Anatomical Variations in the Branches of External Carotid Artery in Cadavers of Nepalese Origin
Introduction: Knowledge of the position and the variations of the external carotid artery and its branches are essential for faciomaxillary surgery and surgeries of the neck. The variations in the branching pattern are also essential to avoid complications with catheter insertion of carotid arteries in various procedures and pre-operative angiography. The external carotid artery is an important route for administration of anticancer drugs for head and neck cancer, so the knowledge of anatomy of branching pattern of external carotid artery is clinically important. Materials and Methods: Total 30 external carotid arteries were included in the present study. The dissection of the external carotid artery was carried in the dissection hall of the Anatomy Department, Manipal College of Medical Sciences. When all the branches and course of the external carotid artery was visible, variations was noted. The length of artery was measured with the help of thread, scale and vernier calliper. All the data were analyzed with Microsoft Excel 2007 software and represented as mean and standard deviation. Results: Average length of the external carotid artery from its origin by bifurcation of the common carotid artery to its termination is 8.1 cm on the right side and 8.0 cm on the left side. 40 % of the external carotid artery shows variations in the branching pattern on right side where as 53.4 % of external carotid artery shows variations on left side. Conclusion: The mean length of external carotid artery is more or less difference between right and left side. The prevalence of variations of external carotid artery was seen more on the left side as compared to the right side. The variations in the branching pattern of external carotid artery are important to the vascular surgeons as well as radiologists to prevent diagnostic errors and also to avoid complications while performing surgery in the head and neck region.
Rajeev Mukhia1*, Dil Islam Mansur2 and BP Powar3
Keywords: Cadavers; External Carotid Artery; Variations; Length
Introduction
External carotid artery is the chief artery of head, face and neck region. The external carotid artery of both sides are the branches of common carotid artery begins lateral to the upper border of lamina of thyroid cartilage, at the level with the intervertebral disc between the third and fourth cervical vertebrae [1]. As it ascends, it gives off several large branches and diminishes rapidly in calibre. At its origin, it is in the carotid triangle it lies anteromedial to the internal carotid artery. It later becomes anterior, and then lateral, to the internal carotid as it ascends. In children the external carotid is smaller than the internal carotid, but in adults the two are of almost equal size. A fingertip placed in the carotid triangle perceives a powerful arterial pulsation, which represents the termination of the common carotid and the origins of external and internal carotids [2].
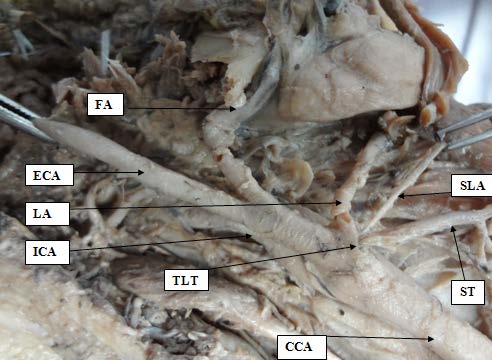
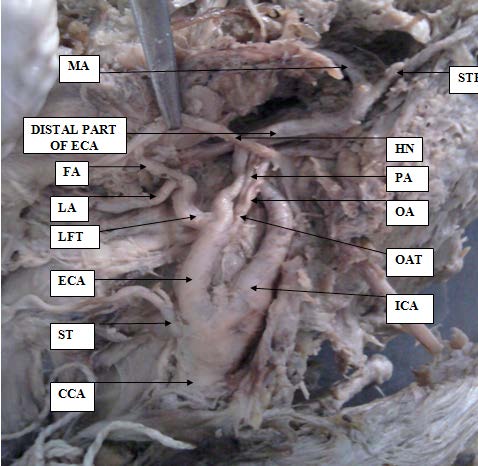
The external carotid artery (ECA) has eight named branches distributed to the head, neck and face. The superior thyroid artery (STA), lingual artery (LA) and facial artery (FA) arise from its ventral aspect, the occipital artery (OA) and posterior auricular artery (PAA) arises from dorsal aspect and the ascending pharyngeal artery (APA) arises from medial aspect. Behind the neck of the mandible, within the substance of the parotid gland, it divides into superficial temporal artery (STA) and maxillary artery (MA) as its terminal branches [3, 4].
The facial artery normally arises from external carotid artery, just above the lingual artery, at the level of greater cornu of hyoid bone in the carotid triangle. The reported variation of facial artery includes its intraparotid origin, origin as a common trunk with lingual artery as linguofacial trunk [5, 6]. Another variation in branches of external carotid artery are as follows – the lingual artery form a common trunk with the facial (lingofacial trunk) in 10-20 % cases, a rare combination branch of the external carotid artery is a thyrolinguofacial trunk [7] also reported about the presence of linguofacial trunk, thyrolingual trunk, thyrolingualfacial trunk in human fetus [8].
Knowledge of the variations of the external carotid artery and its branches is essential for facio-maxillary surgery and surgeries of the neck. The branching pattern of external carotid artery and the knowledge of its origin are essential to avoid complications with catheter insertion of carotid arteries in various procedures [9]. The variations in the origins of external carotid artery can lead to significant possibility of wrong identification during surgery. The detailed insight of the gross and radiologic anatomy of external carotid artery with its branching is essential for applications of angiography in the diagnosis of lesions affecting the neck, face and scalp. The abnormalities most readily diagnosed are tumors, vascular malformations, or bony disorders. Therefore it is necessary to understand the anatomy of this vessel to carry out surgeries in a bloodless field and with minimum postoperative complications [10].
Since there are lots of variations seen in branches of external carotid artery and still many variations are unknown. Hence the present study was done to know the further anatomical variations in course, branching and distribution pattern of external carotid artery and also to correlate the findings with others.
Materials and Methods
After Ethical approval the study was carried out on 30 external carotid arteries. The study was carried out on 15 embalmed Nepalese cadavers irrespective of age and sex in the dissection hall of the Anatomy Department, Manipal College of Medical Sciences from March 2019 to November 2019.
The dissection was done according to the “Cunningham’s manual of practical anatomy 15th edition [11]. A vertical midline incision was taken from the chin to the upper border of sternum. A horizontal incision from lateral side of eye was taken and followed above the tragus and auricle following posteriorly up to mastoid process. Another oblique incision from angle of the mouth to the posterior border of ramus of mandible was made. An oblique incision along the anterior border of the sternocleidomastoid was made from the upper border of sternum to the mastoid process. Skin was reflected carefully so as not to disturb the structures beneath it. The skin was reflected laterally towards the auricles, towards the base of mandible and then at neck region inferolaterally. After reflection of skin, platysma muscle was reflected upwards. All the fat and fascia was removed carefully while the vessels and nerves were kept safe. The sternocleidomastoid was reflected upwards to see the structures below it. The carotid triangle was exposed by clearing the fat over the posterior belly of digastrics and superior belly of omohyoid muscle. The common carotid artery was traced in the carotid sheath till its bifurcation and the external carotid artery was identified anteromedial to the internal carotid artery at the level of upper border of the thyroid cartilage. The external carotid artery was further dissected in the carotid and diagastric triangle. When all the branches & course of the external carotid artery was visible, variations in their origin and course were noted. The length of artery was measured manually with the help of thread, measuring scale and vernier calliper for both right and left sides. The data was analyzed with Microsoft software excel 2007 software and represented as mean ± SD.
Results
During routine dissection an unusual branching pattern of external carotid artery was observed in cadavers. Variations in the origin of branches of external carotid artery on both sides were also observed and noted. Average length of the external carotid artery from its origin by bifurcation of the common carotid artery to its termination is 8.1 cm on the right side and 8.0 cm on the left side. The mean results and standard deviation (SD) of length of various branches of external carotid arteries of both sides is summarized in Table 1.
| Name of branches of external carot- id artery | No of specimen | Right side | Left side | ||
|---|---|---|---|---|---|
| Mean length | SD | Mean length | SD | ||
| Superior Thyroid Artery | 15 | 0.3 | 0.01 | 0.3 | 0.01 |
| Lingual Artery | 15 | 2.0 | 0.05 | 2.1 | 0.06 |
| Facial Artery | 15 | 3.0 | 0.07 | 2.8 | 0.05 |
| Ascending Pharyngeal Artery | 15 | 0.7 | 0.08 | 0.6 | 0.09 |
| Occipital Artery | 15 | 3.2 | 0.09 | 2.7 | 0.05 |
| Posterior Auricular Artery | 15 | 4.8 | 0.08 | 4.6 | 0.1 |
| Superficial Temporal Artery | 15 | 8.1 | 0.05 | 8.0 | 0.06 |
| Maxillary Artery | 15 | 8.1 | 0.05 | 8.0 | 0.06 |
Table 1: Variations in the length of branches of ECA in cm.
A variation in the Level of Carotid Bifurcation
The ECA in majority of cases (21, 70%) took origin at the level of upper border of thyroid cartilage. Higher level origin of upper border of thyroid cartilage was noted in minority of cases (9, 30%). The ECA was antero-medial to the ICA at the level of the carotid bifurcation in all the cases.
Variations in the Branching Pattern of ECA
In present study on the right side we recorded 9 external carotid artery were showing the normal branching pattern i.e. 60% of the cases that includes absence of any kind of trunk or trifurcation present, where as we recorded Thyro- lingual trunk was seen in only one case i.e. 6.6% of the total, Linguo-facial trunk was seen in 3 cases i.e. 20% of the total and Occipito-auricular trunk was seen in 1 cases i.e. 6.6% of the total, trifurcation of the common carotid artery was seen in only 1cases i.e. 6.6% of the total. While on the left side we recorded 7 external carotid were showing normal branching pattern 46.6% of the cases where as we recorded Linguo- facial trunk was present in 4 cases i.e. 26.6% of the total, Occipito-auricular trunk was seen in 2 cases i.e. 13.33% of total and the trifurcation of common carotid artery was seen only in 2 cases i.e. 13.33% of total. The facio-lingual trunk was running medially and upwards, which was crossed by hypoglossal nerve. The thyrolinguofacial and faciomaxillary trunk were not observed in the present study in any of the cases. In comparison of both the sides, the prevalence of variations was more on the left side as compared to right side in the present study. The number and variations of various trunks of both sides is summarized in Table 2.
| Name of the trunk present | No of Right side specimen | Percentage % | No of Left side specimen | Percentage % |
|---|---|---|---|---|
| Thyrolingual trunk | 1 | 6.66 | 0 | 0 |
| Linguofacial trunk | 3 | 20 | 4 | 26.66 |
| Occipitoauricular trunk | 1 | 6.66 | 2 | 13.33 |
| Trifurcation at the origin of external carotid artery | 1 | 6.66 | 2 | 13.33 |
| Normal | 9 | 60 | 7 | 46.6 |
Table 2: Showing the number and percentage of various trunks present in the specimens.

Discussion
Numerous previous studies dealing with the level of carotid bifurcation and variations in the branching pattern of external carotid artery have been described. The level of carotid bifurcation forms an important anatomical and surgical landmark for the pathogenesis of carotid atheromatous and its consequent management by carotid stenting and endarterectomy [12]. The level of the carotid bifurcation has been studied by various authors Lucev, et al. [13], Ito et al. [14], Sanjeev, et al. [15], Al-Rafiah et al. [16].
Their results shows higher levels of carotid bifurcation which correlates with our studies. Our studies shows there was high carotid bifurcation in 30 % cases which was in accordance to Rafiah, et al.[16] and Mompeo and Bajo [17], Studies. Their studies shows high carotid bifurcation was seen in 25% and 36.85% cases respectively. Lower levels of carotid bifurcation as low as intrathoracic bifurcations was reported by Gomez CK [18], Gailloud P, et al. [19] studies however no lower level was seen in our studies. Comparison of the prevalence of branching pattern of external carotid in different populations with present study is shown in Table 3.
| Author | Year | Population | Method | Sample size | Prevalence % |
|---|---|---|---|---|---|
| Lohan et al., [20] | 2007 | American | Angiography | 46 | 82.6 |
| Sanjeev et al., [15] | 2010 | Indian | Dissection | 37 | 56.8 |
| Delic et al., [21] | 2010 | Turkish | Angiography | 91 | 84.6 |
| Yonenaga et al., [22] | 2011 | Japanese | Dissection | 56 | 41.1 |
| Mata et al., [23] | 2012 | Brazil | Dissection | 36 | 77.8 |
| Musa Misiani et al [24] | 2013 | Kenyan | Dissection | 224 | 41.1 |
| Current study | 2019 | Nepalese | Dissection | 30 | 46.7 |
Table 3: Prevalence of branching of external carotid in various populations is compared with present study.
Conclusion
The results of the variations of the external carotid artery and its branches in the present study corroborates with previous studies. In addition we have found some new variations. This knowledge of the variations of the branching pattern of the external carotid artery will be valuable to the head and neck surgeons. The prevalence of variations was seen more on the left side as compared to the right side. The mean length of external carotid artery is more or less difference between right and left side. The detailed insight and awareness of the anatomical variations of the external carotid artery is important and may be useful for vascular surgeons as well as radiologists to prevent diagnostic errors and also to avoid complications while performing surgery in the head and neck region.
References
-
Takenoshita H (1983) Case of hypoplasia of the internal carotid artery associated with persistent primitive hypoglossal artery. Kaibogaku Zasshi 58(5): 533-550.
-
Standring S (2005) Gray’s Anatomy. The Anatomical basis of clinical practice. 39th (Edn.), Edinburg. Elsevier Churchill Livingstone 31: 543-544.
-
Keith LM (2014) Clinically Oriented Anatomy. Lippincott Williams and Wilkins. 7th (Edn.), 1001-1004
-
Dutta AK (1994) Essentials of human anatomy In: Head and Neck. Calcutta: Current Books International 2nd (Edn.), pp: 127-132.
-
Nayak S (1862) Abnormal intra-parotid origin of the facial artery, Saudi Med J, Blanchard & Lea, Philadelphia, pp: 374-376.
-
Midy D, Maures B, Vergnes P, Caliot PA (1986) A Contribution to the study of the facial artery, its branches and anastomoses; application to the anatomic vascular bases of facial fl aps. Surg Radiol Anat 8(2): 99-107.
-
Bergman RA, Thompson SA, Afi fi AK, Saadeh FA (1988) Compendium of human anatomic variations, urban and Schwarzenberg, Baltimore: 65.
-
Zumre O, Salbacak A, Cicekcibasi AE, Tuncer I, Seker M (2005) Investigation of the bifurcation level of the common carotid artery and variations of the branches of the external carotid artery in human fetuses. Ann Anat 187(4): 361-369.
-
Chitra R (2008) Trifurcation of the right common carotid artery. Indian J Plastic Surg 41(1): 85-88.
-
Madhuri AM (2007) Variation in the branching pattern of external carotid artery-a case report. J Anatomical Society India 56(2): 47-51.
-
Romanes GJ (1986) Cunningham’s manual of practical anatomy 15th edn, Oxford medica publication 3: 78-82
-
Michalinos A, Chatzimarkos M, Arkadopoulos N, Safioleas M, Troupis T (2016) Anatomical considerations on surgical anatomy of the carotid bifurcation. Anat Res Int 016: 6907472.
-
Lucev N, Bobinac D, Maric I, Drescik I (2016) Variations of the great arteries in the carotid triangle. Otolaryngol Head Neck Surg 122: 590-591.
-
Ito H, Mataga I, Kageyama I, Kobayashi K (2006) Clinical anatomy in the neck region: the position of external and internal carotid arteries may be reversed. Okajimas Folia Anat Jpn 82(4): 157-167.
-
Sanjeev IK, Anita H, Ashwini M, Mahesh U, Rairam GB (2010) Branching pattern of external carotid artery in human cadavers. J Clin Diagn Res 4(5): 3128-3133.
-
Al-Rafiah A, AA EL-H, Aal IH, Zaki AI (2011) Anatomical study of the carotid bifurcation and origin variations of the ascending pharyngeal and superior thyroid arteries. Folia Morphol (Warsz) 70(1): 47-55.
-
Mompeo B, Bajo E (2015) Carotid bifurcation: clinical relevance. Eur J Anat 19(1): 37-42.
-
Gomez CK, Arnuk OJ (2013) Intrathoracic bifurcation of the right common carotid artery. BMJ Case Rep: bcr2012007554.
-
Gailloud P, Murphy KJ, Rigamonti D (2000) Bilateral thoracic bifurcation of the common carotid artery associated with Klippel-Feil anomaly. AJNR Am J Neuroradiol 21(5): 941-944.
-
Lohan Dg, Barkhordarain F, Saleh R, Krishnam M, Salamon N, et al. (2007) MR Angiography at 3T for Assessment of the External carotid Artery System. Am J Roentegenol: 189(5): 1088-1094.
-
Delic J, Savkovic A, Bajtarevic A, Isakovic E (2010) Variations of ramification of external carotid artery – common trunks of collateral branches. Period Biol 112(1): 117-119.
-
Yonenaga K, Tohnai I, Mitsudo K, Mori Y, Saijo H, et. al. (2011) Anatomical study of the external carotid artery and its branches for administration of superselective intra-arterial chemotherapy via the superficial temporal artery. Int J Clin Oncol 16(6): 654-656.
-
Mata JR, Mata FR, Souza MCR, Nishijo H, Ferreira TAA (2012) Arrangement and prevalence of branches in the external carotid artery in humans. Ital J Anat Embryol 117(2): 65-74.
-
Musa KM, Poonamjeet L, Kevin WO, Jacob G (2015) Variations in branching pattern of external Carotid artery in a black kenyan population. Anatomy J Africa 4(2): 584-590.
- Pattern of Breast Lesions in Ovu Inland, Delta State, South Southern Nigeria
- Morphometric Analysis of the Human Femur: Exploring Platymetric and Robusticity Indices Among the Nigerian Population
- Anatomical Variation of Arteria Lusoria: Clinical Implications for Dysphagia Lusoria and Surgical Risk
- Morphometric Study of the Vertebral Body and Pedicle of Typical Cervical Vertebrae Using Radiological Image
- Epigenetic Mechanisms Driving Human Evolutionary Changes
- Neuroprotective Effects of Ginkgo Biloba Extract on Bilateral Common Carotid Artery Ischaemic Stroke Induced in Wistar Rat