Suspected Cefazolin Induced Autoimmune Hemolytic Anemia: An Unusual Reaction to a Common Antibiotic
Cefazolin is a first generation cephalosporin antibiotic commonly used for the treatment of various bacterial infections. It is generally well tolerated, with minimal side effects. However, hemolytic anemia is an extremely rare but potentially lifethreatening complication of cefazolin therapy. We report a case of a 83 year old male patient who developed severe hemolytic anemia during cefazolin therapy for urinary tract infection. The diagnosis was confirmed by laboratory findings and the resolution of hemolysis after discontinuation of cefazolin. The direct antiglobulin test was negative, suggesting a non immune mechanism of hemolysis. The pathophysiology of cefazolin induced hemolytic anemia is not fully understood, but it may involve hapten formation, cross reactivity with penicillins, or drug metabolites. Clinicians should be aware of this rare adverse reaction and consider it in patients who develop unexplained anemia during or after cefazolin therapy.
Introduction
Hemolytic anemia has an extensive differential diagnosis. Common causes include autoimmune, drug-induced, or infections. Signs and symptoms of hemolytic anemia can vary as they depend on the extent of the anemia, and the extent of compensation. Hemolytic anemia can be acute, chronic, or both. Patients with minimal or long-standing hemolytic anemia may be asymptomatic, and hemolysis is often found incidentally during routine laboratory testing. Patients with acute hemolysis, especially severe hemolysis, tend to have more symptoms. While hemolytic anemia can warrant an extensive work up to find the cause, careful consideration of the entire clinical picture is needed when coming to a presumptive diagnosis. There is an extensive amount of causes of hemolytic anemia and differential diagnosis must be ruled out. While some causes of hemolytic anemia are seen frequently, others are much less common [1, 2]. One such case is cefazolin induced hemolytic anemia. Cefazolin is a first-generation cephalosporin antibiotic commonly used for the treatment of various bacterial infections. It is known to be generally well-tolerated, with minimal side effects such as gastrointestinal disturbances and allergic reactions.
However, hemolytic anemia is an extremely rare side effect of cefazolin use, with only six case reports published in the literature to date [3, 4, 5, 6, 7, 8, 9, 10]. Other cephalosporins are frequent culprits of hemolytic anemia, especially cefotetan and ceftriaxone [11]. However, a review article published in 2021 identified only six cases of cefazolin induced hemolytic anemia (CIHA) [5]. Here we present a case of an 83-year- old man who developed hemolytic anemia during a hospital stay that was determined due to cefazolin exposure. With this case, we hope to highlight a rare adverse event due to cefazolin and to increase awareness. Cases of CIHA may go undiagnosed due to the fact that the hemolytic anemia can present along a range of severity from mild to severe.
Case Presentation
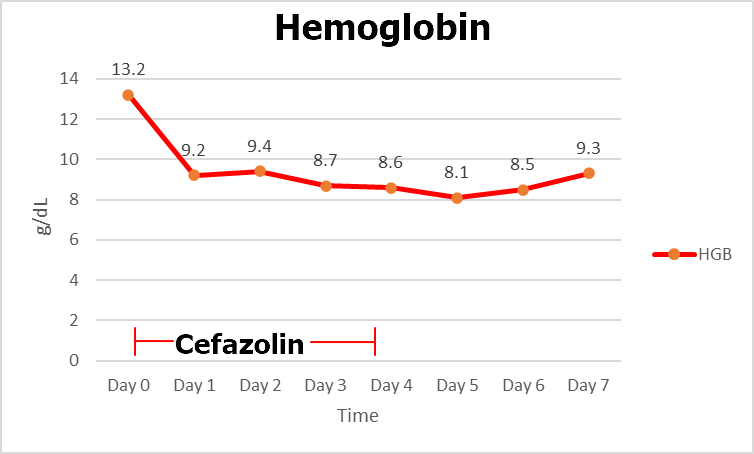
A 83-year-old male patient with a history of penicillin allergy, hypertension, dyslipidemia, gastroesophageal reflux disease, benign prostatic hyperplasia, and stroke presented to the emergency department due to a fall at home. Patient was worked up for fall; CBC, CMP, CT head, MRI head were unremarkable. However, urinalysis was positive for leukocyte esterase, and white blood cells. The patient was ultimately diagnosed with an urinary tract bacterial infection and was started on cefazolin. One day following administration of cefazolin, the patient developed anemia with a hemoglobin level of 9.2 g/dL (normal range: 13.5-17.5 g/dL) from what were normal values upon admission (13.2 g/dL). No apparent bleeding was observed and the patient had no recent surgery. Additionally, no blood was observed in either the stool or urine. Hematology was consulted on day 3 of admission due to acute anemia. Workup showed his reticulocyte count was elevated, LDH elevated, bilirubin elevated, and haptoglobin decreased. The patients’ MCV, B12, folate, iron, iron-binding- capacity, ferritin, prothrombin time, partial thromboplastin time, D-dimer, magnesium, phosphorus, and calcium were all unremarkable. A direct antiglobulin test was negative for both IgG and complement. Peripheral blood smear showed evidence of hemolysis. Bone marrow biopsy showed erythrocyte hyperplasia but no other significant findings; consistent with hemolytic anemia. Flow cytometry was unremarkable. The patient’s chart was reviewed and it was noted that he developed a mild anemia a few years prior. At this time the patient was being treated with cefazolin for methicillin-susceptible Staphylococcus aureus bacteremia. Similarly, the patient had a normal hemoglobin on admission but developed acute anemia during antibiotic treatment. The patient’s history of anemia during prior exposure to cefazolin was important for clinical decision making. A diagnosis of cefazolin induced hemolytic anemia was made, and the patient was immediately switched to an alternative antibiotic. While the anemia was not severe enough to warrant transfusion with packed red blood cells, the patient was monitored closely for any further complications. Upon discontinuation of cefazolin anemia improved. Changes in hemoglobin and hematocrit over hospital stay can be seen in Table 1 and Figure 1 respectively. The patient was counseled on his reaction to cefazolin and recommended to avoid the drug going forward.
| Day 0 | Day 1 | Day 2 | Day 3 | Day 4 | Day 5 | Day 6 | Day 7 | |
|---|---|---|---|---|---|---|---|---|
| HGB | 13.2 | 9.2 | 9.4 | 8.7 | 8.6 | 8.1 | 8.5 | 9.3 |
| HCT | 41.1 | 27.8 | 28.2 | 26.1 | 25.3 | 24.4 | 25.8 | 28.4 |
Table 1: Trended hemoglobin (HGB) and hematocrit (HCT) over patient’s hospital stay.
Discussion
Drug-induced immune hemolytic anemia (DIIHA) is a rare but potentially life-threatening complication of cefazolin therapy. The incidence of DIIHA is estimated to be less than 1 per 1,000,000 people. This is less frequent than drug-induced immune thrombocytopenia and neutropenia which is seen in up to 18 per 1,000,00 people. DIIHA is seen less compared to autoimmune hemolytic anemia (AIHA), which has been reported to occur in 1 in 80,000 people. Other cephalosporins, especially cefotetan, make up 50% of the DIIHA seen today. At one point in time the drug was even discontinued due to this reaction [11]. Cefazolin on the other hand is a much less common culprit of anemia. A review article published in 2021 identified only six cases of cefazolin induced hemolytic anemia [5, 6, 7, 8, 9, 10].
The diagnosis of cefazolin induced hemolytic anemia can be challenging, as it can present with non-specific symptoms such as fever, malaise, and anemia. Laboratory findings such as elevated reticulocyte count, elevated LDH, elevated bilirubin, decreased hemoglobin, decreased haptoglobin and evidence of hemolysis on peripheral blood smear are all findings seen in hemolytic anemia. These labs are commonly drawn in a workup of hemolytic anemia and aid in the diagnosis [11, 12, 13, 14, 15].
A direct antiglobulin test (DAT), also known as a direct coomb’s test can also be useful in the workup of a hemolytic anemia [11]. While some reports of CIHA have shown a positive DAT, others are DAT negative. Therefore, the result of the DAT test is not the most useful when diagnosing CIHA [5]. While we do not recommend omitting DAT from the workup of CIHA, DAT does not definitively rule out DIIHA. While the mechanism of CIHA is not fully understood we hypothesize that there are multiple mechanisms of action due to the varying results seen on DAT. Most often DAT tends to be positive, with IgG or complement attached to the surface of red blood cells. This is thought to be caused by the formation of antibodies against the drug or its metabolites, leading to destruction of red blood cells. Others have shown that penicillin and cephalosporin antibiotics such as cefazolin can act as a hapten causing hemolysis. It has also been hypothesized that hemolysis occurs due to a cross reactive allergy to penicillins. While more research is required to confirm these hypotheses, it is important to note that the patient we present had a documented penicillin allergy. There is no clear consensus among the other 6 case reports about the mechanism of cefazolin induced hemolytic anemia [5, 6, 7, 8, 9, 10, 11].
Autoimmune lymphoproliferative syndrome (ALPS) is a rare aetiology for immune-mediated haemolytic anaemia. ALPS is characterized by immune system dysregulation due to abnormalities in lymphocyte apoptosis (programmed cell death pathway). DAT-negative AIHA is also supportive of an ALPS diagnosis [16]. Transforming growth factor beta (TGF-β1) [17] and interleukin-10 (IL-10) are key regulators of immune homeostasis with anti-tumour effect [18]. Elevated levels of IL-10 protein in the plasma and in lymphoid tissues have been reported in ALPS patients [19]. Treatment of CIHA involves immediate discontinuation of cefazolin and initiation of alternative therapy. Supportive measures such as transfusion of packed red blood cells may be required in severe cases. We recommend trending the hemoglobin to ensure patient recovery along with markers of hemolysis. Additionally, it is recommended to avoid cefazolin for treatment of future infections including prophylaxis. Some cases of mild CIHA may recover spontaneously without any intervention other than stopping the offending agent. More severe cases may need to be treated with transfusion, however treatment should be individualized to each patient [5, 11].
Conclusion
Cefazolin induced hemolytic anemia is an extremely rare but potentially life-threatening complication of cefazolin therapy. Clinicians should be aware of this adverse reaction and consider it in patients who develop unexplained anemia during or after cefazolin therapy. A thorough history including any hemolytic anemia when exposed to cefazolin is useful when diagnosing CIHA. Previous hospital records are useful as the patient may be unaware or unable to recall details of previous medical management. While a few case reports of CIHA exist in the literature, DAT reactivity varies amongst these cases [5]. Further studies are needed to better understand the pathophysiology at the molecular level that drives the hemolysis. This may better our understanding of the condition and further our ability to identify risk factors for this rare side effect. We recommend discontinuation and avoidance of cefazolin and use of alternative antibiotics in patients with suspected CIHA.
References
-
Dhaliwal G, Cornett PA, Tierney LM (2004) Hemolytic Anemia. American Family Physician 69(11): 2599-2607.
-
Bass GF, Tuscano ET, Tuscano JM (2014) Diagnosis and Classification of Autoimmune Hemolytic Anemia. Autoimmunity Reviews 13(4-5): 560-564.
-
Quintiliani R, Nightingale CH (1978) Cefazolin. Annals of Internal Medicine 89(5 Pt 1): 650-656.
-
Beta-Lactam Antibiotics: Mechanisms of Action and Resistance and Adverse Effects (2023) UpToDate.
-
Mause E, Selim M, Velagapudi M (2021) Cefazolin- Induced Hemolytic Anemia: A Case Report and Systematic Review of Literature. European Journal of Medical Research 26(1): 133.
-
Moake JL, Butler CF, Hewell GM, Cheek J, Spruell MA (1978) Hemolysis Induced by Cefazolin and Cephalothin in a Patient with Penicillin Sensitivity. Transfusion 18(3): 369-373.
-
Imam SN, Wright K, Bhoopalam N, Choudhury A (2008) Hemolytic Anemia from Ceftriaxone in an Elderly Patient: A Case Report. Journal of the American Medical Directors Association 9(8): 610-611.
-
Cerynik DL, Lee GC, Fayssoux R, Amin NH (2007) Case Report: Cefazolin-Induced Hemolytic Anemia. Clinical Orthopaedics and Related Research 459: 260-262.
-
Macy E, Contreras R (2015) Adverse Reactions Associated with Oral and Parenteral Use of Cephalosporins: A Retrospective Population-Based Analysis. The Journal of Allergy and Clinical Immunology 135(3): 745-752.
-
Moghaddam M, Razzaghi F, Sheibani H, Pourfathollah AA (2016) A Fatal Case of Cefazolin-Induced Immune Hemolytic Anemia in Iran. Journal of Clinical & Experimental Pathology 6(5): 296.
-
Garratty G (2009) Drug-Induced Immune Hemolytic Anemia. Hematology 1: 73-79.
-
Baldwin C, Pandey J, Olarewaju O (2022) Hemolytic Anemia. Treasure Island (FL), StatPearls Publishing.
-
Doig K, Zhang B (2017) A Methodical Approach to Interpreting the Red Blood Cell Parameters of the Complete Blood Count. Clinical Laboratory Science: Journal of the American Society for Medical Technology 30(3): 173-185.
-
Siddon AJ, Tormey CA (2019) The Chemical and Laboratory Investigation of Hemolysis. Advances in Clinical Chemistry 89: 215-258.
-
Jamwal M, Sharma P, Das R (2020) Laboratory Approach to Hemolytic Anemia. Indian Journal of Pediatrics 87(1): 66-74.
-
Price S, Shaw PA, Seitz A, Joshi G, Davis J, et al. (2014) Natural History of Autoimmune Lymphoproliferative Syndrome Associated With FAS Gene Mutations. Blood 123(13): 1989-1999.
-
Hammed MRA, Ahmed YA, Adam EN, Bakry R, Elnaggar MG (2022) sVCAM-1, and TGFβ1 in Chronic Phase, Chronic Myeloid Leukemia Patients Treated with Tyrosine Kinase Inhibitors. Egypt J Immunol 29(4): 163- 173.
-
Mohammed DA, Khallaf SM, El-Naggar MGM, Abdel- Hameed MR; Bakry R (2021) Interleukin-10: A Potential Prognostic Marker in Patients with Newly Diagnosed Multiple Myeloma. Research in Oncology 17(1): 38-41.
-
Ohga S, Nomura A, Takahata Y, Ihara K, Takada H, et al. (2002) Dominant Expression of Interleukin 10 but not Interferon Γ in CD4–CD8–Αβt Cells of Autoimmune Lymphoproliferative Syndrome. British Journal of Haematology 119(2): 535-538.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies