Bantam and Trifling-Small Cell Carcinoma Ovary
Small cell carcinoma of the ovary, hypercalcaemic subtype emerges as an infrequently discerned, malignant ovarian neoplasm with an aggressive clinical course. Tumefaction delineates inactivating chromosomal mutations of SMARCA4 gene and is commonly associated with hypercalcemia. Tumefaction appears non concordant with small cell neuroendocrine pulmonary carcinoma. Neoplasm is additionally designated as SMARCA4 deficient carcinoma of ovary or malignant rhabdoid tumors of the ovary.
Abbreviations
RTPS2: Rhabdoid Tumor Predisposition Syndrome 2; DNA: Deoxyribonucleic Acid; ATRT: Atypical Teratoid / Rhabdoid Tumor; FIGO: International Federation of Gynecology and Obstetrics; EMA: Epithelial Membrane Antigen; TTF: Thyroid Transcription Factor; CT: Computerized Tomography; MRI: Magnetic Resonance Imaging; CNS: Central Nervous System.
Editorial
Small cell carcinoma of the ovary, hypercalcaemic subtype emerges as an infrequently discerned, malignant ovarian neoplasm with an aggressive clinical course. Tumefaction delineates inactivating chromosomal mutations of SMARCA4 gene and is commonly associated with hypercalcemia. Tumefaction appears non concordant with small cell neuroendocrine pulmonary carcinoma. Neoplasm is additionally designated as SMARCA4 deficient carcinoma of ovary or malignant rhabdoid tumors of the ovary.
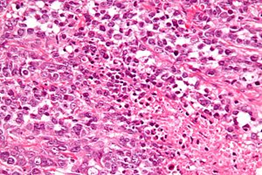
Tumor emerges as an undifferentiated small cell neoplasm composed of monomorphic, non-cohesive cells with significant mitotic activity. Morphological features as follicle- like spaces, rhabdoid morphology or large cell component may or may not be discerned. Immunohistochemistry depicts loss of nuclear SMARCA4 / BRG1 expression within > 93% neoplasms. Generally, adolescents or young, adult female subjects are implicated with median age of disease occurrence at 25 years. Tumors with germline mutations may incriminate younger subjects. Postmenopausal women are uncommonly implicated [1, 2].
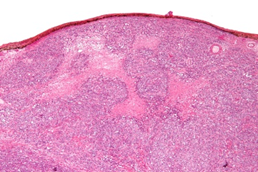
Small cell carcinoma of the ovary demonstrates inactivating germline or somatic mutations of SMARCA4 gene which is a subunit of SWI / SNF complex and is posited to trigger oncogenesis. Besides, SWI/SNF complex appears to regulate chromatin re-modeling. Neoplasm may be induced due to predisposition factors as rhabdoid tumor predisposition syndrome 2 (RTPS2) [1, 2]. Precise cellular origin of the neoplasm remains obscure and tumor is postulated to arise from epithelial, primitive germ cell, neural or mesenchymal progenitor cells. In contrast to diverse ovarian epithelial neoplasms, a definitive DNA methylation signature is encountered. Pre-eminently, tumefaction harbours inactivating somatic or germline mutations within SMARCA4 gene. Loss of expression of SMARCA2 possibly occurs due to transcriptional / posttranscriptional silencing [1, 2]. Small cell carcinoma of the ovary with hypercalcemia is genetically stable and expounds definitive DNA methylation profiles, a feature which differentiates the tumor from diverse SWI / SNF deficient carcinomas. Small cell ovarian carcinoma demonstrates an inferior clinical outcome and majority of implicated subjects represent with an advanced tumor stage. Neoplasm is associated with nonspecific clinical symptoms as pain, abdominal distention or signs of intestinal obstruction. Few subjects depict symptoms of hypercalcemia [1, 2]. Tumors with SMARCA4 germline mutation appear concurrent with rhabdoid tumor predisposition syndrome 2 (RTPS2) and demonstrates a predilection for various undifferentiated malignant tumors as atypical teratoid / rhabdoid tumor (ATRT) or extracranial malignant rhabdoid tumor [1, 2]. Grossly, neoplasm is preponderantly unilateral, solid or cystic and manifests as a lobulated mass with nodular surface. Tumor magnitude varies from 6 centimeters to 26 centimeters with mean tumor diameter of 15 centimeters. Cut surface is fleshy, tan to grey/white. Focal haemorrhage and necrosis are commonly observed. Familial neoplasms are frequently bilateral [1, 2]. Upon microscopy, tumefaction displays a diffuse pattern comprised of intensely adherent cells. Tumor cell nests or cords are occasionally observed. Follicle-like spaces are imbued with eosinophilic or basophilic secretions [3, 4]. Neoplasm is composed of miniature, spherical cells impregnated with scanty cytoplasm and miniature nucleoli. Majority of neoplasms depict a component of large cells with quantifiably variable, frequently discerned rhabdoid features [3, 4]. Neoplasm composed of an estimated > 50% of large cells is designated as small cell carcinoma of the ovary hypercalcaemic, large cell variant. Few neoplasms display an intermingling of mucinous glands. Focal myxoid stroma is common. Mitotic figures are quantifiably significant. Tumor necrosis is frequent [3, 4].
The International Federation of Gynaecology and Obstetrics (FIGO) staging system is commonly adopted for staging benign and malignant ovarian neoplasms and is denominated as • Stage I: tumor confined to the ovaries 1. ~stage Ia: tumor confined to singular ovary with intact ovarian capsule, absent tumor cells upon ovarian surface and absence of malignant cells within ascites or peritoneal washings. 2. ~stage Ib: tumor implicating dual ovaries while simulating stage Ia, intact ovarian capsule, absent tumor cells upon ovarian surface and absence of malignant cells within ascites or peritoneal washings ~stage Ic: tumor infiltrates singular or dual ovaries along with any feature designated as 3. Stage Ic1: tumor associated with surgical or intraoperative spill 4. stage Ic2: tumor capsule ruptured prior to surgical intervention or tumor dissemination upon ovarian or fallopian tube surface 5. stage Ic3: appearance of malignant cells within ascites or peritoneal washings • stage II: tumor involves singular or bilateral ovaries along with tumor extension into pelvic cavity below the pelvic brim or primary peritoneal carcinoma 1. ~stage IIa: tumor extension or implants within the uterus or fallopian tubes 2. ~stage IIb: tumor extension into various pelvic intraperitoneal tissues • ~stage III: tumor implicates singular or dual ovaries or fallopian tubes with definitive cytological or histological dissemination into the peritoneum beyond pelvis along with or devoid of tumor metastasis into retroperitoneal lymph nodes 1. ~stage IIIa: tumor dissemination into retroperitoneal lymph nodes along with or devoid of microscopic tumor metastasis beyond the pelvis categorized as 2. stage IIIa1: definitive cytological or histological assessment of tumor cells singularly confined to retroperitoneal lymph nodes 3. stage IIIa1(i): retroperitoneal lymph node with tumor metastasis ≤10 millimetre magnitude 4. stage IIIa1(ii): retroperitoneal lymph node with tumor metastasis >10 millimetre magnitude 5. stage IIIa2: discernible microscopic evidence of extra- pelvic extension superior to the pelvic brim with tumor extension into peritoneal cavity along with or absence of tumor metastasis into retroperitoneal lymph nodes 6. stage IIIb: discernible or macroscopic tumor metastasis into peritoneal cavity beyond the pelvis ≤2 centimeters in greatest dimension along with or devoid of tumor metastasis into retroperitoneal lymph nodes and tumor extension into capsule of liver and spleen 7. stage IIIc: discernible macroscopic tumor extension into extrapelvic tissue or peritoneal cavity >2 centimeters in greatest dimension along with or devoid of metastasis into retroperitoneal lymph nodes in addition to tumor extension into capsule of liver and spleen • Stage IV: tumor is associated with distant metastasis in the absence of metastases into peritoneal cavity and 1. ~stage IVa: pleural effusion with disseminated tumor cells 2. ~stage IVb: tumor associated with distant metastases ~ tumor metastasis into visceral parenchyma and metastases to extra-abdominal organs, inguinal lymph nodes and lymph nodes extending beyond abdominal cavity [3, 4].
Additionally, bilateral ovarian tumors may represent as stage I disease although are associated with distant metastases in ~30% subjects. Besides, majority of ovarian cancers represent as stage III lesions [3, 4].
Small cell carcinoma of the ovary appears immune reactive to Wilm’s tumor antigen 1(WT1), CD10, calretinin, epithelial membrane antigen (EMA), cytokeratin AE1/AE3 or p53 wild type antigen [4, 5]. Tumor cells display loss of nuclear SMARCA4 / BRG1 expression and SMARCA2 / BRM expression. Exceptionally, SMARCA4 proficient neoplasms depict loss of nuclear SMARCB1 / INI1 staining. Tumor cells appear immune non-reactive to CAM5.2, inhibin, CD99, thyroid transcription factor (TTF), OCT3/4 or FOXL2 [4, 5]. Small cell carcinoma of the ovary, hypercalcaemic subtype requires segregation from neoplasms as undifferentiated and dedifferentiated ovarian carcinomas, adult and juvenile granulosa cell tumor, small cell carcinoma, pulmonary subtype, dysgerminoma, embryonal rhabdomyosarcoma, primitive neuroectodermal tumor, malignant melanoma or malignant lymphoma [4, 5]. As established investigations for cogent neoplastic assessment remain lacking, small cell ovarian carcinoma may be subjected to abdominal ultrasonography and computerized tomography (CT). Histological evaluation remains obligatory for definitive tumor discernment. Appropriate tumor assessment, especially of germline SMARCA4 pathogenic variant lesions, necessitate clinical evaluation and precise genetics assays [4, 5]. Family members mandate surveillance. Members demonstrating germline SMARCA4 genetic mutation require clinical evaluation, ultrasonography and magnetic resonance imaging (MRI) of whole body and central nervous system (CNS) [4, 5]. Surgical procedures as bilateral salpingo- oophorectomy may be employed for decimating possible tumor occurrence. Nevertheless, advantage of preliminary tumor detection with imaging or surgical intervention remains debatable [4, 5]. Majority of implicated subjects display hypercalcemia due to parathyroid hormone related peptide secreted by tumor cells. However, symptoms of hypercalcemia are predominantly absent [4, 5]. Neoplasm may suitably be managed with surgical intervention, chemotherapy and radiation therapy. Standard therapeutic guidelines are available with International SCCOHT Consortium (ISC). Subsequent to complete response with induction chemotherapy, high dose chemotherapy with autologous stem cell rescue (HDC-aSCR) may be beneficially employed. Possible treatment modalities as epigenetic modulators, kinase inhibitors and immunotherapy may emerge as futuristic tools to treatment [4, 5]. Tumor stage is a significant prognostic parameter delineated as • ~FIGO stage I: 5 year overall survival at 55% • ~FIGO stage II: 5 year overall survival at 40% • ~FIGO stage III: 5 year overall survival at 29% • ~FIGO stage IV: 5 year overall survival at 0%. Factors contributing to superior prognostic outcomes are designated as ~Older age >40 years upon initial tumor discernment ~miniature tumors with magnitude < 10 centimeters and absence of large cell component [4, 5, 6, 7].
References
-
Blatnik A, Dragos VS, Blatnik O, Stegel V, Klancar G, et al. (2024) A Population-Based Study of Patients With Small Cell Carcinoma of the Ovary, Hypercalcemic Type, Encompassing a 30-Year Period. Arch Pathol Lab Med 148(3): 299-309.
-
Boujida I, Mahdi Y, Khmou M, Charif S, Horache K, et al. (2024) A rare case of small cell carcinoma of the ovary, hypercalcemic type. J Surg Case Rep 2024(2): rjae079.
-
Wens FSPL, Hulsker CCC, Fiocco M, Smetsers SE, Krijger RR, et al. (2023) Small Cell Carcinoma of the Ovary, Hypercalcemic Type (SCCOHT): Patient Characteristics, Treatment, and Outcome-A Systematic Review. Cancers (Basel) 15(15): 3794.
-
Pressey JG, Dandoy CE, Pater LE, Rios J, Sisson R, et al. (2020) Small cell carcinoma of the ovary hypercalcemic type (SCCOHT): Comprehensive management of a newly diagnosed young adult. Gynecol. Oncol 158: 538-546.
-
Tischkowitz M, Huang S, Banerjee S, Hague J, Huntsman DG, et al. (2020) Small-Cell Carcinoma of the Ovary, Hypercalcemic Type-Genetics, New Treatment Targets, and Current Management Guidelines. Clin. Cancer Res 26: 3908-3917.
-
Libre Pathology.
-
Wikimedia commons.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies