Study of Variations in the Morphology of Liver in the Nepalese Cadavers
Backgrounds: Liver is the largest viscera, located in the right hypochondrium, epigastrium and left hypochondrium of the abdominal cavity. It is a wedge-shaped organ with its narrow end pointed towards the left. It is convex in the front, to the right, above, and behind, and is somewhat concave inferiorly, where it is moulded to the shapes of the adjacent viscera. Even though the surface is smoothly continuous, liver is customarily apportioned by the anatomists into a larger right and a smaller left lobe by the line of attachment of the falciform ligament anteriorly and the fissure for ligamentum teres and ligamentum venosum on inferior surface. Materials and Methods: The present study was conducted on 50 formalin fixed livers and gall bladders during routine labex of undergraduate students in the dissection hall of Anatomy department of Nobel Medical College Teaching Hospitals, Biratnagar, Nepal in the period of 3 years starting from June 2016 to May 2019. Each of the specimens was studied for morphological variations. Results: In the present study the livers with normal architectures were considered normal. Out of 50 liver specimens, 21 were normal without any gross anomalies with normal architecture. The remaining 29 specimens showed some short of accessory fissures and lobes on the different lobes of the liver. Out of 29 specimens in 2 specimens lingular process was observed arising from the left lobe. Hypoplastic left lobes was also observed in 2 specimens. Conclusions: Knowledge of morphological variations like atrophy, agenesis, presence of accessory lobes and fissures, presence of intrahepatic gall bladder and absence of normal fissure and lobe can cause diagnostic error in interpretation for the anatomists, radiologists and surgeons.
Introduction
Liver is the largest viscera, located in the right hypochondrium, epigastrium and left hypochondrium of the abdominal cavity [1]. It is a wedge-shaped organ with its narrow end pointed towards the left. It is convex in the front, to the right, above, and behind, and is somewhat concave inferiorly, where it is moulded to the shapes of the adjacent viscera [2]. even though the surface is smoothly continuous, liver is customarily apportioned by the anatomists into a larger right and a smaller left lobe by the line of attachment of the falciform ligament anteriorly and the fissure for ligamentum teres and ligamentum venosum on inferior surface. In addition to the right and left lobes, there are two additional lobes called as the quadrate lobe and the caudate lobe, separated from each other by the porta hepatis. Quadrate lobe is visible on the inferior surface appears somewhat rectangular and is bounded in front by the inferior border, on the left by fissure for ligamentum teres, behind by the porta hepatis, and on the right by the fossa for the gall bladder. Tha caudate lobe is visible on the posterior surface, bounded on the left by the fissure for ligamnetum venosum, below by porta hepatis, and on the right by the groove for inferior venacava. Above, it continues into the superior surface. Below and left it has a small round papillary process [3].
The liver primordium appears in the middle of the third week as an outgrowth of the endodermal epithelium at the distal end of the foregut. This outgrowth, the hepatic diverticulum, or liver bud, consists of rapidly proliferating cells that penetrate the Septum transversum, that is, the mesodermal plate between the pericardial cavity and the stalk of the yolk sac. While hepatic cells continue to penetrate the septum, the connection between the hepatic diverticulum and the foregut (duodenum) narrows, forming the bile duct. A small ventral outgrowth is formed by the bile duct, and this outgrowth gives rise to the gallbladder and the cystic duct. During further development, epithelial liver cords intermingle with the vitelline and umbilical veins, which form hepatic sinusoids. Liver cords differentiate into the parenchyma (liver cells) and form the lining of the biliary ducts. Hematopoietic cells, Kupffer cells, and connective tissue cells are derived from mesoderm of the septum transversum [4].
Material and Methods
The present study was conducted on 50 formalin fixed livers and gall bladders during routine labex of undergraduate students in the dissection hall of Anatomy department of Nobel Medical College Teaching Hospitals, Biratnagar, Nepal in the period of 3 years starting from March 2017 to April 2019. Each of the specimens was studied for morphological variations.
Inclusion Criteria
Fresh undisected liver specimens.
Exclusion Criteria
The cirrhotic livers and livers with tumors or other pathologies.
Results
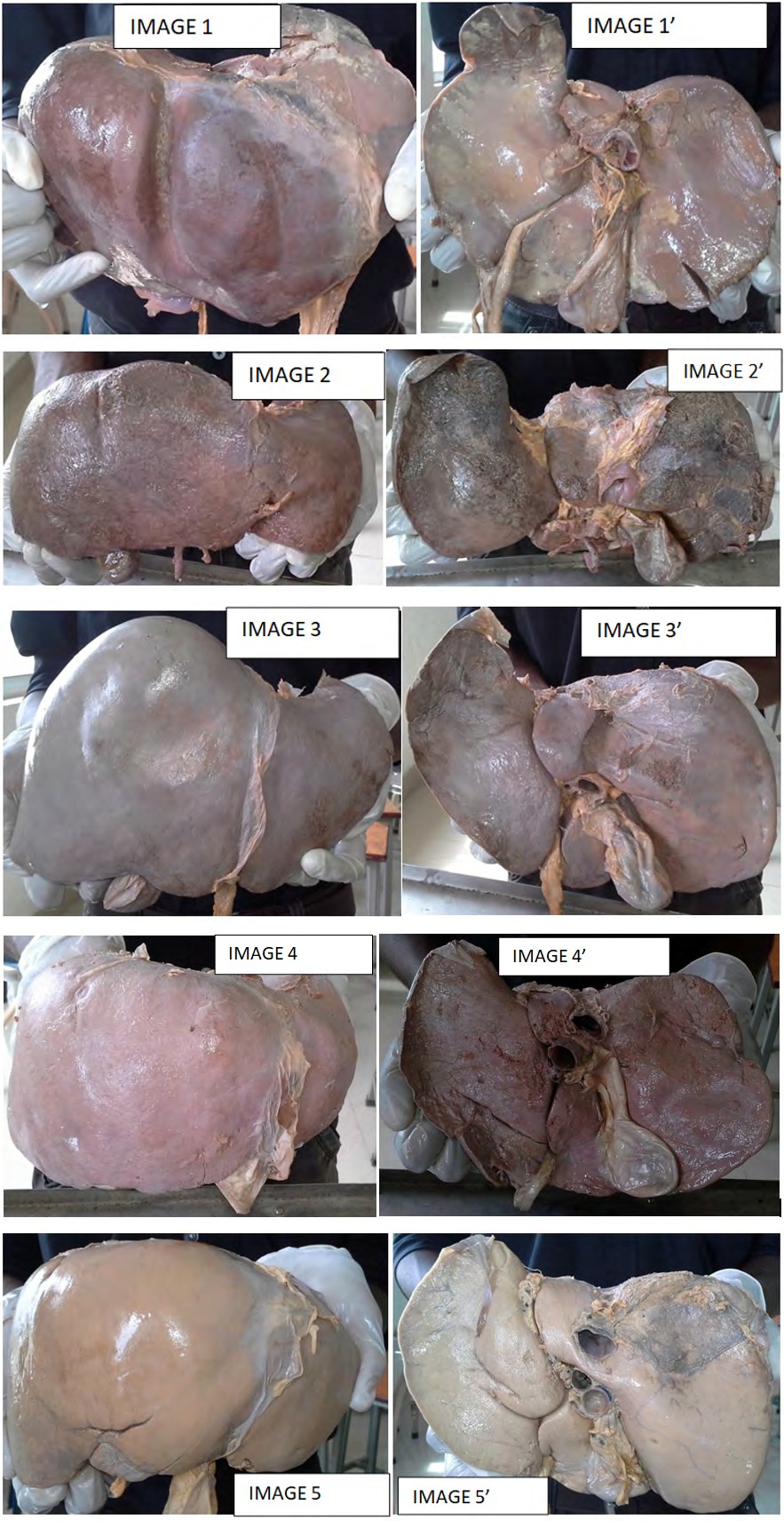
In the present study the livers with normal architectures were considered normal. Out of 50 liver specimens, 21 were normal without any gross anomalies with normal architecture. The remaining 29 specimens showed some short of accessory fissures and lobes on the different lobes of the liver. Out of 29 specimens in 2 specimens lingular process was observed arising from the left lobe (Image 1&1’). Hypoplastic left lobes was also observed in 2 specimens.
Right Lobes
On the right lobe of 9 liver specimens accessory fissures were seen in different areas of the right lobe. The fissured varied in size and shape.
Two specimens presented a goove on the superior surface formed by the diaphragm called as the diaphragmatic impression, that is, Netter type 7.
Left Lobe
The left lobe of two specimen showed a tongue like projection from the left border called as the lingular process, that is, Netter type 5.
Caudate Lobe
The caudate lobe of 5 specimens showed some type of accessory fissures and accessory lobes between the caudate process and the right lobe.
Quadrate Lobe
The quadrate lobe of two specimens presented with further lobulation and fissure on its surfaces.
Intrahepatic Gall Bladder
Out of the studied liver specimen one specimen showed the gall bladder embedded inside the quadrate lobe, which we simply called as the intrahepatic gall bladder. One specimen showed partial gall bladder embedding in the substance of right lobe of liver. So that the fundus part was not clear (Image 7&7’).

Discussion
In spite of the complex development of liver, gross abnormalities of liver are rare. The more common gross abnormalities are irregularities in the normal architecture and less common abnormality is the occurrence of one or more accessory livers or lobes. Bradely has done much to elucidate the development of liver. The single liver in some lower animals like pig and dog has distinct lobules separated by strands of connective tissue and sometimes the human liver shows this variation by reversion [5]. The congenital anomalies of liver can be divided into anomalies due to defective development and anomalies due to excessive development. Defective development of right lobe may remain latent or progress to portal hypertension, whereas defective development of left lobe of liver can lead to gastric volvulus. The excessive development of liver can may lead to formation of accessory lobes that carry the risk of torsion [6]. The acquired changes in the liver morphology are represented by the appearance of lingual lobes, costal organ with very small left lobe, deep renal impressions and local inflammation of the organ or the gall bladder [7]. Study done by TS Cullen, showed that multiple hepatic fissures and lobes were common on the undersurface of liver [8]. Study done by Vinnakota S and Jayasree N showed that 35.48% of specimens showed sparse incidence of accessory fissures in various lobes of the liver [9]. It was described that the hepatic malformations are common in perinatal age group and liver undergoes reformation postnatal. Accordingly all fissures and lobes of liver should disappear during postnatal [10]. Hussein Muktyazet, et al. found accessory liver lobes in six cadavers (14.6%), atrophy of left lobe in two cadavers, accessory fissures in five cases (12.1%) and evidence of ectopic liver tissues [11]. Pujari & Deodhare reported presence of a symptomatic accessory lobe may herniated into thorax through diaphragm and cause serious problems. He also reported a case of bifid liver presenting with anomalous quadrate and caudate lobes with transverse gall bladder [12]. In the present study out of 50 specimen’s variations was observed in 29 specimens (58%). In one of the specimen there was seen intrahepatic gall bladder along with the Riedel’s lobe.
Conclusion
Knowledge of morphological variations like atrophy, agenesis, presence of accessory lobes and fissures, presence of intrahepatic gall bladder and absence of normal fissure and lobe can cause diagnostic error in interpretation for the anatomists, radiologists and surgeons. Awareness helps to avoid fatal complications and assists in planning the better way for surgical approaches during liver resection. This knowledge also is helpful for the morphologists and embryologists to update the frequency of the variations in liver or gall bladder.
Acknowledgement
First of all I would like to thank the managing director of Nobel Medical College, Biratnagar for giving me the opportunity to carry out the study in the Department of Anatomy. And special thanks go to the supporting staffs of Anatomy Department for assisting the study by managing the liver specimens.
References
-
Rouiller C (1964) The Liver: Morphology, Biochemistry, Physiology, Academic Press, New York, NY, USA.
-
Williams PL, Warwick R, Dyson M, Bannister LH (1995) Gray’s Anatomy, 38th (Edn.), Churchilll Livingstone, Edinburg, UK.
-
Fraser CG (1952) Accessory Lobes of the Liver. Annals Surgery 135(1): 127-129.
-
Sadler TW (2011) Langman’s Medical Embryolog, pp 214.
-
Bradely OC (1908) A contribution to the morphology and development of the mammalian liver. Journal Anatomy Physiology 43(1): 1-42.
-
Daver GB, Bakhshi GD, Patil A, Ellur S, Mohit J, et al. (2005) Bifid liver in a patient with diaphragmatic hernia. Indian Journal Gastroenterology 24(1): 27-28.
-
Royer MF (1959) Vias Biliares e Pancreas, Guanabara Koogan, Rio de Janeiro, Brazil.
-
Cullen TS (1925) Accessory Lobes of the Liver. Archives of Surgery 11: 718-764.
-
Vinnakota S, Jayasree N (2013) A New Insight into the Morphology of the Human Liver: A Cadaveric Study. International Scholarly Research Notices 2013: Article ID 689564.
-
Parke WW, Settles HH, Bunger PC, Van Demark RE (1925) Malformations of the liver: some prenatal and postnatal developmental aspects. Clinical Anatomy 9(5): 718-764.
-
Hussein M, Usman N, Gupta R, Sharma KR (2013) Morphological variations of liver lobes and its clinical significance in north Indian populations. GJMMS 1(1): 1-5.
-
Pujari BD, Deodhare SG (1976) Symptomatic accessory lobes of liver with a review of the literature. Postgrad Med J 52(606): 234-236.
- Pattern of Breast Lesions in Ovu Inland, Delta State, South Southern Nigeria
- Morphometric Analysis of the Human Femur: Exploring Platymetric and Robusticity Indices Among the Nigerian Population
- Anatomical Variation of Arteria Lusoria: Clinical Implications for Dysphagia Lusoria and Surgical Risk
- Morphometric Study of the Vertebral Body and Pedicle of Typical Cervical Vertebrae Using Radiological Image
- Epigenetic Mechanisms Driving Human Evolutionary Changes
- Neuroprotective Effects of Ginkgo Biloba Extract on Bilateral Common Carotid Artery Ischaemic Stroke Induced in Wistar Rat