A Sustainable Approach to Utilizing Medical Waste in the Construction Industry: A Comprehensive Review
The sustainable use of medical waste in the construction sector has gained attention as an innovative solution to address the growing environmental concerns linked to biomedical waste disposal. Medical waste contributes significantly to pollution, and its effective management is vital to safeguarding both public health and the environment. Simultaneously, the construction industry, as one of the largest consumers of natural resources, generates considerable waste. Integrating medical waste into construction materials offers a dual benefit-minimizing the environmental footprint of the construction industry while providing an eco-friendly solution for managing medical waste. This paper provides a comprehensive review of the current research on the sustainable incorporation of medical waste into construction materials. It examines various methods of medical waste utilization, identifies the challenges and opportunities this approach presents, and explores the policy and regulatory frameworks that support sustainable medical waste management. The paper concludes by emphasizing the potential of this approach to promote a circular economy, reduce the environmental impact of waste management, and underscores the importance of further research and cross-industry collaboration between the medical and construction sectors.
Introduction
The demand for construction materials is currently at an all-time high, making it a critical component of the construction industry and a major factor influencing the overall cost of any project. As a result, achieving economic efficiency remains a priority in all engineering activities. In India, hospital waste management is a significant challenge, with healthcare facilities generating approximately 619 tons of medical waste daily. This research aims to explore the feasibility of using hospital waste as a partial replacement for cement in concrete. Successfully incorporating hospital waste into construction materials could not only reduce construction costs but also significantly mitigate environmental hazards. The Bio-medical Waste Management (BMWM) Rules, 2016, notified under the Environment (Protection) Act, 1986, recognize incineration as one of the safe methods for treating and disposing of biomedical waste generated across the country. These rules establish emission standards in Schedule II, which include limits for dioxins and furans. Additionally, the BMWM Rules stipulate that no healthcare facility shall set up an on-site treatment and disposal system if a Common Bio-medical Waste Treatment Facility (CBWTF) is available within a 75-kilometer radius. Where CBWTF services are unavailable, facilities must install the necessary biomedical waste treatment equipment, including incinerators, before commencing operations, subject to authorization from the appropriate authority, such as the State Pollution Control Board (SPCB) or Pollution Control Committee (PCC) in their respective State or Union
Territory.
Previous Work
Medical waste is an increasingly pressing issue due to the rising demand for healthcare services, which in turn leads to greater waste generation. A promising solution to this challenge lies in the sustainable use of medical waste within the construction industry. This literature review examines various studies that explore this innovative approach. Kavitha, et al. [1] conducted a study on the use of medical waste in concrete production. Their findings showed that incorporating medical waste as a partial replacement for cement reduced carbon dioxide emissions while enhancing the compressive strength of the concrete. They concluded that this method presents a viable and sustainable solution for managing medical waste. Similarly, Akhtar, et al. [2] investigated the use of medical waste in brick production. Their research demonstrated that adding medical waste to clay bricks improved compressive strength and decreased water absorption, suggesting that this method could offer a sustainable alternative for disposing of medical waste.
A review by Kumar, et al. [3] explored several sustainable approaches to using medical waste in construction materials, such as replacing conventional components like cement and aggregates. While highlighting the benefits, the authors also discussed challenges, including the need for proper segregation and handling of medical waste to ensure safety. In “Sustainable Medical Waste Management: A Review of State-of-the-Art Literature” by Yadav and Singh, published in the International Journal of Management, Technology, and Engineering, the authors provide an extensive review of sustainable medical waste management methods and their implications for the construction sector. They emphasize the importance of implementing strict safety measures and regulatory standards to protect both workers and the environment. Ong and Lee [4], in their article published in the Journal of Sustainable Development, reviewed the potential for using medical waste in construction and identified future research opportunities and challenges. They underscored the need for innovative solutions to overcome obstacles such as waste handling and material safety.
In the Journal of Environmental Management, Kumar, Kumar, and Gupta [5] discussed the current state of medical waste management and proposed sustainable strategies for utilizing this waste in the construction industry. They highlighted the environmental and public health benefits of sustainable medical waste management. Finally, Katti and Babu [6], in their article published in the Journal of Building Engineering, reviewed research on the potential for using medical waste in construction materials. They emphasized the need for further research to address the challenges and limitations of this approach, while also recognizing its potential environmental benefits. Li et al. [7] explored the use of medical waste as a raw material for lightweight aggregate production. Their findings revealed that medical waste could be transformed into lightweight aggregate with high strength and low water absorption, demonstrating its potential as a sustainable option for waste disposal in the construction industry.
Materials and Methods
A comprehensive waste management plan was proposed, outlining the process from waste generation, collection, and transportation to recycling, treatment, recovery, and disposal, with special consideration for the pandemic situation. The material flow was carefully structured to minimize human interaction with contaminated waste, reducing the risk of exposure by decontaminating the waste immediately after collection. Contaminated PPE waste was collected from healthcare facilities and subjected to a decontamination process, which involved thorough washing and drying of the materials. After decontamination, the processed waste was stored for a minimum of 28 days. These three stages- collection, decontamination, and storage-were identified as high-risk zones for potential virus exposure. To mitigate these risks, waste handlers were required to follow strict PPE and safety protocols. Once the storage period was complete, the materials were transferred to a shredder unit, where they were shredded and densified into small pieces for further processing. The shredded material was then mixed with fillers and heated to approximately 180°C. Following this, the heated polymer-filler mixture was pressed in a hydraulic press to form building blocks and pavement tiles, as outlined in the materials section.
Waste Materials
Medical waste is generated from a range of activities, including general medical treatment, clinical investigations, food preparation, and ward operations. The volume of medical waste produced depends on several factors, such as the hospital’s size, the level of equipment used, and occasionally the location of the medical facility. The composition of medical waste typically reflects the nature of its source. Different departments within hospitals and clinics generate distinct types of waste. Additionally, various scattered sources can produce medical waste similar in nature to hospital waste [8].
Compressive Strength
Compressive strength refers to the ability of a material or structure to resist or withstand forces under compression. It is determined by the material’s capacity to resist failure in the form of cracks or fractures. The compressive strength of concrete is often measured through a cube test, which provides insight into the overall characteristics of the concrete [9, 10, 11, 12, 13, 14, 15]. This test helps assess whether the concreting process was executed correctly. For general construction, concrete compressive strength typically ranges from 15 MPa (2,200 psi) to 30 MPa (4,400 psi), with higher strengths used in commercial and industrial buildings. Several factors influence the compressive strength of concrete, including the water-cement ratio, cement quality, quality of the concrete materials, and the level of quality control during production. The compressive strength test is usually performed on either a cube or cylinder sample of the concrete [16, 17, 18].
Test concrete for 7days, 14days and 28 days
Concrete reaches its maximum strength at 28 days. However, since significant capital is involved in the construction industry, it’s more practical to assess concrete strength at 7 and 14 days to predict whether it will meet the target strength at 28 days. From the table below, it’s evident that concrete gains about 16% of its strength within the first 24 hours, 65% by 7 days, and around 90% by 14 days. After 14 days, the strength gain slows, with concrete achieving approximately 99% of its target strength by 28 days. It is essential to allow the concrete to stabilize before accurately judging its strength. While we cannot wait for 28 days to determine if the concrete is suitable for construction, testing concrete strength at various intervals, such as 7 and 14 days, helps ensure that the construction process stays on track [19].
| 1Day | 16% |
|---|---|
| 3Days | 40% |
| 7Days | 65% |
| 14Days | 90% |
| 21Days | 94% |
| 28Days | 99% |
Table 2: Percentage of Strength.
Cement
In the present study, a single batch of Portland Pozzolana Cement (PPC), fly ash-based, was used, conforming to the IS 1489 (Part I): 1991 specifications. Cement serves as a binder in construction, a material that sets, hardens, and adheres to other substances, effectively binding them together. While rarely used on its own, cement is commonly mixed with sand and gravel (aggregate) to form various construction materials. It is combined with fine aggregates to create mortar for masonry or with sand and gravel to produce concrete. In this case, Ordinary Portland Cement (OPC) was utilized [20].

Fine Aggregate
| Materials | OPC | Hospital Waste Ash |
|---|---|---|
| Specific Gravity | 3.05 | 2.71 |
| Silicon Dioxide (SiO )(%) 2 | 17.454 | 19.603 |
| Aluminum Oxide (A1 O )(%) 2 3 | 4.422 | 10.377 |
| Ferric Oxide (Fe O )(%) 2 3 | 3.93 | 6.273 |
| Calcium Oxide (CaO)(%) | 65.844 | 36.636 |
| Magnesium Oxide (MgO)(%) | 2.346 | 2.136 |
| Sulfur Trioxide (SO ) (%) 3 | 3.979 | 5.589 |
| Sodium Oxide (Na O)(%) 2 | 0.252 | 2.697 |
| Potassium Oxide (K O)(%) 2 | 1.117 | 0.701 |
| TiO (%) 2 | 0.348 | 3.395 |
| P O (%) 2 5 | 1.03 | 1.167 |
| Cl (%) | 0.012 | 5.370 |
| SrO (%) | 0.072 | 0.044 |
| MnO (%) | 0.064 | 0.123 |
| ZnO (%) | - | 5.370 |
| CuO (%) | - | 0.044 |
Table 1: Fly ash-based, was used, conforming.
Coarse Aggregate
Crushed stone with a maximum nominal size of 19 mm was used as coarse aggregate in this study. Coarse aggregates are particles larger than 4.75 mm, typically ranging between 9.5 mm and 37.5 mm in diameter. These aggregates can come from primary, secondary, or recycled sources and are essential components in various areas of construction. They serve structural purposes, such as forming base layers or drainage layers beneath pavements, and are commonly used in mixtures like asphalt and concrete. Coarse aggregates are sourced from rock quarries or dredged from riverbeds, and their size, shape, hardness, texture, and other properties can vary significantly depending on their origin. Even materials from the same quarry or type of stone may exhibit substantial differences. Generally, coarse aggregates are categorized as either smooth or rounded (like river gravel) or angular (such as crushed stone). Due to this variability, standardized testing methods are used to assess their key characteristics, as precise identification is difficult. Some of the most important properties used to describe coarse aggregates include relative density, which helps predict their behavior in construction applications [21].

Hospital Waste
Hospital waste ash was collected from SIMS Hospital in Bilaspur, Chhattisgarh. The ash consisted of a mixture of fine and coarse particles, including broken glass bottles, metallic fragments, syringes, and other surgical items, as illustrated in the accompanying image. The ash mixture was passed through a No. 50 sieve, and the retained material was discarded [22].

Mixing of Concrete
The ingredient must not be rotated for morethan2 minute sand the following pattern must be followed. M20 Concrete: 1:1.5:3 mixture of cement, sand, and aggregate + Addition of Medical Waste Ash 300g of Ash is replaced with 300g of cement for cube 1And150gofAshisreplacedwith150gofcement for cube2 100g of Ash is replaced with 100g of cement for cube 3.

Procedure
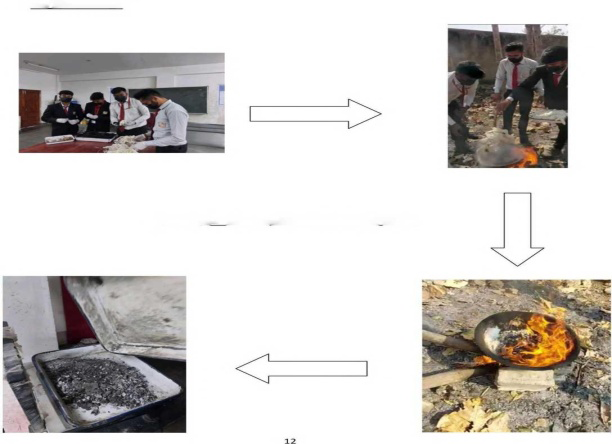
The process outlined above consists of the following steps:
- Separation: The first step involves sorting and separating items such as masks, drip bottles, and drip bandages.
- Ignition: In the second step, the sorted materials are placed into a pot and ignited.
- Burning: The materials are then burned until they begin to melt. This process is maintained for approximately 40 to 50 minutes until the materials are fully converted into ash.
- Collection: The final step is to collect the ash once the pot has cooled down.
Procedure of casting cubes
- Mix Preparation: Combine the medical waste ash with the concrete mix, and then pour the prepared concrete mixture into a steel cube mold for casting.
- Mold Removal: After the concrete has set for 24 hours, carefully remove the concrete cube from the mold.
- Submersion: Submerge the test specimens in water for the required duration.
- The specimen should be submerged in water for either 7, 14, or 28 days, with the water being changed every 7 days.
- Ensure that the concrete specimen is thoroughly dried before placing it on the Universal Testing Machine (UTM).
- The weight of the samples must be recorded prior to testing, and it should not be less than 8.1 kg.
- Testing specimens should be positioned between the bearing surfaces.
- Care must be taken to remove any loose material or grit from the metal plates of the machine and the specimen block.
- The concrete cubes should be placed on the bearing plate and aligned correctly with the center of thrust between the testing machine plates.

Results and Discussion
The comprehensive review of the sustainable utilization of medical waste in the construction industry has yielded several key findings that highlight the potential benefits, challenges, and future directions of this innovative approach [23, 24].
Characterization of Medical Waste
The analysis identified various types of medical waste suitable for repurposing in construction, including plastics, metals, glass, and certain organic materials. Each category was evaluated for its physical and chemical properties to determine its feasibility as a construction material.
- Plastics: The review noted that sterilized plastic waste can be used as an aggregate substitute in concrete, enhancing its durability and resistance to water.
- Glass: Crushed glass from medical containers demonstrated potential as a lightweight aggregate, contributing to reduced concrete density while maintaining strength.
- Metals: Metals from medical equipment, when processed properly, can be recycled for use in structural applications, thus conserving raw materials [25].
Environmental Impact
Incorporating medical waste into construction has significant environmental implications:
- Waste Reduction: Utilizing medical waste can divert substantial amounts from landfills, addressing the growing issue of medical waste management.
- Resource Conservation: The substitution of conventional materials with medical waste can reduce the demand for natural resources, such as sand and gravel, contributing to the preservation of ecosystems.
- Carbon Footprint: The life cycle assessment of construction materials revealed that using medical waste can lead to lower greenhouse gas emissions, particularly when considering the energy-intensive processes involved in producing traditional construction materials [26].
Mechanical Performance of Construction Materials
The review encompassed various studies that evaluated the mechanical properties of construction materials incorporated with medical waste:
- Concrete Strength: Research findings indicate that concrete mixtures with up to 20% replacement of natural aggregates with sterilized plastic waste exhibited comparable compressive strength to conventional concrete [27].
- Durability: The incorporation of medical waste, particularly glass, has been shown to enhance the durability of concrete against environmental factors, such as freeze-thaw cycles and chemical attacks.
Economic Viability
The economic analysis highlighted several advantages of using medical waste in construction:
- Cost Savings: Utilizing waste as a raw material can lead to cost reductions in construction projects, particularly in regions facing high disposal fees for medical waste.
- Job Creation: The development of new recycling facilities and processing centers for medical waste can create job opportunities and stimulate local economies [28].
Challenges and Considerations
Despite the promising results, several challenges must be addressed:
- Safety and Health Concerns: Ensuring that medical waste is adequately sterilized and poses no health risks during processing and use is paramount. Establishing standardized protocols for handling and recycling is essential.
- Regulatory Framework: Current regulations may not fully support the use of medical waste in construction. Policy adjustments are necessary to facilitate this innovative approach.
- Public Perception: There may be public resistance to using materials derived from medical waste in construction due to perceived safety concerns. Education and transparency about the processing methods can help alleviate these fears.
Future Directions
The review emphasizes the need for further research to explore:
- Long-term Performance: Longitudinal studies assessing the durability and structural integrity of materials incorporating medical waste over time.
- Innovative Processing Technologies: Development of new technologies that can efficiently and safely process medical waste for construction purposes.
- Life cycle Assessments: Comprehensive lifecycle assessments to quantify the environmental benefits and economic feasibility of medical waste utilization in construction.
Conclusion
In conclusion, the sustainable utilization of medical waste in the construction industry presents a promising solution to the growing challenges of medical waste disposal. Research shows that incorporating medical waste as a partial substitute for traditional construction materials like cement and aggregates can enhance compressive strength, lower carbon emissions, and reduce water absorption. This innovative approach not only mitigates the environmental burden of medical waste but also offers significant economic and ecological advantages. However, the safe and sustainable integration of medical waste into construction requires the development of effective strategies, including proper waste segregation and handling. Addressing these challenges is crucial for wider adoption. Future research should focus on discovering new techniques for incorporating medical waste into construction materials and establishing clear guidelines and regulations to ensure its safe and sustainable use.
Future Scope
- Development of innovative technologies to convert medical waste into construction materials: There is a need to develop and improve technologies that can convert medical waste into sustainable construction materials such as bricks, blocks, and tiles.
- Collaboration between the medical and construction industries: Collaboration between the medical and construction industries can lead to the efficient and sustainable use of medical waste. This can be achieved through joint research and development, sharing of resources and expertise, and the establishment of partnerships.
- Implementation of government policies and regulations: Governments can play a crucial role in promoting the use of medical waste in the construction industry by implementing policies and regulations that encourage the sustainable use of waste and incentivize companies to invest in innovative technologies.
- Adoption of circular economy principles: The adoption of circular economy principles in the construction industry can help reduce waste and promote the sustainable use of resources. This can be achieved through the implementation of waste reduction strategies, the use of renewable energy sources, and the promotion of sustainable practices.
- Public awareness and education: Raising public awareness and educating people about the importance of sustainable waste management practices can help promote the use of medical waste in the construction industry. This can be achieved through campaigns, workshops, and educational programs.
References
-
Kavitha V (2022) Global prevalence and visible light mediated photo degradation of pharmaceuticals and personal care products (PPCPs)-a review. Results in Engineering 14: 100469.
-
Akhtar A, Sarmah AK (2018) Construction and demolition waste generation and properties of recycled aggregate concrete: A global perspective. Journal of Cleaner Production 186: 262-281.
-
Kumar M, Patel AK, Shah AV, Raval J, Rajpara N, et al. (2020) First proof of the capability of wastewater surveillance for COVID-19 in India through detection of genetic material of SARS-CoV-2. Science of The Total Environment 746: 141326.
-
Young BE, Ong SWX, Ng LF, Anderson DE, Chia WN, et al. (2020) Immunological and viral correlates of COVID-19 disease severity: a prospective cohort study of the first 100 patients in Singapore. Th Lancet: 34.
-
Gupta P, Kumar S, Suman RR, Kumar V (2020) Sentiment analysis of lockdown in india during covid-19: A case study on twitter. IEEE Transactions on Computational Social Systems 8(4): 992-1002.
-
Katti A, Kakade N, Mulani A, Mohite VR, Nazima S, et al. (2020) Effectiveness of structured teaching program in prevention of tuberculosis among HIV infected people: An observational study. International Journal of Pharmaceutical Research 12(3).
-
Li J, Liu J (2015) Recycling of medical waste into building materials: an economic analysis. Journal of Cleaner Production 93: 70-78.
-
WHO (2017) Safe management of wastes from health- care activities (No. WHO/FWC/WSH/17.05). World Health Organization, Geneva.
-
Chandra S, Kumar R (2014) Sustainable utilization of biomedical waste in construction materials: a review. Construction and Building Materials 52: 296-305.
-
Agamuthu P, Fauziah SH (2013) Sustainable management of medical waste in Malaysia: towards zero landfill. Journal of Material Cycles and Waste Management 15(4): 419-424.
-
Chen YY, Huang CH (2015) Recycling of medical waste into construction materials: a case study in Taiwan. Journal of Material Cycles and Waste Management 17(2): 228-237.
-
Huang CH, Chen YY (2015) Recycling of medical waste into environmentally friendly construction materials: a review. Journal of Cleaner Production 99: 23-37.
-
Karthikeyan S, Sridhar S (2015) Utilization of biomedical waste in construction materials-a review. Journal of Material Cycles and Waste Management 17(2): 238-252.
-
Liu J, Li J (2016) A review of the utilization of medical waste in the construction industry. Journal of Cleaner Production 112: 823-834.
-
Zhang Y, Li Q, Li H (2014) Utilization of medical waste in construction materials: status and challenges in China. Journal of Material Cycles and Waste Management 16(4): 573-580.
-
Ekanayake LL, Kulatunga U (2013) Sustainable management of medical waste in developing countries: a review. Waste Management & Research 31(8): 785-802.
-
Khetriwal DS, Sharma A (2015) Sustainable management of biomedical waste in India: a review. Journal of Material Cycles and Waste Management 17(1): 1-10.
-
Kumar V, Kumar A (2015) Biomedical waste management in India: critical appraisal. Journal of Material Cycles and Waste Management 17(1): 1-10.
-
Lohani B, Das S (2014) Medical waste management in India: a review. International Journal of Environmental Science and Development 5(5) 494-498.
-
Singh A, Jain RK, Jain S (2015) Biomedical waste management: a review. Journal of Material Cycles and Waste Management 17(1): 1-9.
-
Tchobanoglous G, Theisen H, Vigil S (1993) Integrated solid waste management: engineering principles and management issues. McGraw-Hill, New York.
-
UNEP (2004) Guidelines for the environmentally sound management of wastes consisting of, containing or contaminated with persistent organic pollutants. United Nations Environment Programme, Geneva.
-
EPA (2016) Medical waste. United States Environmental Protection Agency.
-
EC (2014) European waste hierarchy. European Commission.
-
Ministry of Environment and Forests (2016) Biomedical waste management rules, 2016. Government of India.
-
WHO (2005) Safe management of wastes from health- care activities. World Health Organization, Geneva.
-
UNEP (2013) The globale-waste monitor -2014. United Nations Environment Programme, Geneva.
-
Li C, Yang Y, Ren L (2020) Genetic evolution analysis of 2019 novel coronavirus and coronavirus from other species. Infection, Genetics and Evolution 82: 104285.
- Lessons to Learn: Trees are More than the Lungs of the World
- Community Forestry Enterprises as a Model for Sustainable Forest Development: The Case Of The "Baja Tarahumara" in Chihuahua, Mexico
- Ecological and Socio-Economic Impacts of Chromolaena odorata and Mesosphaerum suaveolens, Two Invasive Alien Species in Central and Southern Benin, West Africa
- Epigenetic Sustainability: Modeling the Human Factor as a Natural Resource through Science 4.0 and the NR3C1 Biological Pilot
- Growth-at-Risk: A Framework for Assessing Economic Vulnerability
- The Rural Territory as a Socioecological System for the Management of Public Policy for Sustainable Rural Development