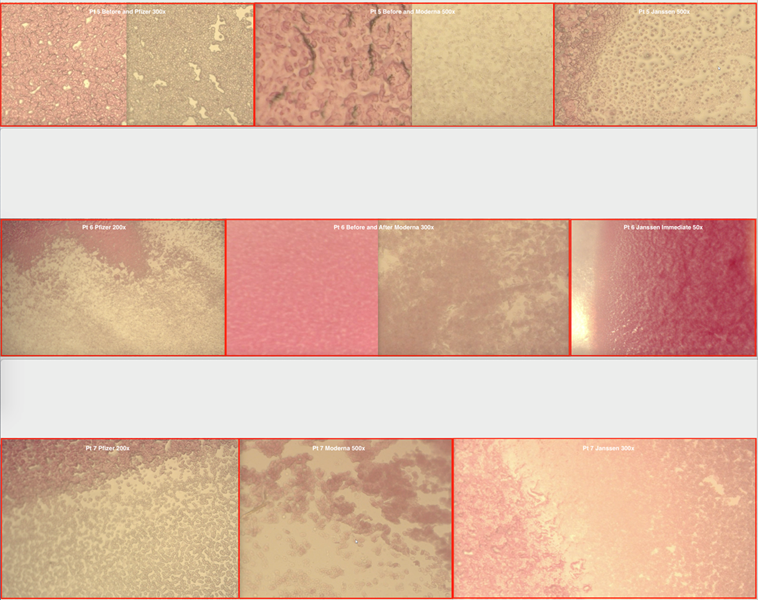
Figure 2: Microscopic examination of erythrocytes in six individuals before and after the addition of Pfizer BioNTech, Moderna and Janssen Ad26.COV2.S vaccines for SARS-CoV-2 (COVID-19). Patients 2 through 7 are each labeled along with the vaccine added and the microscopic power used for each image. Images were taken from the recorded video segments conducted at the time of the investigation. The results of each individual are shown for all three vaccines under powers ranging from 50x to 1500x.
Following the addition of the Janssen vaccine the patient’s blood is seen at 200x with evidence of mild reductions in erythrocyte coloration compared with the Pfizer and Moderna vaccines; however, within the first couple minutes as shown at 1000x and 1500x, the erythrocytes loss their oxygenated red color and began coalescing.
Subject (patient) 3 is a 51-year old African American female with no known comorbidities. She has no documented COVID infection and is unvaccinated. The results of her microscopic examination are shown in the second panel in Figure 2. The first image shows desaturation of erythrocytes when Pfizer was added as seen under 200x. The next three images show the results of Moderna added to her blood; first at 50x and then 5-seconds later when her blood was looked at under 200x. Finally the results under 500x reveal desaturation and clumping of erythrocytes. The final image for this subject showed erythrocyte desaturation at 200x following addition of Janssen Ad26.COV2.S.
The fourth subject is a 62-year old Caucasian male with elevated M-spike on serum protein electrophoresis (SPEP) consistent with possible circulating antibodies with no known SARS-CoV-2 infection. He is not vaccinated. His microscopic results are shown in the third panel of Figure 2. At 50x the initial discoloration of erythrocytes can be seen in the left part of the image where the Pfizer droplet was placed. The second image shows the results under 1000x. The next images show the immediate discoloration of his erythrocytes following administration of Moderna at 200x and 500x power. Immediately below these images are the 20x and 500x discoloration of erythrocytes following administration of Janssen.
Subject 5 is a 56-year old Caucasian female who has not been diagnosed with COVID and who received the first two injections of the Pfizer BioNTech vaccine. Her before and after microscopic results are shown in the fourth panel of Figure 2. To the left are her before and after results following administration of the Pfizer vaccine at 300x. The next microscopic images reveal the before and after results of administering the Moderna vaccine at 500x. The final microscopic image shows the results of Janssen at 500x with the non-vaccinated blood appearing in the left part of the field and the vaccinated region to the right of that. In each case the erythrocytes show desaturation with loss of red coloration.
Subject 6 is a 71-year old Caucasian male who received both original Moderna vaccines and the booster. The results of his microscopic analysis are shown in the fifth panel of Figure 2. To the left is shown the interface between the blood where the Pfizer vaccine has been added to the blood under 200x, with the loss of erythrocyte coloration where the vaccine was added. The middle images show the before and after results at 300x of adding Moderna with erythrocyte discoloration and clumping of erythrocytes. The final microscopic images shows where Janssen was added to the left part of the field at 50x with loss of erythrocyte coloration.
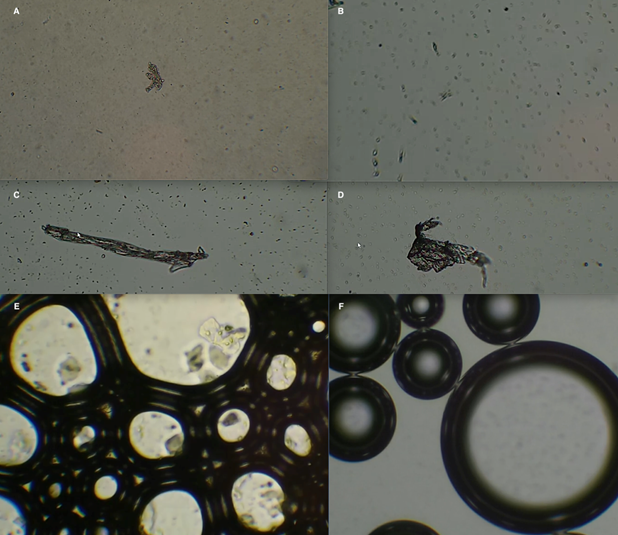
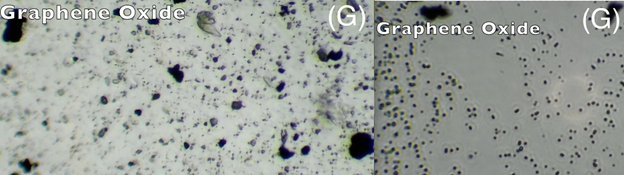
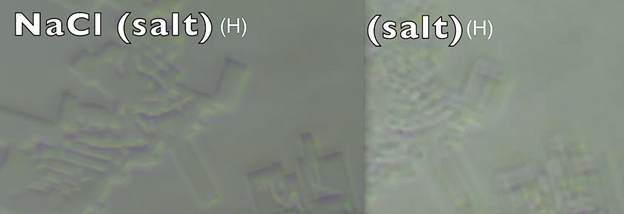
Figure 3: Microscopic examination of Pfizer BioNTech, Moderna and Janssen vaccines. 100x microscopic analysis of the vaccines at 100x revealed evidence of (A, D) crystalline structures, (B, C) fibrous material, (E) lipid nanoparticles trapped in air droplets, and (F) air bubbles coalescence when the slide is tapped. Graphene oxide was independently added (G) to determine what graphene oxide looks like under the microscope. Finally, sodium chloride was added (H) independently and analyzed microscopically. Social media has reported microscopic material identical to “F” and “H” as nanotechnology reportedly being used to track vaccine recipients.
The final subject, subject 7 is a 63-year old Caucasian male with no known comorbidities or prior infection with SARS-CoV-2. He is unvaccinated. His results are shown in the final panel (sixth) of Figure 2. To the left is shown the interface between the blood where Pfizer has not been added (upper left) and the region where the vaccine vials droplet was added. The erythrocytes are desaturated in the region where the vaccine was added. The middle microscopic image shows the interface region where Moderna was added at 500x. The final image shows the interface where the Janssen vaccine was added at 300x.
Figure 3 shows the microscopic examination of all three vaccines from 11 different vials. As shown in Figure 3 there was evidence of extraneous materials in each of the vaccine vials including crystalline structures (A, D), fibrous material (B, C), and precipitating lipid nanoparticles (E). There was no microscopic evidence of microchips, or graphene oxide – which undoubtedly does exist as it is part of the processing of many vaccines. Additionally there was no evidence of living organisms or the ovum of living organisms. While Figure 3 is displayed at 100x, the analysis was carried out to 1000x. Finally, air droplets were seen (F) as would be expected from microscopic wet mounts. When the slide is tapped, these air droplets will coalesce as shown (F). Graphene oxide was added (G) in various concentrations to observe what would be seen if graphene oxide was present in the vaccines. Finally, the appearance of sodium chloride [NaCl] was examined under the microscope (H).
Discussion
Examination of the Pfizer, Moderna, and Janssen vaccines using microscopic settings from 20x to 1500x revealed crystalline and fibrous materials in some but not all samples. There was no significant graphene oxide material present, certainly not 99% of the vaccine material, and there was no evidence of living creatures, eggs, or nanotechnology tracking material proposed in social media reporting. There was evidence of lipid nanoparticles coalescing and precipitating out of solution in some but not all of the Pfizer samples. The prevalence of these extraneous materials in the total vaccine supplies is currently unknown.
Blood obtained by syringe venipuncture technique without the addition of anti-coagulants or other chemical compounds clearly showed oxygenated hemoglobin in erythrocytes prior to the addition of any vaccine. This included both the blood samples themselves and blood samples with the addition of normal saline as shown Figure 1 a and b respectively. The normal saline samples served as controls for dilutional effect upon erythrocyte coloration (oxygen saturation) as well as time required to observe clotting, clumping or coagulation.
In the seven individuals’ studies, the addition of each of the vaccines (Pfizer BioNTech, Moderna, and Janssen) produced desaturation of erythrocytes to varying degrees upon contact; in some instances immediately upon contact. This oxygen desaturation was identified by the loss of red color that is present when the hemoglobin molecule binds with oxygen. The loss of erythrocyte red color is seen with oxygen hemoglobin desaturation and was seen as the vaccines spread through the peripheral blood smears.
The affected erythrocytes remained pale without restoration of their red color once desaturation occurred and persisted throughout the microscopic observation. This loss in red color indicates the loss of ability of hemoglobin to combine with oxygen. Since there is more than adequate oxygen present in atmospheric air to re-saturate erythrocytes, this loss of red color suggests that it is not the absence of available oxygen for binding, but rather, a change in the conformation of hemoglobin resulting in the hemoglobin molecule no longer being able to bind oxygen for transport.
One mechanism that could explain this alteration in the hemoglobin molecule is the possible introduction of genetic material into the cytoplasm of the erythrocytes. Since erythrocytes have neither nuclei nor ribosomes there is no mechanism for the erythrocytes to translate the genetic code into spike proteins. Genetic material including RNA and DNA found outside cells capable of transcribing or translating genetic material has previously been shown to result in the prion type alteration of other proteins [6]. It has also been shown that lipid nanoparticle drug vaccine biologics are distributed throughout the body [7] to varying degrees, including the blood. Entry of this genetic material can either be through the fusion of the lipid nanoparticles with the erythrocyte membrane [8, 9] or via erythrocyte binding with the adenovirus [10, 11] vector.
If such genetic material is then introduced into erythrocytes that lack the ability to translate the genetic code into spike proteins, this could explain a possible conformational change in the hemoglobin molecule resulting in a loss of retention of oxygen and subsequent desaturation with loss of red erythrocyte color. If that change is persistent it would explain the persistent loss of erythrocyte oxygen saturation.
Alteration in the hemoglobin molecule would consequently result in the inability of erythrocytes to carry oxygen to the body and the same carrier molecule (hemoglobin) would be unavailable for removal of carbon dioxide from the body.
Finally, coalescing of erythrocytes was noted in several samples along with changes in erythrocyte morphology and color. This immunologic InflammoThrombotic virally mediated response was initially described in 1994 and published in 1999 [12]. This InflammoThrombotic response was not observed when normal saline, atropine, or Domitor was added to the blood and observed for the same 3 to 5-minute period of time. The only difference between peripheral blood smears showing this InflammoThrombotic coalescence of erythrocytes and those that did not was the presence of the vaccines. This was seen with all three vaccines and was not related to the time of observation as noted by the absence of coalescence using normal saline observed for the same period of time.
Analysis of the vaccines independently showed evidence of particulate contaminants; however, there was no evidence of substantial graphene oxide. There was no evidence of bacteriologic life or nanotechnology. Given the source of the vaccine vials used in this study, the differential reporting of “bad batches” of vaccines being discussed in the lay press would appear to be more related to the tendency of clinicians in certain areas of the country to report vaccine adverse effects, while clinicians in other regions of the U.S. are less inclined to report adverse effects.
Conclusion
While there is undoubtedly a dose response effect to this desaturation of erythrocytes upon exposure to the mRNA and DNA drug vaccines biologics for SARS-CoV-2; there should be no observed prion type desaturation of erythrocytes. The clinical implications would undoubtedly be determined by the amount and duration of interaction between the vaccines and erythrocytes. The effect was seen in each participant with each of the three vaccines, including people who have and have not been previously vaccinated. The results demonstrate the need for further investigation. Also of concern are possible impurities in some of the vaccines particularly those containing lipid nanoparticles [13]. However, there is no observable graphene oxide, biologic agents, or nanotechnology in the vaccines.
Limitations
This study looked at seven people receiving the Pfizer vaccine; with six people receiving all three of the drug vaccine biologics under U.S. investigation from a total of 11 vaccine vials. This study demonstrates the need for further investigation and caution with larger numbers of individuals blood samples, as well as concern for individuals who have been vaccinated to date. At this time there is sufficient reason to pause the vaccination programs while this is further investigated.
Acknowledgment
Funding, supplies and equipment included Fleming Diagnostic Imaging and Therapeutic Management, LLC; Regen IV Wellness of Dallas, TX; and Brighteon Studios.
Conflict of interest
The authors have no conflicts of interest to report.
References
-
Stoll S (2021) How much oxygen is in the atmosphere? Have you ever wondered how much breathable air is on Earth? https://scottstoll.com/how-much-oxygen-is-in- the-atmosphere/
-
Pfizer (2020) Vaccines and Related Biological Products Advisory Committee Meeting, FDA Briefing Document, Moderna COVID-19 Vaccine.
-
Moderna (2020) Vaccines and Related Biological Products Advisory Committee Meeting. FDA Briefing Document, Moderna COVID-19 Vaccine.
-
Janssen (2021) Vaccines and Related Biological Products Advisory Committee Meeting. FDA Briefing Document, Janssen Ad26.COV2.S Vaccine for the Prevention of COVID-19.
-
How many cells are in the human Body? Fast Facts. https://www.healthline.com/health/number-of-cells- in-body
-
Mushegian, AR, Elena SF (2020) RNAs that behave like prions. mSphere 5(4): 1-11.
-
Bahl K, Senn, JJ, Yuzhakov O, Bulychev A, Brito LA, et al. (2017) Preclinical and clinical demonstration of immunogenicity by mRNA vaccines against H10N8 and H7N9 influenza viruses. Molecular Therapy 25(6): 1316-1327.
-
Xia Q, Zhang Y, Li Z, Hou X, Feng N (2019) Red blood cell membrane-camouflaged nanoparticles: a novel drug delivery system for antitumor application. Acta Pharmaceutica Sinica B 9(4): 675-689.
-
Schoenmaker L, Witzigmann D, Kulkarni JA, Verbeke R, Kerstenet G, et al. (2021) mRNA-lipid nanoparticle COVID-19 vaccines: Structure and stability. International Journal of Pharmaceutics 601: 120586.
-
Carlisle RC, Di Y, Cerny AM, Sonnen AFP, Sim RB (2009) Human erythrocytes bind and inactivate type 5 adenovirus by presenting Coxackie virus-adenovirus receptor and complement receptor 1. Blood 113(9): 1909-1918.
-
Roelvink PW, Lizonova A, Lee JGM, Bergelson JM, Finberg RW, et al. (1998) Coxsackievirus-Adenovirus Receptor Protein Can Function as a Cellular Attachment Protein for Adenovirus Serotypes from Subgroups A, C, D, E, and F. Journal of Virology 72(10): 7909-7915.
-
Fleming RM (1997) The Pathogenesis of Vascular Disease. Textbook of Angiology. In: Chang JC (Ed), Springer-Verlag New York, pp: 787-798.
-
Packer M, Gyawali D, Yerabolu R, Schariter J, White P (2021) A novel mechanisms for the loss of mRNA activity in lipid nanoparticle delivery systems. Nature Communications 12: 677.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies