Human Immunodeficiency Virus (HIV) Viral Load Fluctuation Mirrors the Haemoglobin Levels and Predicts the Risk of Anaemia
Background: Anaemia is a common complication of HIV infection that can have a significant impact on the health and wellbeing of affected individuals. Evaluating the relationship between haemoglobin concentration, CD4 count and viral load is therefore important in order to predict and reduce the risk of anaemia in people living with HIV. Objectives: The aim of this study was to evaluate the relationship between haemoglobin concentration, CD4 count and viral load in people living with HIV. Method: This retrospective cross-sectional study was carried out at Parirenyatwa Opportunistic Infections Clinic, Zimbabwe. The study was conducted from November 2022 to April 2023. The data collected from each patient`s data base included; demographics, haemoglobin value, CD4 count and viral load count. Data collected during this study were captured on spreadsheet using Microsoft excel and the data were analyzed using the Graph Pad prism software. Results: A total of 244 participants were enrolled into the study from the Parirenyatwa Group of Hospitals Opportunistic Infections Clinic of which 102 (41.8%) were male and 142 (58.2%) were female. Participants with high CD4 count and low viral load had a mean haemoglobin of 13.3g/dL, those with low CD4 count and high viral load count had a mean haemoglobin of 8.3g/dl, those with high CD4 count and high viral load count had a mean haemoglobin of 12.5g/dl and those with low CD4 and low viral load count had a mean haemoglobin of 10.70g/dl. Conclusion: The overall finding from this study was that haemoglobin levels of people living with HIV is greatly affected by viral load and CD4 counts and that patients’ haemoglobin levels inversely tract the HIV viral loads. Low CD4 count and/ or high viral load count is associated with anaemia in people living with HIV.
Introduction
Human Immunodeficiency virus (HIV) is a chronic infection and people living with HIV have to be followed medically, and the core treatment is the provision of antiretroviral drugs (ARVDs) which increases the quality of their lives. Without treatment, HIV can destroy the immune system and end with acquired immunodeficiency syndrome (AIDS). AIDS is the last stage of the development of HIV and has no cure. HIV can be transmitted through penetrative sexual intercourse, blood transfusion, sharing of contaminated needles, and between mother and child; during pregnancy, childbirth or during breastfeeding.
Two surrogate markers, which are HIV RNA viral load and CD4+ counts are used to monitor people living with HIV [1]. HIV is confirmed through an antigen/ antibody rapid test and/ or nucleic acid test [2]. The types of HIV infection that exist are HIV-1 and HIV- 2, although HIV-1 is the most common type in Africa and worldwide [3]. Statistics show that the prevalence of HIV among adults in 2020 was 12.9 percent, which corresponds to approximately 1.23 million adults living with HIV in Zimbabwe [4].
The most common haematological abnormality in people living with HIV is anaemia, a condition defined as a low haemoglobin concentration and has been shown to be a public health problem that affects low-, middle- and high-income countries and has significant adverse health consequences [5]. The signs and symptoms of anaemia include inexplicable exhaustion, shortness of breath, pale skin and eyes, restless legs syndrome, headaches, heart palpitations, irregular heartbeats, chest pain and coldness of the hands and feet [6].
Causes of anaemia in people living with HIV are multifactorial, and include; immune dysregulation that increases the risk of anaemia through red blood cell destruction or ineffective red blood cell production, blood loss as a result of neoplastic disease or gastrointestinal lesions accompanying opportunistic infections. Another cause of anaemia is the impaired erythropoiesis resulting from the release of inflammatory mediators and cytokines, such as; IL- 1, IL-6, IL-10, TNF, PD-1, TLR2, CD11a and sVCAM-1, which are raised in people living with HIV. There is also decreased production of and sensitivity to erythropoietin coupled with malabsorption and impaired recycling of iron [7, 8].
It is important to evaluate anaemia in people living with HIV as they are more likely to be affected by this disorder. The diagnosis of anaemia is confirmed through laboratory tests, especially full blood count (FBC). HIV viral load (the level of HIV RNA copies/mL in plasma) and CD4 count are used to monitor the severity of the immunodeficiency. The viral load reflects the level of replication of HIV in the body. Among people living with HIV, anaemia is a strong risk factor for disease progression and death. Therefore understanding the role of anaemia in HIV management is critical for the development of strategies to reduce morbidity and mortality. It is therefore necessary to evaluate anaemia in people living with HIV considering the variability of viral loads and CD4 counts with the to confirm if human immunodeficiency virus (HIV) viral load fluctuation mirrors the haemoglobin levels and predicts the risk of anaemia.
Materials and Method
Following ethical approval in 2022 by the Joint Research Ethics Committee for the University of Zimbabwe Faculty of Medicine and Health Sciences and Parirenyatwa Group of Hospitals (October 2022: JREC 347/2022), a retrospective study was carried out at Parirenyatwa Group of Hospitals Opportunistic Infections clinic from November 2022 to April 2023. Demographic and laboratory data were obtained from the patients’ database and recorded on a data sheet. The data collected from each patient`s file were; demographics, haemoglobin concentration, CD4 count and viral load count.
Study participants inclusion criteria consisted of people living with HIV who were attended to at Parirenyatwa Group of Hospitals OI Clinic and were on ARVs. Names of participants, as well as any other personal information that could be used to identify any individual were not included in this study. The information gathered for this study was kept confidential and was only accessible to the researchers. Ethical principles of research which include autonomy, non-maleficence, beneficence, justice, advocacy and confidentiality were considered and maintained throughout the study. Data collected during the study were captured by spreadsheet using Microsoft excel and presented in Table forms and Figures. Descriptive analyses, such as mean, standard deviations, median and inter-quartile ranges, were employed to summarize the raw data. The variables (CD4 count and viral load) were used to create four categories; High CD4 count and low viral load count (A), Low CD4 count and high viral load count(B), high CD4 count and high viral load count (C) and lastly low CD4 count and viral low load count (D), and their haemoglobin levels. The categorical data were analyzed using the Graph Pad prism software. One way ANOVA data comparison of the four categories and their haemoglobins was employed for data analysis.
Results
A total of 244 participants were enrolled into the study from the Parirenyatwa Group of Hospitals. The participants` mean age was 35.7 years and a standard deviation of 14.8. The study was normally distributed and the age distribution of the patients in the study showed a median age of 36 years.
Data were used to create Table 1 for participants’ demographics as well as four different categories according to the variability of the CD4 count and the viral load. The categories created are as follows:
- Category A: high CD4 count, low viral load count
- Category B: low CD4 count, high viral load count
- Category C: high CD4 count, high viral load count
- Category D: low CD4 count, low viral load count
| Variable | Frequency n (%) | |
|---|---|---|
| Gender | Male | 102 (41.8) |
| Gender | Female | 142 (58.2) |
| Age (Years) | 06-20 | 35 (14.3) |
| Age (Years) | 21-40 | 110 (45.1) |
| Age (Years) | 41-60 | 74 (30.3) |
| Age (Years) | 61-80 | 25 (9.8) |
| Mean | 35.701 | |
| Mode | 40 | |
| Median | 36 | |
| Standard deviation | 14.817 | |
| Inter quartile range | 06-70 |
Table 1: Participants` characteristics (n = 244)
The 4 categories (A-D) were used to create Table 2, illustrating the participants’ characteristics according to categories.
Table 2 showing mean, standard deviation, median and mode of the 4 categories against their number of participants (N), mean and median haemoglobin and the standard deviation of the haemoglobins.
- Category A: high CD4 count, low viral load count
- Category B: low CD4 count, high viral load count
- Category C: high CD4 count, high viral load count
- Category D: low CD4 count, low viral load count
| N | Mean | Standard Deviation | Median | Mode | |
|---|---|---|---|---|---|
| A | 117 | 13.3 | 1.326 | 13.3 | 12.7 |
| B | 65 | 8.655 | 1.713 | 8.3 | 7.4 |
| C | 34 | 11.91 | 1.079 | 12.05 | 12 |
| D | 28 | 10.2 | 1.649 | 10.7 | 11.6 |
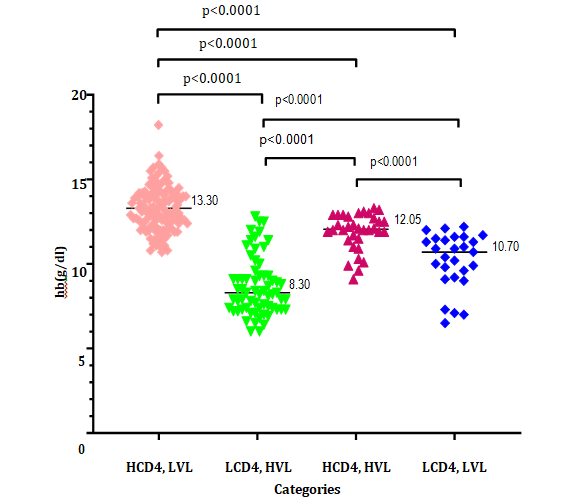
Table 2: Characteristics of participants according to categories Figure 1 is showing the 4 different categories - High CD4 count
Table 2: Characteristics of participants according to categories Figure 1 is showing the 4 different categories - High CD4 count and low viral load count, Low CD4 count and high viral load count, high CD4 count and high viral load count and lastly low CD4 count and viral low load count and their haemoglobins. The numbered line on each scatter is representing the median haemoglobin of each category. The means of the categories are then compared to another using the one- way ANOVA test. Variances are then indicated by the p values.
Discussion
HIV has overburdened health and economies of low to middle income countries. International and local initiatives are required to easy this burden through the development of algorithms that can be used in monitoring health of people living with HIV. One such initiative is to predict the risk of the development and progression of anaemia. Therefore the present study attempted to investigate the relationship between HIV viral load fluctuation and the haemoglobin levels of in people living with HIV on anti-retro-viral (ARV) treatment.
Data from the opportunistic infections clinic at Parirenyatwa group of Hospitals were used to build a simpler and cheaper algorithm to predict anaemia. There was a significant relationship between CD4 count and viral load. CD4 count and viral load are commonly used as markers to assess the immune and disease progression in people living with HIV. Haemoglobin concentration on the other hand is used to assess anaemia, which is a common complication of HIV infection [9]. When the viral load is low or going down, CD4 count will be higher or going up. When the CD4 count is low or going down, viral load will be higher or going up. The variables –(CD4 count and viral load results) were used to create four categories: High CD4 count and low viral load count (A), Low CD4 count and high viral load count (B), high CD4 count and high viral load count (C) and lastly low CD4 count and viral low load count (D) and their haemoglobins. Categories A and B are the normally encountered situations while C and D show abnormal results.
Our study revealed that females are at a greater risk of being affected by HIV than males. Females are disproportionately affected by HIV compared to males with young women most at risk. Females are at a higher risk of HIV than males due to gender inequalities, especially in low income countries. Some of the factors leading to this patten include; harmful social norms, gender-based violence leading to HIV being passed on in non-consensual sexual relationships, low or inconsistent condom use and transactional sex. Lack of access to health services or age restriction to access services and economic issues also causes females to be at a greater risk [10]. The age group of 21 to 40 years had the highest frequency of HIV infections compared to other age groups. Several factors contribute to the high HIV prevalence in this age group. These include risky sexual behaviours, lack of access to prevention and treatment services, social and cultural norms that promote early sexual debut and gender inequalities, limited knowledge about HIV prevention and transmission [11].
The category of patients with High CD4 count and low viral load had the mean haemoglobin of 13.3g/dL, which falls within normal range for both females and males. This demonstrates that there is low risk or no burden of anaemia when the CD4 count is high and the viral load count is low. The haemoglobin values in these individuals are high and normal. This phenomenon can be attributed to the body`s immune system, which will be functioning well while the HIV virus is under control. There is also perceived improved nutrition as HIV infection could impair the absorption of nutrients in the gut, leading to anaemia of nutritional deficiency [11]. Last but not least, reduced opportunistic infections help to improve haemoglobin concentrations in this category [12].
The category of participants with low CD4 count and high viral load had a mean haemoglobin concentration of 8.3g/dL, which is moderate to severe anaemia. This is because a low CD4 count and a high viral load can lead to chronic inflammation, impaired nutrient absorption and an increased risk of opportunistic infections, all of which can contribute to anaemia [9].
Participants in the category with high CD4 count and high viral load had discordance on their corresponding haemoglobin levels and had a mean haemoglobin concentration of 12.05g/dL, which is marginally low for males. Anaemia was present in some male participants in this category. It is possible for a person with HIV to have a high viral load and a high CD4 at the same time, albeit in transition. This situation is known as the discordant or non-typical immune status. This can be due to the fact that an individual’s immune system is particularly effective at controlling HIV replication even in the face of high viral loads [13]. This discordance can also be caused by less virulent HIV strains or strains that replicate more slowly than typical strains [14]. Genetic mutation is also another reason that makes people living with HIV resistant to HIV infection or slows the progression of the disease.
Participants with low CD4 count and low viral load results happen to be a rare situation and in our study had a mean haemoglobin of 10.70g/dL, which is a mild to moderate anaemia. The low viral load can occur when an individual is responding well to the ARVs. When ART is effective, it can reduce the viral load and takes long for the CD4 count to rise. However, selective IgA deficiency, certain medications, autoimmune disorders and some types of cancers could also lead to a decrease in CD4 cells [15].
Our study revealed interesting trends when the CD4 counts, viral loads and haemoglobin levels were compared as shown in Figure 1. One way ANOVA comparison of the four categories and their haemoglobins, which was done using the scatter plot to see if there was a significant difference across the 4 categories revealed statistically significant difference between all the categories when compared against each other as the p values were all less than 0.0005. This trend demonstrates that HIV viral load fluctuations inversely mirror the haemoglobin concentrations of respective participants and either result can be used to predict disease burden or risk of anaemia. This revelation can form the basis of a usable algorithm applicable in low to middle income countries.
Conclusion
The overall finding from this study was that low CD4 count and/ or high viral load is associated with anaemia in people living with HIV. Monitoring the CD4 count and viral loads when determining the risk of anaemia is then important for the identification of vulnerable individuals. These parameters can then be monitored for the prevention of anaemia. Early detection of anaemia would provide cheaper methods for prevention such as iron tablets and changing the diet. This will also help in limiting red blood cell transfusion, which is costly among the Zimbabwean population.
Recommendations
The present study showed that human immunodeficiency virus (HIV) viral load fluctuation mirrors the haemoglobin levels in people living with HIV. Based on this finding, the following recommendations can be made
- Monitoring of CD4 count and viral load regularly in order to predict the development of anaemia. People living with HIV should have their CD4 and viral load regularly monitored by a healthcare provider. This will help to identify any changes in the immune function and viral replication that could increase the risk of anaemia.
- Screening for anaemia should be done in people living with HIV particularly if they have low CD4 and high viral load. Anaemia can be treated with iron supplements or erythropoietin stimulating agents before it reaches severe cases.
- Management of co-existing conditions should be considered. People living with HIV who have low CD4, and high viral load may be at increased risk of coexisting conditions that may lead to anaemia, such as opportunistic infections and chronic kidney disease.
Funding
This research was supported by the Fogarty International Center of the National Institutes of Health under Award Number D43 TW011326. However, the content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
References
-
Thompson CG, Cohen MS, Kashuba AD (2021) Pharmalogical Approach to HIV-1. Prevention 61: 471- 490.
-
Branson BM, Owen SM, Wesolowski LG, Bennett B Werner BG, et al. (2014) Laboratory Testing for the Diagnosis of HIV infection. Centers for Disease Control and Prevention.
-
Hemelaar J, Gows E, Ghys PD (2021) Regional Distribution of HIV-1 Genetic subtypes and recombinants. Lancet HIV 8(4): e259-e268.
-
National Hiv Survey (Zimphia 2020) Results Indicate Zimbabwe is on Track to Achieve HIV Epidemic Control by 2030 (2020) U S Embassy in Zimbabwe.
-
Stevens GA, Finucane MM, Regil DLM, Paciorek CJ, Flaxman SR, et al. (2013) Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995-2011: a systematic analysis of population-representative data. Lancet Glob Health 1(1): e16-e25.
-
Moore RD, Forney D (2002) Anaemia in HIV -infected patients receiving antiretroviral therapy. J Acquir Immune Defic Syndr 29(1):54-57.
-
Kerkhoff AD, Wood R, Cobelens FG, Gupta WA, Bekker LG, et al. (2014) Resolution of anaemia in a cohort of HIV infected patients with a high prevalence and incidence of tuberculosis receiving antiretroviral therapy in South Africa. BMC Infect Dis 14: 3860.
-
Moyle G, Sawyer W, Law M, Amin J, Hill A (2004) Changes in hematologic parameters and efficacy of thymidine analogue based, highly active antiretroviral therapy: a meta-analysis of six prospective, randomized, comparative studies. Clinical Therapeutics 26(1): 92-97.
-
Sullivan PS, Hanson DL, Books JT (2006) Impact of viral load and CD4 on the incidence of anaemia in HIV-infected adults: a cohort study. J Infect Dis
-
Tomris Turmen (2003) Gender and HIV/aids. International Journal of Gynecology and Obstetrics 82(3): 411- 418.
-
Derek CM (1999) Wasting in HIV infection and AIDS. the Journal of nutrition 129(1): 238S2 -242S.
-
Palella FJ, Baker RK, Moorman AC, Chmiel JS, Wood KC, et al. (2006) Mortality in the highly active ARV therapy era: changing causes of death and disease in the HIV outpatient study. J acquir Immune Defic Syndr 43(1): 27-34.
-
Sandler NG, Wand H, Roque A, Law M, Nason MC, et al. (2011) Plasma Levels of SOLUBLE CD14 Independently Predict Mortality in HIV infection. J Infect Dis 203(6): 780-790.
-
Moir S, Chun TW, Fauci AS (2011) Pathogenic mechanisms of HIV disease. Annu Rev Pathol 6: 780-790.
-
Fauci AS, Lane HC, Redfield RR (2021) Covid-19 Navigating the Uncharted. New England Journal of Medicine 382(13): 1268-1269.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies