Clinicopathological Spectrum of Multiple Myeloma: Experience of an Institute in Eastern India
Introduction: Primary polycythemia belongs to the group of myeloproliferatifs disorders whose natural course is marked by thrombohemorrhagic events in the short term and transformation into acute leukemia in the long term. Primary polycythemia is rarely seen in our department. It usually precedes a myelodysplastic phase. Arterial thrombosis as a revealing mode is exceptional. Case report: We report the case of a 78-year-old woman diagnosed with polycythemia vera in 2018, with signs of hyperviscosity in the setting of arterial hypertension treated with hydryuree. The appearance of unexplained dyspnea in 2023 led to the diagnosis of pulmonary embolism. The follow-up blood count unexpectedly revealed a bicytopenia consisting of severe anemia at 5g/dl and thrombocytopenia at 88,000/mm3. The myelogram was consistent with AML. The evolution was rapidly fatal in our context. The interest of this work lies in the rarity of this AML secondary to polycythemia vera, but also in its exceptional mode of manifestation, making management ambiguous due to treatment of a pulmonary embolism in a context of thrombocytopenia. Conclusion: This is the first case of its kind to be described in our department.
Introduction
Plasma cell neoplasms (PCN) encompass a group of disorders characterized by clonal proliferation of plasma cells in the bone marrow [1]. The spectrum of PCN encompasses a continuum of disease states, each exhibiting distinct clinical, pathological and molecular features. At one end of the spectrum is asymptomatic precursor condition monoclonal gammopathy of undetermined significance (MGUS) and other end is multiple myeloma (MM) with features of end organ damage. Smouldering multiple myeloma (SMM) represents an intermediate stage between MGUS and symptomatic MM. Other entities in this spectrum include plasmacytoma, plasma cell leukemia and monoclonal immune deposition diseases [2]. Diagnosis of multiple myeloma requires more than 10% of clonal bone marrow plasma cells or biopsy proven plasmacytoma and ≥1 of the following myeloma defining events. 1) End organ damage (CRAB- hypercalcemia, renal failure, anemia and lytic bone lesions) attributable to plasma cell disorder. 2) Clonal bone marrow plasma cell percentage ≥60% 3) an involved-to-involved serum free light chain (SFLC) ratio ≥100. 4) >1 focal lesion on magnetic resonance imaging (MRI) [3]. The International staging system (ISS) of multiple myeloma provides strong survival estimate, which is based on pretreatment levels of serum β2microglobulin and serum albumin [4].
In year 2020, MM was the third most common hematological malignancy worldwide after Non-Hodgkin lymphoma and leukemia and contributed about 14% of all cases [5]. In 2020, the age standardized incidence of multiple myeloma was 1.78 (95% UI 1•69–1•87) per 100 000 people globally and mortality was 1•14 (95% UI 1•07–1•21) per 100 000 people globally [6]. In India, Age standardised rates (ASRs) of multiple myeloma was 0.7/100 000. According to National Cancer Registry Programme (NCRP) 2020, heterogeneity in Age standardised rates (ASRs) of multiple myeloma was observed between urban and rural areas of India. ASR of multiple myeloma in rural areas was 0.2 per 100 000 people, while in large cities it was 1.8 per 100 000 people [7].
Treatment strategies for multiple myeloma have evolved significantly in recent years. Induction chemotherapy consists of bortezomib, lenalidomide, dexamethasone (VRd) followed by autologous stem cell transplantation (ASCT) which remains a standard treatment option for eligible patients [8]. There are very few studies related to multiple myeloma from eastern India. This study thus aims to evaluate the clinico-pathological spectrum of multiple myeloma in an institute in eastern India.
Material and Methods
This was a cross sectional hospital based retrospective study after obtaining approval from the Institutional Research Committee. During 4-year period of study from June 2018- June 2022, we identified 74 cases of multiple myeloma. The diagnosis of MM was based on the International Myeloma Working Group criteria for the classification of monoclonal gammopathies, multiple myeloma, and related disorders [3].
Medical record of all the patients who were diagnosed as MM was reviewed. Patient characteristics and clinical history including age, sex, presenting symptoms, skeletal survey were recorded. Laboratory parameters including complete blood cell count, serum calcium, serum creatinine, serum protein electrophoresis, immunofixation assay, serum albumin, serum β2 microglobulin, bone marrow study results were obtained.
Data Analysis
For the statistical analysis, the statistical software SPSS version 22.0 for Windows (SPSS Inc., Chicago, IL, USA) was used.
Results
Out of 74 patients, 51 (69%) were men and 23 (31%) were women. The man to female ratio was 2.2:1. The age of the patient ranged from 32 to 81 years with a median age of 55 years. Sixth decade was the most common age group in our study and only 7 (9.4%) patients were younger than 40 years (Table 1).
| Age | Men | Women | |
|---|---|---|---|
| <40 | 6 | 1 | 6:01 |
| 41-50 | 13 | 4 | 13:04 |
| 51-60 | 17 | 7 | 17:08 |
| 61-70 | 12 | 8 | 3:02 |
| 71-80 | 3 | 2 | 3:02 |
| 81-90 | 0 | 1 | 0:01 |
| 51 | 23 | 2.2:1 | |
| Median Age: 55 years | |||
| Range: 32-81 years |
Table 1: Demographic data of patients with Multiple myeloma (n=74).
Clinical Features
The most common clinical presentations were fatigue 60 (81%) and bone pain 48 (65%).
Laboratory Parameters
| Results | ||||||
|---|---|---|---|---|---|---|
| No. of Patient | Median | Range | Distribution | No. | Percentage | |
| Hemoglobin (Gm/Dl) | 74 | 7.9 | 3.4-14.1 | ≤8 | 39 | 52.7 |
| 8.1-10.0 | 21 | 28.3 | ||||
| 10.1-12 | 9 | 12.1 | ||||
| >12 | 5 | 6.7 | ||||
| Creatinine (Mg/Dl) | 61 | 1.2 | 0.43-10.05 | <1.3 | 33 | 54.1 |
| 1.3-1.9 | 13 | 21.3 | ||||
| ≥2 | 15 | 24.6 | ||||
| Calcium (Mg/Dl) | 54 | 9.83 | 6.9-17.4 | <8.5 | 8 | 14.8 |
| 8.5-10.9 | 29 | 53.8 | ||||
| ≥11 | 17 | 31.4 | ||||
| ß2 Microglobulin(MG/L) | 18 | 3344 | 2.48- 14400 | <3.5 | 2 | |
| 3.5-5.5 | 2 | |||||
| >5.5 | 14 |
Table 2: Laboratory test results in patients with Multiple myeloma.
Hematological Factors
Hematological factors- At presentation anemia (hemoglobin levels <10 gm/dl) was present in 60 (81%) patients. Severe anemia (hemoglobin < 8 gm/dl) was present in 39 (52.7%) patients and only 5 (6.7%) patients had hemoglobin >12 gm/dl. The anemia was predominately normocytic normochromic. Microcytic hypochromic anemia was observed in 17 (23%) patients and macrocytic anemia in 5 (6.7%) patients. Rouleaux formation Figure 2A on peripheral blood smear was observed in 35 (47.3%) patients. The total leukocyte counts less than 4 x 109/L was observed in 11 (14.8%) patients and leucocytosis was noted in 13 (17.5%) patients. Thromobocytopenia (platelet counts less than 100 x 109/L) was present in 7 (9.4%) patients. Circulating plasma cells were observed in 6 (8%) patients and 2 patients were diagnosed as Plasma cell leukemia (plasma cells>20% of total leukocyte count). Erythrocyte sedimentation rate (ESR) were available in 37 cases, out of which 35 patients had ESR more than 20mm/hr and more than 100mm/hr in 9 patients. Serum creatinine more than 2 mg/dl was present in 15 (24.6%) patients and hypercalcemia was observed in 17 (31.4%) of patients. Serum lactate dehydrogenase level was performed in 27 patients, 22 (81.4%) of which showed levels more than 260 U/L
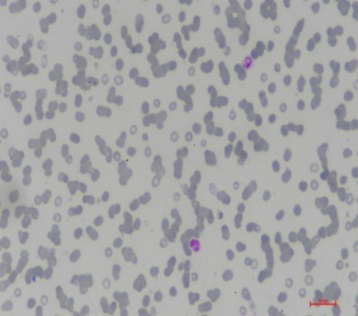
Figure 2A: Peripheral Blood Film Smear Showing Rouleaux Formation (Leishman Stain, 400x).
Serum Protein Electrophoresis
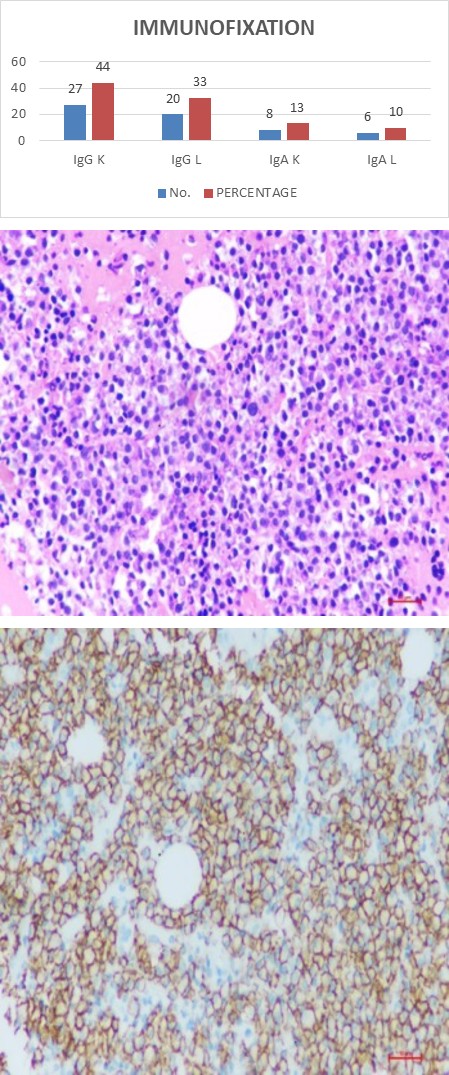
Serum protein electrophoresis showed an M-protein in all the 74 patients. Serum Immunofixation was performed in 61 patients. The most common monoclonal gammopathy was IgG kappa in 27 (44%) patients followed by IgG lambda in 20 (33%) patients. IgA kappa was noted in 8 (13%) and IgA lambda in 6 (10%) patients (Figure 1).
Bone Marrow Examination
The bone marrow plasma cell count was estimated on aspiration smears by differential count of 1000 nucleated cells. All the patients had more than 10% of plasma cells and median value of plasma cells was 52%. More than 60% plasma cells were observed in 31 (42%) patients. Bone marrow biopsy was adequate for evaluation in 59 patients. Most common pattern was diffuse infiltration, observed in 35 (59%) patients followed by interstitial pattern in 16 (27%) patients and nodular pattern in 8 (14%) patients (Table 3), (Figures 2B-D).
| Plasma Cells | No. of Patients | Percentage |
|---|---|---|
| <10 | 0 | 0 |
| 20-Oct | 10 | 13.5 |
| 21-30 | 11 | 14.8 |
| 31-40 | 9 | 12.1 |
| 41-50 | 6 | 8.1 |
| 51-60 | 7 | 9.4 |
| 61-70 | 13 | 28.9 |
| 71-80 | 4 | 5.4 |
| >80 | 14 | 18.9 |
Table 3: Bone Marrow Plasma Cells in Patients with Multiple myeloma (n=74).
Figure 2B: Bone marrow aspirate, smear showing many plasma cells (MGG stain, 400x).
Figure 2C: Bone marrow trephine biopsy section, showing diffuse infiltration by plasma cells (H&E, 400x).
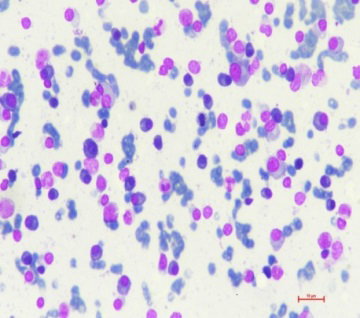
Figure 2D: Bone marrow trephine biopsy section, CD138 immunohistochemistry highlighting plasma cells (400x).
Bony Lesions
Different modalities including conventional X-ray radiography, low dose computed tomography (CT) and magnetic resonance imaging (MRI) are available for detecting osseous lesions in MM. Imaging findings were available in 62 out of 74 patients. Lytic lesions were found in 39 (63%) patients and 13 (21%) patients showed punched out lesions. Compression fracture of spine was observed in 3 patients. No radiographic abnormalities were observed in 7 (11%) patients at the time of diagnosis (Table 4).
Prognosis and Predictive Factors
| Findings | Number | Percentage |
|---|---|---|
| Lytic Lesions | 39 | 63 |
| Punch Out Lesions | 13 | 21 |
| Compression | 3 | 5 |
| Negative | 7 | 11 |
| Total | 62 |
Table 5: Radiographic findings in patients with Multiple myeloma (n=62).
International staging system (ISS) that predicts the patient survival includes combination of serum albumin and β2 microglobulin [4]. Serum albumin was less than 3.5 gm/ dl in 42 (56.7%) patients. Values of β2 microglobulin were available in 18 patients only, out of which 14 had value more than 5.5 mg/L. These 14 patients were classified under stage III of ISS. Value of β2 microglobulin was <3.5 mg/L in 2 patients and were classified in stage I and between 3.5 mg/L to 5.5 mg/L in 2 patients and were classified under stage II of ISS. Table 5 ISS staging of 56 patients were not feasible due to unavailability of β2 microglobulin levels.
| Stage I | Stage II | Stage III |
|---|---|---|
| 2 | 2 | 14 |
Table 4: International Staging System (N=18).
Discussion
MM is considered as a disease of the old with median age of 60-70 years in western countries [9]. The median age of patients in our study was 55 years which was lower compared to western countries. Sixth decade was the most common age group at presentation in other Indian studies by Jacob et al and Kaur, et al. [10, 11] Our study showed higher percentage of patients (9.4%) with age less than 40 years compared to 2% and 2.2% in study by Kyle, et al. [9] and Blade, et al. [12] Indian study by Yanamandra, et al. [13] reported higher incidence (9.6%) of MM in the patients less than 40 years of age similar to our result. A high male: female ratio observed in our study was similar to the study by Asian myeloma network and other India studies [10, 11, 12, 13, 14]. Fatigue and bone pain was the most common clinical presentation similar to other study [9].
In our study anemia (Hemoglobin levels <10 gm/dl) and severe anemia (Hemoglobin < 8 gm/dl) at presentation was observed in 81% and 52.7% of the patients respectively. Although in majority of the patients, anemia was normocytic normochromic, 23% patients had microcytic anemia. Compared to study by Kyle, et al. [9] incidence of severe anemia and microcytic anemia is higher in our studies. In a developing country like ours, anemia could be multifactorial in origin. Other etiologies including iron deficiency needs to be evaluated at presentation before attributing it solely to MM. Thrombocytopenia was present in 9.4% of the patients, which was similar to Kyle, et al. [9].
In patients with MM, circulating plasma cells of >5% is associated with poor prognosis [15]. In our study only 6(8%) patients had circulating plasma cells, out of which 5 had >5% circulating plasma cells. Two patients had more than 20% plasma cells and these cases were labelled as plasma cell leukemia. Patient having >5% circulating plasma cells had higher proportion of bone marrow plasma cells (median 86% vs. 52%) and this correlation was statistically significant (p value <0.05) and these findings were similar to study by Granell, et al. [15].
Hypercalcemia and renal dysfunction are two important diagnostic criteria of MM. The primary cause of hypercalcemia in MM is tumor induced increased osteoclastic bone resorption [16]. In our study, hypercalcemia was observed in 31.4% of the patients, 53.8% of the patients diagnosed as MM had normal calcium levels. All the patients with hypercalcemia had anemia and 8 (47%) of them had severe anemia. Six out of 17 (35%) patients with hypercalcemia had renal dysfunction. Study by Bao, et al. [17] showed that in a newly diagnosed case of MM, hypercalcemia was associated with high levels of serum creatinine, low hemoglobin level and poor outcome.
Toxic effect of monoclonal light chain is the major reason of development of renal dysfunction in MM [18]. Incidence of renal dysfunction is reported in 15% to 40% of the patients with MM and up to 10% of them require dialysis [19]. In our study, renal dysfunction was reported in 15% of the patients.
Serum immunofixation revealed IgG M protein in 77% of the patients followed by IgA in 23% and IgG kappa being the most common type. In the study by Kyle, et al. [9] IgG M protein was observed in 52% of the patients. No case of light chain myeloma was observed in our study. The median value of plasma cells in the bone marrow was 52%, which was similar to study by Kyle, et al. [9] in a newly diagnosed case of MM, more than 60% plasma cells is one of the myeloma defining lesion and associated with poor outcome. Study by Al saleh, et al. [20] showed that 39% of the patient had more than 60% plasma cells which is comparable to what we observed (42%) in our study. Our study showed diffuse pattern as the most common pattern (59%) of infiltration by plasma cells similar to Subramanian, et al. [21].
Medical imaging is crucial for the diagnosis of MM. Increased osteoclastic activity and reduced osteoblastic functions are main pathogenic mechanism of bone lesions in MM [22]. Kyle, et al. [9] reported lytic lesions in 66% patients similar to our study.
At the time of initial presentation, serum albumin and β2 microglobulin levels are two important parameters to predict the patient outcome [4]. In our study 56.7% patients had Serum albumin <3.5 gm/dl which is an indicator of poor outcome. Study by Asian myeloma network, which included 3405 patients from various Asian countries reported serum albumin <3.5 gm/dl in 52% of the patients, which was quite similar to our findings [14]. Due to financial constraints of our study group, β2 microglobulin levels were available in only 18 cases and hence ISS staging was not feasible in all the cases. This is one of the important limitations of our study. Other limitations of our study are unavailability of cytogenetics, treatment and survival outcome data.
Key Message
Multiple myeloma is a disease with multi system involvement. Our study from eastern India reiterates that Indian population has onset of MM at younger age. At presentation our study group had higher proportion of anemia and advance disease.
References
-
Kyle RA, Rajkumar SV (2008) Multiple myeloma. Blood 111(6): 2962-2972.
-
Raab MS, Podar K, Breitkreutz I, Richardson PG, Anderson KC, et al. (2009) Multiple myeloma. Lond Engl 374(9686): 324-339.
-
Rajkumar SV (2016) Multiple myeloma: 2016 update on diagnosis, risk-stratification, and management. Am J Hematol 91(7): 719-734.
-
Greipp PR, San Miguel J, Durie BGM, Crowley JJ, Barlogie B, et al. (2005) International staging system for multiple myeloma. J Clin Oncol 23(15): 3412-3420.
-
https://gco.iarc.fr/today/homehttps://gco.iarc.fr/ today/data/factsheets/cancers/35-Multiple-myeloma- fact-sheet.pdf.
-
Huang J, Chan SC, Lok V, Zhang L, Lucero Prisno DE, et al. (2022) The epidemiological landscape of multiple myeloma: a global cancer registry estimate of disease burden, risk factors, and temporal trends. Lancet Haematol 9(9): e670-e677.
-
Swaminathan R, Mehra N (2022) Improving the global reporting of multiple myeloma: a focus on low-income and middle-income countries. Lancet Haematol 9(9): e631-e632.
-
Rajkumar SV (2018) Multiple myeloma: 2018 update on diagnosis, risk‐stratification, and management. Am J Hematol 93(8): 1091-1110.
-
Kyle RA, Gertz MA, Witzig TE, Lust JA, Lacy MQ, et al. (2003) Review of 1027 Patients With Newly Diagnosed Multiple Myeloma. Mayo Clin Proc 78(1): 21-33.
-
Jacob LA, Suresh Babu MC, Lakshmaiah KC, Babu KG, Lokanatha D, et al. (2007) Multiple myeloma: Experience of an institute in limited resource setting. Indian J Cancer 54(1): 340-342.
-
Kaur P, Shah BS, Baja P (2014) Multiple myeloma: a clinical and pathological profile. Gulf J Oncolog 1(16):14- 20.
-
Blade J, Kyle RA, Greipp PR (1996) Presenting features and prognosis in 72 patients with multiple myeloma who were younger than 40 years. Br J Haematol 93(2): 345-351.
-
Yanamandra U, Saini N, Chauhan P, Sharma T, Khadwal A, et al. (2018) AYA-Myeloma: Real-World, Single-Center Experience Over Last 5 Years. J Adolesc Young Adult Oncol 7(1): 120-124.
-
Kim K, Lee JH, Kim JS, Min CK, Yoon SS, et al. (2014) Clinical profiles of multiple myeloma in Asia-An Asian Myeloma Network study. Am J Hematol 89(7): 751-756.
-
Granell M, Calvo X, Garcia-Guiñón A, Escoda L, Abella E, et al. (2017) Prognostic impact of circulating plasma cells in patients with multiple myeloma: implications for plasma cell leukemia definition. Haematologica 102(6): 1099-1104.
-
Oyajobi BO (2007) Multiple myeloma/hypercalcemia Arthritis. Res Ther (Suppl 1): S4.
-
Bao L, Wang Y, Lu M, Chu B, Shi L, et al. (2020) Hypercalcemia caused by humoral effects and bone damage indicate poor outcomes in newly diagnosed multiple myeloma patients. Cancer Med 9(23): 8962- 8969.
-
Kundu S, Jha SB, Rivera AP, Flores Monar GV, Islam H, et al. (2022) Multiple Myeloma and Renal Failure: Mechanisms, Diagnosis, and Management. Cureus 14(2): e22585.
-
Dimopoulos MA, Terpos E, Chanan Khan A, Leung N, Ludwig H, et al. (2010) Renal impairment in patients with multiple myeloma: a consensus statement on behalf of the International Myeloma Working Group. J Clin Oncol 28(33): 4976-4984.
-
Al Saleh AS, Parmar HV, Visram A, Muchtar E, Buadi FK, et al. (2020) Increased Bone Marrow Plasma-Cell Percentage Predicts Outcomes in Newly Diagnosed Multiple Myeloma Patients. Clin Lymphom Myeloma Leuk 20(9): 596-601.
-
Subramanian R, Basu D, Dutta TK (2009) Prognostic significance of bone marrow histology in multiple myeloma. Indian J Cancer 46(1): 40-45.
-
Hameed A, Brady JJ, Dowling P, Clynes M, O Gorman P, et al. (2014) Bone disease in multiple myeloma: pathophysiology and management. Cancer Growth Metastasis 7: 33-42.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies