The Exiguous Imetus-Fumarate Hydratase Deficient Renal Cell Carcinoma
Fumarate hydratase deficient renal cell carcinoma is an exceptionally discerned neoplasm which arises on account of germline mutations within fumarate hydratase (FH) gene. Commonly, clinical manifestations as non-renal leiomyomatosis may concur. Neoplasm is associated with autosomal dominant mode of disease transmission. Neoplasm may configure as a high grade, infiltrative lesion comprised of papillary articulations or solid sheets of neoplastic cells. Characteristically, tumour cells nuclei are pervaded with inclusion like nucleoli and demonstrate peri-nucleolar clearing. Neoplasm arises on account of oncogenesis triggered due to metabolic inconsistencies emerging as a consequence of defective fumarate hydratase enzyme. The high grade, infiltrative neoplasm articulating papillary structures or solid sheets is comprised of tumour cells incorporated with prominent cytomegalovirus (CMV) like nucleolar inclusions and foci of peri-nucleolar clearing. Neoplastic cells manifest overexpression and immunoreactivity to modified cysteine (2SC) along with decimation of fumarate hydratase enzyme.
Introduction
Confirmatory analysis may be obtained by ascertaining germline mutations within fumarate hydratase gene. Fumarate hydratase (FH) gene is situated upon chromosome 1q42-43 and is comprised of 10 exons. Tumor cells depict impaired oxidative phosphorylation wherein constituent cells demonstrate a metabolic transition into aerobic glycolysis. In the absence of fumarate hydratase activity, levels of fumarate appear elevated wherein the enzyme functions as an onco- metabolite. Fumarate impairs function of hypoxia inducible factor prolyl hydroxylase with consequently increased levels of hypoxia inducible factor 1 alpha -HIF1a [1, 2]. Germline mutations within fumarate hydratase gene are associated with enhanced possible emergence of uterine leiomyomas, cutaneous leiomyomas and renal cell carcinoma. Concordant renal carcinoma is additionally designated as hereditary leiomyomatosis and renal cell carcinoma syndrome associated renal carcinoma or fumarate hydratase deficient renal cell carcinoma [1, 2]. Fumarate hydratase deficient renal cell carcinoma is commonly confined to renal parenchyma. In addition, hereditary leiomyomatosis and renal cell carcinoma syndrome associated renal carcinoma demonstrates leiomyomas confined to uterus and diverse cutaneous surfaces.
Genetic mutations occurring within fumarate hydratase (FH) gene induces defective fumarate hydratase enzyme within the citric acid cycle with consequent metabolic derangement, ‘pseudo-hypoxic’ upregulation of hypoxia inducible factor 1 alpha -HIF1a and non-enzymatic modification of cysteine residues within multiple proteins, designated as ‘succination’. Subsequently, enzymatic function is altered with consequent initiation of oncogenesis [1, 2]. Hereditary leiomyomatosis and renal cell carcinoma syndrome associated renal carcinoma is encountered within one third (~33%) subjects delineating HLRCC germline mutation. Mean age of representation of renal cell carcinoma is 36 years.
In contrast, the predominant cutaneous leiomyomas and uterine leiomyomas are encountered within ~85% of incriminated individuals and are commonly exemplified within the third decade. Uterine leiomyomata are innumerable and enlarged. An estimated 50% of incriminated female subjects necessitate a hysterectomy below< 30 years although surgical therapeutic intervention is necessitated within 18 years to 52 years. Grossly, a solitary, unilateral, solid or cystic neoplasm is enunciated. Tumour magnitude varies from 2.5 centimeters to 12.0 centimeters [3, 4].
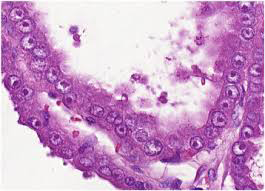
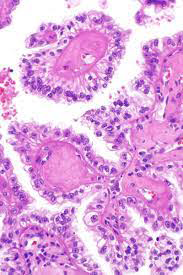
Upon microscopy, the high grade tumefaction exemplifies distinct configurations as papillary, tubular, solid, cribriform, cystic, sarcomatoid or collecting duct carcinoma-like, Tumour cells are permeated with prominent eosinophilic, cytomegalovirus (CMV)-like nucleoli and a distinct peri- nucleolar halo. Nucleolar alterations may be focal. Papillary articulations may delineate hyalinised and oedematous fibro-vascular cores with micro-papillary fronds. Aggregates of foamy macrophages are absent in Figures 1 & 2 [3, 4].
TNM staging of renal cell carcinoma as per American Joint Committee on Cancer
Primary tumour
TX: Primary tumour cannot be assessed T0: No evidence of primary tumour T1: is subdivided into
- T1a: tumour confined to renal parenchyma<4 centimeter diameter
- T1b: tumour confined to renal parenchyma >4 centimeter and <7 centimeter diameter T2: Tumour confined to renal parenchyma ≥ 7 centimeter diameter
- T2a: tumour confined to renal parenchyma >7 centimeter and up to 10 centimeter diameter
- T2b: tumour confined to renal parenchyma >10 centimeter diameter T3: Tumour of variable magnitude with extension into major veins as renal vein or inferior vena cava or perinephric tissues although ipsilateral adrenal gland is spared. Tumour extension beyond Gerota’s fascia is absent.
- T3a: tumour demonstrates macroscopic extension into renal vein or muscular, segmental branches with tunica media or tumour invades peri-renal tissue or adipose tissue of renal sinus. Tumour extension beyond Gerota’s fascia is absent.
- T3b: tumour dissemination into infra diaphragmatic inferior vena cava
- T3c tumour dissemination into supra diaphragmatic inferior vena cava or invasion into wall of inferior vena cava T4: Tumour of variable magnitude incriminating ipsilateral adrenal gland or tumour extension beyond Gerota’s fascia.
Regional lymph nodes
- NX: Regional lymph nodes cannot be assessed
- N0: Regional lymph node metastasis absent
- N1: Regional lymph node metastasis present
Distant metastasis
- M0: Distant metastases absent
- M1:Distant metastases present
Staging of renal cell carcinoma
- Stage I: T1, N0, M0
- Stage II: T2, N0, M0
- Stage III: T3, N0, M0 OR T1, T2, or T3, N1, M0
- Stage IV: T4, any N, M0 OR any T, any N, M1. Contiguous incrimination of ipsilateral adrenal gland is contemplated as stage T4 whereas noncontiguous involvement is designated as M1. Commonly discerned sites of distant metastasis emerge as pulmonary parenchyma, bone, lymph node, hepatic parenchyma, adrenal gland and brain, in decreasing order of frequency.
Discussion
Neoplastic cells appear immune reactive to PAX8, vimentin, GLUT1, p53, S100A1 protein, succinate dehydrogenase subunit B(SDHB) or integrase interactor 1(INI1). Besides, nuclear and cytoplasmic overexpression of 2-succino-cysteine (2SC) emerges as a sensitive and specific technique for neoplastic discernment, in contrast to genomic mutation within fumarate hydratase gene as detected with cogent immunohistochemistry. Tumour cells appear immune non-reactive to fumarate hydratase, carbonic anhydrase IX(CAIX), alpha methyacyl CoA racemase (AMACR), CK7, CK20, CD117,RCC, TFE3 and high molecular weight cytokeratin (HMWCK) [5, 6].
Fumarate hydratase deficient renal cell carcinoma requires segregation from neoplasms such as papillary type II renal cell carcinoma, clear cell renal cell carcinoma, hereditary leiomyomatosis and renal cell carcinoma syndrome associated renal carcinoma, collecting duct carcinoma, micropthalmia transcription factor (MiT) family translocation associated renal cell carcinoma or unclassified renal cell carcinoma [5, 6].
Clinical and genetic assessment of hereditary leiomyomatosis and renal cell carcinoma syndrome associated renal carcinoma is subject to cogent description of diagnostic criterion. Microscopic examination with discernible characteristic nucleolar features in concurrence with cytoplasmic and nuclear immune reactivity to 2 succino- cysteine (2SC) and loss of expression of fumarate hydratase appears pathognomonic [5, 6].
Fumarate hydratase deficient renal cell carcinoma is associated with inferior prognostic outcomes and preliminary, widespread distant metastases which may be especially envisaged within miniature neoplasms [5, 6].
Conclusion
Fumarate hydratase deficient renal cell carcinoma is an exceptionally discerned neoplasm which arises on account of germline mutations within fumarate hydratase (FH) gene. Genetic mutations occurring within fumarate hydratase (FH) gene induces defective fumarate hydratase enzyme within the citric acid cycle with consequent metabolic derangement, ‘pseudo-hypoxic’ upregulation of hypoxia inducible factor 1 alpha (HIF1a) and non-enzymatic modification of cysteine residues within multiple proteins, designated as ‘succination’. The high grade, infiltrative neoplasm exemplifies distinct configurations as papillary, tubular, solid, cribriform, cystic, sarcomatoid or collecting duct carcinoma-like and is comprised of tumour cells incorporated with prominent cytomegalovirus (CMV)-like nucleolar inclusions and foci of peri-nucleolar clearing. Neoplastic cells appear immune reactive to PAX8, vimentin, GLUT1, p53, S100A1 protein, succinate dehydrogenase subunit B(SDHB) or integrase interactor 1(INI1). Tumour cells appear immune non-reactive to fumarate hydratase, carbonic anhydrase IX(CAIX), alpha methyacyl CoA racemase (AMACR), CK7, CK20, CD117,RCC, TFE3 and high molecular weight cytokeratin (HMWCK). Fumarate hydratase deficient renal cell carcinoma requires segregation from neoplasms such as papillary type II renal cell carcinoma, clear cell renal cell carcinoma, hereditary leiomyomatosis and renal cell carcinoma syndrome associated renal carcinoma, collecting duct carcinoma, micropthalmia transcription factor (MiT) family translocation associated renal cell carcinoma or unclassified renal cell carcinoma. Neoplasm is associated with inferior prognostic outcomes and preliminary, widespread distant metastases.
References
-
Bezwada D, Brugarolas J (2023) Reporting on FH- deficient renal cell carcinoma using circulating succinylated metabolites. J Clin Invest 133(11): e170195.
-
Zheng L, Zhang X, Pan X, Huang Z, Zhang M, et al. (2023) AKR1B10 Is a New Sensitive and Specific Marker for Fumarate Hydratase-Deficient Renal Cell Carcinoma. Mod Pathol 36(11): 100303
-
Liang J, Sun G, Pan X, Zhu S, Zhao J, et al. (2023) Genomic and transcriptomic features between primary and paired metastatic fumarate hydratase-deficient renal cell carcinoma. Genome Med 15(1): 31.
-
Howells E, Wigston L, Mackie G, Tran B, Nott L (2023) Advanced fumarate hydratase-deficient renal cell carcinoma responding to combination immune checkpoint inhibitors. Can J Urol 30(3):11558-11561.
-
Lv Y, Song L, Hu M (2023) Fumarate hydratase-deficient renal cell carcinoma: a case report and review of the literature. J Med Case Rep 17(1): 182.
-
Miura Y, Motoshima T, Anami T, Takemura K, Kinowaki K, et al. (2023) A Case Report of Aggressive Fumarate Hydrase-deficient Renal Cell Carcinoma With Loss of HLA Antigens. Cancer Diagn Progn 3(4): 522-527.
-
Image 1 Courtesy: Science direct
-
Image 2 Courtesy: Wikipedia
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies