The Alfresco Aqueducts- Extrahepatic Cholangiocarcinoma
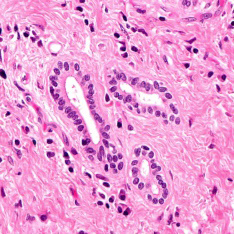
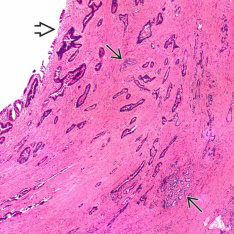
Extrahepatic cholangiocarcinoma or extrahepatic bile duct carcinoma is an exceptionally discerned, malignant neoplasm. Majorities (~95%) of neoplasms appear as adenocarcinoma and tumefaction is infrequently encountered, in contrast to adenocarcinoma gallbladder. Extrahepatic cholangiocarcinoma exhibits localized tumour extension into ampulla of Vater, colon, duodenum, gallbladder, hepatic parenchyma, omentum, pancreas or gastric region. Tumours emerging from right hepatic duct or left hepatic duct may extend proximally into hepatic parenchyma or distally into common hepatic duct. Tumours arising from cystic duct extend into gallbladder or common bile duct. Tumours engendered from distal common bile duct extend to pancreas, duodenum, colon, omentum or gastric region. Tumour metastases into regional lymph nodes or sites as hepatic parenchyma, pulmonary parenchyma or peritoneum may ensue
TNM Staging of Distal Bile Duct Cholangiocarcinoma
Primary Tumour
- TX: Primary tumour cannot be assessed.
- Tis: Carcinoma in situ.
- T1: Tumour infiltration < 5 millimetres into wall of distal bile duct.
- T2: Tumour infiltration between 5 millimetres to 12 millimetres into wall of distal bile duct.
- T3: Tumour infiltration >12 millimetres into wall of distal bile duct.
- T4: Tumour infiltration into adjacent vascular articulations as celiac axis, superior mesenteric artery or common hepatic artery.
Regional Lymph Nodes
- NX: Regional lymph nodes cannot be assessed.
- N0: Regional lymph node metastasis absent.
- N1:Tumour metastasis into one to three regional lymph nodes.
- N2: Tumour metastasis into ≥ 4 regional lymph nodes distant metastasis.
- M0: Distant metastasis absent.
- M1: Distant metastasis present into hepatic parenchyma, pulmonary parenchyma or peritoneum [4, 5].
Stages of Distal Bile Duct Cholangiocarcinoma
- Stage 0: Carcinoma in situ. Regional lymph node and distant metastasis absent (Tis, N0, M0).
- Stage I: Tumour infiltration <5 millimetres into wall of distal bile duct (T1,N0,M0)
- Stage II: is subdivided into ~Stage II A: Tumour infiltration < 5 millimetres into wall of distal bile duct with regional lymph node metastasis into one to three lymph nodes; OR tumour infiltration between 5 millimetres to 12 millimetres into wall of distal bile duct (T2,N0,M0 or T1,N1,M0) ~Stage II B: Tumour infiltration ≥ 12 millimetres into wall of distal bile duct OR tumour infiltration ≥5 millimetres into wall of distal bile duct with regional lymph node metastasis into one to three lymph nodes (T3,N0,M0 or T2 or T3,N1,M0)
- Stage III: is subdivided into ~Stage IIIA: Tumour infiltration into wall of distal bile duct with regional lymph node metastasis into ≥4 lymph nodes(T1,T2 or T3,N2,M0) ~stage IIIB: Tumour infiltration into large blood vessels supplying abdominal viscera as celiac axis, superior mesenteric artery or common hepatic artery with regional lymph node metastasis absent or into ≥one lymph nodes(T4, any N, M0)
• Stage IV: Tumour metastasis into distant organs as hepatic or pulmonary parenchyma, peritoneum or diverse abdominal viscera. Tumour infiltration into wall of distal bile duct is variable and invasion into vascular articulations or regional lymph nodes may or may not occur (any T, any N, M1).
Resectable or localized carcinoma of distal bile duct is denominated by a tumour confined to accessible areas as inferior segment of common bile duct or perihilar area and can be comprehensively eradicated by surgical resection. Unresectable, metastatic or recurrent carcinoma of distal bile duct is unamenable to complete eradication with surgical resection and is preponderantly encountered within a majority of subjects. Recurrent carcinoma of distal bile duct reappears following treatment and is discernible within bile ducts, gallbladder or hepatic parenchyma [4, 5].
Extrahepatic cholangiocarcinoma is immune reactive to mucin, carcinoembryonic antigen (CEA), CK7, p-cadherin, CD24 and epidermal growth factor receptor (EGFR). Extrahepatic cholangiocarcinoma is immune non-reactive to CK20 or CD10 [5, 6]. Extrahepatic cholangiocarcinoma requires segregation from neoplasms such as intra-ductal dissemination of hepatocellular carcinoma, cholangiocarcinoma or metastatic carcinoma, tumour metastasis from carcinoma breast, colon, ovary or renal parenchyma, tumour dissemination from adjacent carcinomas arising from ampulla of Vater, colon, duodenum, gallbladder, pancreatic carcinoma or gastric carcinoma, sclerosing cholangitis, carcinomas metastasizing into hepatic parenchyma, gallbladder adenoma, polyp of gall bladder, IgG4 related sclerosing cholangitis or adenomyomatosis of gall bladder [5, 6]. Surgical tissue sampling is optimal for appropriate tumour discernment as cogent clinical diagnosis may be challenging or erroneous. Cytological brushings of biliary tract or cytological examination of bile drainage fluid may be adopted for tumour detection. Extrahepatic cholangiocarcinoma exhibits elevated alkaline phosphatase. Serum bilirubin may be normal, thereby indicating tumour localization superior to bifurcation of hepatic duct or an incomplete obstruction of common bile duct. Tumours arising from distal bile duct may mandate surgical intervention with adoption of Whipple’s procedure. Klatskin tumour or hilar tumour necessitates surgical resection of bifurcation of hepatic duct. Intraepithelial tumour dissemination appears non indicative of inferior prognostic outcomes. However, carcinoma in situ arising within stump of bile duct may reoccur [5, 6].
Factors Contributing to Superior Prognostic Outcomes are Designated as
~Decimated tumour stage. ~Papillary projections upon histological examination. ~Absent metallothionein expression. ~Distally located neoplasms. ~Immune reactive CDX2 and MUC2.
Factors Contributing to Adverse Prognostic Outcomes Appear as
~Enhanced grade or stage of tumour. ~Tumour discernment upon surgical margins. ~Tumour confined to hilar region. ~Occurrence of tumour necrosis within nodal tumours. ~Severe nuclear atypia within tumour cells confined to lymphatic vessels ~Decimated expression of focal adhesion kinase. ~Expression of IMP [3]. ~Expression of nuclear KIT [5, 6].
References
-
Lotfollahzadeh S, Hoilat GJ, Smith M, Recio Boiles A, Babiker HM (2022) Hepatobiliary Tract Cancer. Stat Pearls International, Treasure Island, Florida.
-
O Hagan K (2022) Updates in Cholangiocarcinoma. J Adv Pract Oncol 13(3): 320-323.
-
Zhang X, Cai Y, Xiong X, Liu A, Zhou R, et al. (2022) Comparison of current guidelines and consensus on the management of patients with cholangiocarcinoma: 2022 update. Intractable Rare Dis Res 11(4): 161-172.
-
Javle M, Lee S, Azad NS, Borad MJ, Kelley RK, et al. (2022) Temporal Changes in Cholangiocarcinoma Incidence and Mortality in the United States from 2001 to 2017. Oncologist 27(10): 874-883.
-
Proskuriakova E, Khedr A (2022) Current Targeted Therapy Options in the Treatment of Cholangiocarcinoma: A Literature Review. Cureus 14(6): e26233.
-
Zhao F, Yang D, He J Ju X, Ding Y, et al. (2022) Establishment and validation of a prognostic nomogram for extrahepatic cholangiocarcinoma. Front Oncol 12: 1007538.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies