Anatomical Variations of Internal Iliac Artery and Internal Iliac Vein and their Clinical Significance
Pelvic cavity is bounded by three bilateral pairs of bones (pubis, ilium and ischium) and two posteriorly located bones (sacrum and coccyx). Different organs lie in complicated juxtaposition in the pelvic cavity, including vessels, nerves, muscles, urogenital organs, and the rectum. Such configurations of these organs are difficult to comprehend for many surgeons to perform advanced surgery for cancers that arise in urological, gynecological organs or rectal cancer. Also procedure like sacrectomies and lateral pelvic compartment exenterations, isolating the external and internal iliac veins within the presacral area is crucial to avoid inadvertent injury and severe hemorrhage. This study review anatomic variations of internal iliac artery and internal iliac vein and their clinical significance. We found some rare patterns, which should be considered during surgery. These will benefit our understanding of pelvic anatomy and enhance safety in performing radical surgery for treating pelvic diseases; increase knowledge regarding the internal iliac artery and its branches is helpful in applying ligatures safely during pelvic surgeries which is essential to minimize intraoperative blood loss and other complications.
Background
Pelvic cavity is formed by three bilateral pairs of bones (pubis, ilium and ischium) and two posteriorly located bones (sacrum and coccyx). The cavity is primary home to the some of the urinary organs, most of the reproductive organs and the distal part of the digestive tract in humans like pelvic colon and rectum [1]. Different organs lie in complicated juxtaposition in the pelvic cavity, including vessels, nerves, muscles, urogenital organs, pelvic colon and rectum [2, 3, 4]. Such configurations of these organs are difficult to understand for many surgeons to perform advanced surgery for cancers that arise in urological, gynecological organs, colon or rectal cancer [5]. Also procedure like sacrectomies, lateral pelvic compartment exenterations, isolating of external and internal iliac veins within the presacral area is crucial to avoid inadvertent injury and severe hemorrhage [6]. It is necessary to have an accurate, comprehensive understanding of pelvic anatomy and intrapelvic vessels with their branching and tributaries or relations of vessels in relation to sacral plexus to perform safe and appropriate surgery. However, in addition to the complexity of the pelvic cavity, many anatomical variations, particularly vascular patterns and relation to the course of sacral plexus, make it even more difficult to understand. There is a paucity of literature concerning the anatomical variations of the internal iliac artery, internal iliac veins, or sacral plexus. Thus, we aim to review the current literature with regards anatomical variations of intrapelvic vessels, inter-relationships among intrapelvic vessels and their clinical significance.
Anatomical Variations of Internal Iliac Artery
The abdominal aorta is divided into right and left at the level of the 4th-5th lumbar vertebra and called the common iliac artery (CIA). Anterior to the sacroiliac joint, the common iliac arteries are divided into external and internal iliac arteries. The external iliac artery supplies the lower limb and internal iliac artery (IIA) is the major vascular supply of the pelvis [7]. The internal iliac artery is one of the two divided parts of the common iliac artery; it passes medially over the pelvic brim and runs downward to the pelvic cavity [1]. At the upper margin of the greater sciatic foramen, it has anteriorly and posteriorly division. The ureter stands at the medial aspect of internal iliac artery; the para rectal space is noted between the ureter and the internal iliac artery. It is the main blood supply to the pelvic organs like (urogenital organs, some urinary organs), gluteal muscles, and perineum, with the anterior (visceral supply) and posterior (parietal supply) trunks. The visceral branches of the anterior division are superior vesical artery (SVA), inferior vesical artery (IVA), middle rectal artery (MRA), uterine and vaginal arteries. The last two branches are present in females, where in the vaginal artery replaces the inferior vesical artery (IVA). The parietal branches of the anterior division are obturator artery (OBA), inferior gluteal artery (IGA), and internal pudendal artery (IPA). The branches from the posterior division are all parietal, namely, iliolumbar artery (ILA), lateral sacral artery (LSA), and superior gluteal artery (SGA)(1)(Figure 1).
![Figure 1: Right internal iliac artery dissection, superior view [7].](/fulltextimages/5576/fig_1.png)
There is an important and increased potential anatomic variation for the internal iliac artery (IIA), especially at the end of branching of internal iliac artery. Reasons for these arterial variations are multifactorial or many factors that contribute to anatomical variation. It may be due to hemodynamic forces, fetal position in the uterus/Womb, genetic factors and the result of developmental anomalies during the formation of blood vessels(8). The Branching pattern of internal iliac artery was classified as per modified Adachi classification (Figure 2).
Adachi Types
Type I: The superior gluteal artery (SGA) arises from the internal iliac artery and Inferior gluteal and internal pudendal vessels are given off by a common trunk. The latter two divides within the pelvis. It is considered as Type Ia, whereas the bifurcation occurs below the pelvic floor it is classified as type Ib.
Type II: The superior gluteal artery and the Inferior gluteal arteries arise by a common trunk and the internal pudendal vessels separately.
Type II a: Type IIa which the trunk common to the two gluteal arteries divides within the pelvis and Type IIb in which the division occurs outside the pelvis.
Type III: The Three branches arise separately from internal iliac artery (IIA).
Type IV: Three arteries arise by a common trunk.
Type IVa the trunk first gives rise to the superior gluteal artery before bifurcating in to the other two branches.
Type IVb the Internal pudendal is the first vessel to spring the common trunk. Then divides into superior and inferior gluteal arteries.
Type V: The Internal pudendal and superior gluteal arteries arise from a common trunk and the Inferior gluteal has a separate origin. Material and methods.
![Figure 2: Adachi’s types of IIA variations. IIA: internal iliac artery; IGA: Inferior gluteal artery; IPA: Internal pudendal artery; SGA: Superior gluteal artery; UA: Umbilical artery [9].](/fulltextimages/5576/fig_2.png)
Clinical significance
Internal iliac artery is principal artery that supplies the pelvis; therefore, to perform surgery in pelvis region like prophylactic bilateral internal iliac artery ligation. Accidental arterial injury need knowledge of arterial pattern is essential for surgeon. Currently endovascular therapy for pathological condition like aneurysm is available. Internal iliac artery aneurysm can be treated with Cather based techniques by injecting embolization and other thrombogenic material into aneurismal sac and its branches. Ligation of internal iliac artery (IIA). Has been used to control serious obstetric and pelvic hemorrhage. Ligation of anterior division of internal iliac artery is being restored to produce pelvic compartment hypotension to control extensive pelvic hemorrhaging vessel. The superior gluteal artery perforator flap can be transferred pedicle to treat sacral pressure sores or to be transferred freely for breast reconstruction. Coil embolization therapy for uterine fibroid tumor/cancer or any major uterine malignancy may reduce the chance of infertility in young patient. The fact that internal iliac artery has extensive area of supply and is of great surgical importance.
Obliterated Umbilical Artery
It is a branch of internal iliac artery and an important anatomic landmark to identify the uterine artery, especially during laparoscopic procedures (Figure 1). Moreover, it is in close relation with para-vesical space and it divides the paravesical space into two parts. When traction is applied where it attaches to the anterior abdominal wall, it indicates the uterine artery. The superior vesical artery (SVA) arises from the proximal part of the umbilical artery, which supplies the upper part of the bladder. The inferior vesical artery (IVA) supplies the base of the bladder; however, it is not possible to detect it during every dissection every dissection. It is also called the vaginal artery. The umbilical artery becomes the medial umbilical ligament when it reaches the anterior abdominal wall.
Uterine Artery
The uterine artery arises from the anterior division of the internal iliac artery (IIA) and goes anteromedially to the lateral part of uterine cervix below the isthmic part of uterus, where it crosses the ureter superiorly (Figure 1). It begins between the origins of the obturator and umbilical arteries; however, sometimes it may have a common trunk with the superior vesical artery (SVA). The uterine artery runs between the anterior and posterior layer of broad ligament, above the cardinal ligament. It anastomoses with the ovarian artery and also gives a vaginal branch.
Clinical Significance: During hysterectomy/total removal of the uterus from the obliterated umbilical artery is one way to identify the uterine artery. Another method is to follow the ureter to the point where it crosses under the uterine artery. Moreover, after opening the retroperitoneal region on the pelvic sidewall, antero-medial dissection of internal iliac artery may show the uterine artery.
Obturator Artery
The obturator artery(OBA) runs antero-infero-laterally on the obturator fascia and exits from the pelvis through the obturator foramen [7]. The origin of the obturator artery varies; however, it mostly arises near the origin of the umbilical artery. It goes just under the obturator nerve and anastomoses with the inferior epigastric artery or external iliac artery via the pubic branch (corona mortis); in the pelvis, the obturator artery gives rise to the pubic branch it leaves the pelvis from the obturator foramen [1] (Figure 3).
![Figure 3: The obturator artery arising from the anterior trunk of the internal iliac artery. CIA: common iliac artery; EIA: external iliac artery; IIA: internal iliac artery; IEA: inferior epigastric artery; OA: obturator artery [10].](/fulltextimages/5576/fig_3.png)
Clinical significance: An aberrant (accessory obturator artery), a variation, may arise from the external iliac artery and runs to the obturator foramen [11].
Corona Mortis
Some individuals can have anastomosis between iliac arteries and obturator vessels in the retro pubic region that can be of arterial or of venous profile, or both [12]. Such arterial/ anastomosis called(corona mortis) or venous anastomosis is especially significant in the ilioinguinal approach (treatment of acetabulum fracture) and with the use of the modified Stoppa approach [13]. Because its section or rupture due to traction by the isolated ramus can cause great bleeding due to the difficulty to find the arterial segment that recoils in the region of the obturator vessels. Therefore, surgical orthopedists and other specialists such as obstetricians, gynecologists and gastroenterologists (while repairing groin hernia) should take these probabilities into account [10]. If the anastomosis is carefully identified, it can be given prophylactic ligature to avoid such devastating complication [14, 15, 16, 17] (Figure 4).
![Figure 4: Corona mortis, Lateral view [18].](/fulltextimages/5576/fig_4.png)
Internal Pudendal Artery
Internal pudendal artery runs inferolaterally, anterior to
the piriformis muscle and sacral plexus (Figures 5a & 5b). It passes through the greater sciatic foramen along the posterior aspect of the ischial spine close to the sacrospinous ligament and enters the ischioanal fossa through the lesser sciatic foramen. Injury of the internal pudendal artery could be managed by compression on the ischiorectal/ischioanal fossa. The internal pudendal artery gives rise to the dorsal artery of clitoris [19].
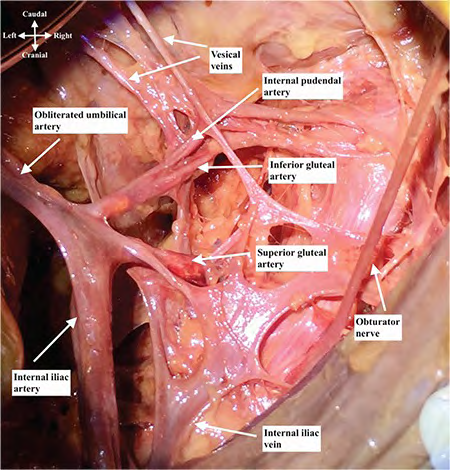
A B Figure 5: Right Internal artery dissection showing internal pudendal artery, lateral view.
Inferior Gluteal Artery
This passes between the sacral nerves, usually S1 and S2, sometimes S2 and S3 and leaves the pelvis through the greater sciatic foramen below the piriformis muscle (Figure 5a). The inferior gluteal artery is also a danger zone during sacrospinous ligament fixation [1].
Anatomical Variations of Internal Iliac Vein
The common iliac veins (CIV) are formed by the junction of the internal and external iliac veins. The internal iliac veins ascend from the pelvis with various tributaries that correspond to the branches of the internal iliac artery, while the external iliac veins are the upward continuation of the femoral veins which is venous drainage from the lower limb [1]. The position of the iliac veins is named according to the corresponding arteries [20]. In this review anatomical location of the common iliac veins, location of internal iliac veins formation, and distance between right and left CIVs varied in each individual [21].
Clinical Significance
The variations of the iliac veins and their relationships can be important in retroperitoneal surgical interventions such as the superior hypogastric, neurectomy and hysterectomy as well as in the interpretation of the pelvic imaging, particularly in the computed tomography (CT) scanning or in the magnetic resonance [22].
The anatomical variations and the congenital anomalies of the iliac veins were indicated on the Figure below (6). Among the numerous variations of internal iliac veins, the right and the left internal iliac veins usually drain towards the contralateral external iliac vein. In type I, one internal iliac vein drained into the ipsilateral common iliac vein in both halves of the pelvis; in type II, two internal iliac veins drained into the ipsilateral common Iliac vein in one or both halves of the pelvis; in type III, one of the two internal ilia veins drained into the contralateral common Iliac vein, and the other drained into the ipsilateral common iliac vein; and type IV comprised all variations in internal iliac veins patterns that did not fit into types I-III. Additionally, type II was sub classified into three subtypes: in type IIa, two internal iliac veins were present in the left half of the pelvis; in type IIb, two internal iliac veins were present in the right half of the pelvis; and in type IIc, two internal iliac veins were present in both halves of the pelvis. Similarly, type III was classified into two subtypes: in type IIIa, one internal iliac veins draining toward the ipsilateral cavity ran from the right cavity into the left common iliac veins; in type IIIb, it ran from the left cavity into the right common iliac vein (Figure 6).
![Figure 6: Variations in the branching pattern of the internal iliac vein. IVC, inferior vena cava; CIV, common iliac vein; IIV, internal iliac vein; EIV, external iliac vein [5].](/fulltextimages/5576/fig_6.png)
Relationships between Sacral Plexus, Internal Iliac Artery, and Internal Iliac Vein
The sacral plexus are a network of nerve fibres that innervate the cutaneous and muscles of the pelvis/perineum and lower limb. It is located on the surface of the posterior pelvic wall, anterior to the piriformis muscle. This network of nerve fibers is formed by the anterior rami (divisions) of the sacral spinal nerves S1, S2, S3 and S4. It also receives contributions from the lumbar spinal nerves L4 and L5 [1].
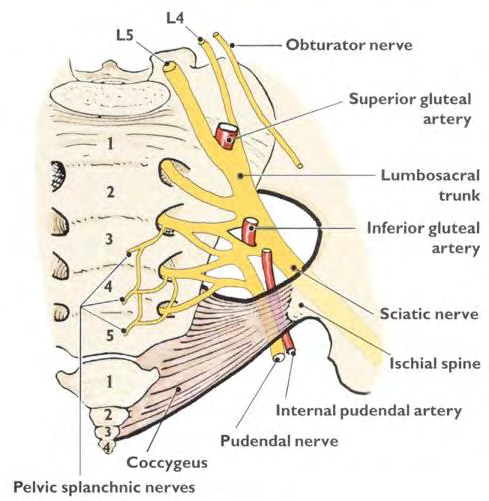
The Superior gluteal artery is branch of internal iliac artery pass between the L5 and S1 branches of sacral plexus.
Runs dorsal, on the lateral side of the internal iliac vein and on the medial side of the internal iliac vein. Superior gluteal vein is a tributaries of internal iliac veins passed through the routes lateral to L5, between the L5 and S1, and between the S1 and S2 [4] (Figure 7).
Conclusion
This study review anatomic variations of internal iliac artery and internal iliac vein. We found some rare patterns, which should be considered during surgery. These will benefit our understanding of pelvic anatomy and enhance safety in performing radical surgery for treating pelvic diseases; increase knowledge regarding the internal iliac artery and its branches is helpful in applying ligatures safely during pelvic surgeries which is essential to minimize intraoperative blood loss and other complications.
Many surgeons probably consider this configuration to be typical pelvic anatomy, and they might implement surgery based on that assumption. Understanding the above vascular variations might be valuable to prevent inadvertent intraoperative bleeding from the internal iliac vessels in such advanced surgeries.
This review suggested that, although many anatomic variations are present in the pelvis, pelvic anatomies are not likely to arise at random. These facts might facilitate the evaluation and detection of anatomic variations in the pelvis with more precision, in advance of surgery.
Conflict of Interest
There are no conflicts of interest for the authors of this article.
References
-
Standring S (2016) Gray’s Anatomy. The Anatomical Basis of Clinical Practice, Elsevier.
-
Mohamadi Y, Toolee H, Hassanzadeh G (2016) Bilateral Variation of Internal Iliac Artery. Anat Sci J 13(3): 197- 199.
-
Francis YM, Balaji T, Rajila Rajendran HS, Gnanasundaram V, Subramanian A, et al. (2018) Study on variations in the origin and branching pattern of internal iliac artery in cadavers. Biomed Pharmacol J 11(4): 2201-2207.
-
Morita S, Saito N, Mitsuhashi N (2007) Variations in internal iliac veins detected using multidetector computed tomography. Acta Radiol 48(10): 1082-1085.
-
Hamabe A, Harino T, Ogino T, Tanida T, Noura S, et al. (2020) Analysis of anatomical variations of intrapelvic vessels for advanced pelvic surgery. BMC Surg 20(1): 9-13.
-
Sakthivelavan S, Aristotle S, Sivanandan A, Sendiladibban S, Felicia Jebakani C (2014) Variability in the Branching Pattern of the Internal Iliac Artery in Indian Population and Its Clinical Importance. Anat Res Int 2014: 1-6.
-
Selçuk İ, Yassa M, Tatar İ, Huri E (2018) Anatomic structure of the internal iliac artery and its educative dissection for peripartum and pelvic hemorrhage. Turk Jinekoloji ve Obstet Dern Derg 15(2): 126-129.
-
Kumari S, gowda MT (2016) The Branching Pattern of the Internal Iliac Artery in South Indian Population. Int J Anat Res 4(4): 2907-2913.
-
A AS (2017) Variation in the Arterial Branching Pattern of Internal Iliac Artery In human cadavers (South Indian Population). J Med Sci Clin Res 5(9): 27761-27767.
-
Al Talalwah W (2016) A new concept and classification of corona mortis and its clinical significance. Chinese J Traumatol 19(5): 251-254.
-
Berberoglu M, Uz A, Özmen MM, Bozkurt C, Erkuran C, et al. (2001) Corona mortis: An anatomic study in seven cadavers and an endoscopic study in 28 patients. Surg Endosc 15(1): 72-75.
-
Shereen R, Lee S, Salandy S, Roberts W, Loukas M (2019) A comprehensive review of the anatomical variations in the right atrium and their clinical significance. Transl Res Anat 17: 100046.
-
Guo HZ, He YF, He WQ (2019) Modified stoppa approach for pelvic and acetabular fracture treatment. Acta Ortop Bras 27(4): 216-219.
-
Cação Pereira GJ, Nicoletti Gumieiro D, Innocenti Dinhane D, Sardenberg T, De Almeida Silvares PR, et al. (2018) Anastomosis entre vasos ilíacos y obturadores en la región retropúbica: estudio en cadáveres. [Anastomosis among iliac vessels and obturators in the retropubic region: Study in cadavers]. Rev la Asoc Argentina Ortop y Traumatol 83(3): 205.
-
Okcu G, Erkan S, Yercan HS, Ozic U (2004) The incidence and location of corona mortis: A study on 75 cadavers. Acta Orthop Scand 75(1): 53-55.
-
Sarikcioglu L, Sindel M, Akyildiz F, Gur S (2003) Anastomotic vessels in the retropubic region: Corona mortis. Folia Morphol (Warsz). 62(3): 179-182.
-
Kim HY, Yang DS, Park CK, Choy WS (2015) Modified stoppa approach for surgical treatment of acetabular fracture. CiOS Clin Orthop Surg 7(1): 29-38.
-
Papagrigorakis E, Gkarsioudis K, Skandalakis P, Filippou D (2018) Corona Mortis: Surgical Anatomy, Physiology and Clinical Significance. Int J New Technol Res 4(3): 263111.
-
Kawanishi Y, Muguruma H, Sugiyama H, Kagawa J, Tanimoto S, et al. (2008) Variations of the internal pudendal artery as a congenital contributing factor to age at onset of erectile dysfunction in Japanese. BJU Int 101(5): 581-587.
-
Cardinot TM, Aragão AHBM, Babinski MA, Favorito LA (2006) Rare variation in course and affluence of internal iliac vein due to its anatomical and surgical significance. Surg Radiol Anat 28(4): 422-425.
-
Akhgar J, Terai H, Rahmani MS, Tamai K, Suzuki A, et al. (2016) Anatomical location of common iliac veins at the level of sacrum-perforation risk is related to the trajectory angle of screw. Eur Spine J 25: S348.
-
Wong L, Rao S, Barton DPJ (2003) Transvaginal tamponade for intra-operative pelvic haemorrhage in gynaecological oncology patients. BJOG An Int J Obstet Gynaecol 110(7): 707-709.
- Pattern of Breast Lesions in Ovu Inland, Delta State, South Southern Nigeria
- Morphometric Analysis of the Human Femur: Exploring Platymetric and Robusticity Indices Among the Nigerian Population
- Anatomical Variation of Arteria Lusoria: Clinical Implications for Dysphagia Lusoria and Surgical Risk
- Morphometric Study of the Vertebral Body and Pedicle of Typical Cervical Vertebrae Using Radiological Image
- Epigenetic Mechanisms Driving Human Evolutionary Changes
- Neuroprotective Effects of Ginkgo Biloba Extract on Bilateral Common Carotid Artery Ischaemic Stroke Induced in Wistar Rat