Borderline Resectable Pancreatic Cancer: Concepts and Controversies
Pancreatic cancer is a lethal malignancy which is increasing in incidence. Surgical resection offers the best chances of cure for a potentially resectable adenocarcinoma of pancreas which can be supplemented by appropriate adjuvant treatment further. However, 40% of the cases are diagnosed with a distant metastasis at presentation and the remaining 30- 40% are diagnosed as a locally advanced and unresectable. The definition of resectability has been debatable and the term borderline resectable pancreas was introduced. The optimal approaches to manage these tumors are controversial and not yet standardised. While these tumors may be resectable with high probability of incomplete resection, if they are not downstaged with prior neoadjuvant chemotherapy or chemoradiotherapy. Neoadjuvant chemotherapy with single agent or with multiple agents with or without concurrent radiotherapy have been tried since ages and these modalities have wide range of conversion to R0 resection ranging from 4%- 80%. Majority of the patients despite curative R0 resection require adjuvant chemotherapy either alone or in combination with radiotherapy. This review discusses the controversies related to the management of borderline adenocarcinoma pancreas.
Introduction
Pancreatic cancer is the lethal malignancy and is the fourth leading cause of death in United States. Pancreatic adenocarcinoma is the most aggressive among all known histologies of pancreatic cancer .It has a dismal prognosis too with medial survival ranging from 15- 23 months and 5 – year overall survival (OS) is hardly 15-20% [1, 2]. Historically the localized pancreatic cancer (PC) is treated with surgery followed by adjuvant therapy but this is not true with borderline resectable pancreatic cancer (BRPC) [3]. Nevertheless, currently R0 surgical resection is the mainstay of the treatment and the only modality to offer best chances of long term survival. There is a new entity described in the literature as BRPC, where subgroup of patients respond so well following neoadjuvant therapy that borderline resectable PC becomes amenable to R0 resection. Thus, it becomes crucial to detect the potentially resectable tumor accurately and to offer the appropriate treatment modality to the selected patients and high quality multi-detector computerised tomography (MDCT) is the imaging modality of choice to address this issue. In this review we shall briefly discuss the approach to management of BRPC and we have also tried to resolve existing controversies in the management of BRPC.
Anatomical Definition of BRPC and Resectability Concerns
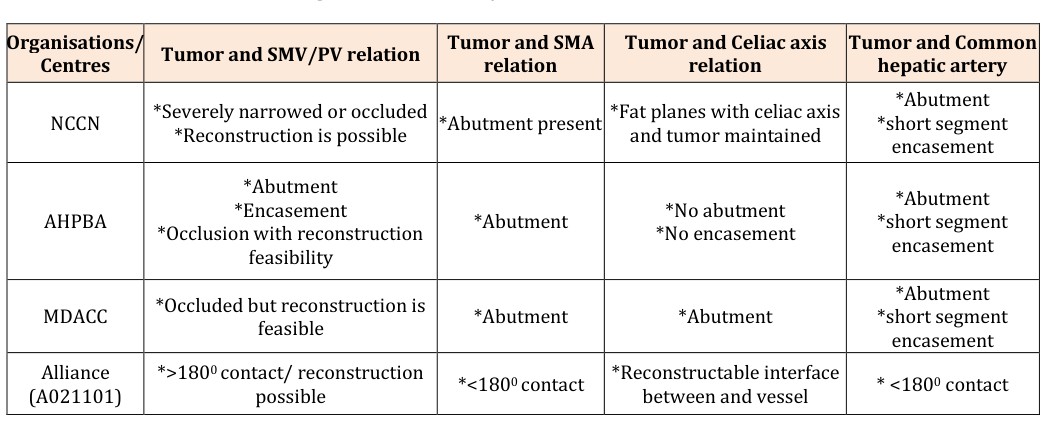
encasement or abuttement of Superior mesenteric artery (SMA)/ portal vein (PV) by either ≥ 180° or ≤ 180° (Table 1). Further in 2014, Tran, et al. simplified this classification by defining Tumor-vein circumference interface (TVI) which is very much helpful in decision making and planning for venous reconstruction. This TVI grouping is as follows; (i) no interface, (ii) ≥ 180° of circumference or occulsion, (iii) ≤ 180° of interface. Details of each system are as follows in table [4, 5, 6, 7]. In brief, BRPC can be defined as tumor limited to pancreas with limited involvement of re-constructible vascular structures whereas locally advanced pancreatic cancer (LAPC) is defined as involvement of celiac axis and /or > 180° encasement of SMA/SMV or PV where reconstruction is not feasible [5]. The multi-institutional trial for patients with BRPC was conducted by Alliance for Clinical Trials in Oncology (Alliance A021101), in cooperation with the Southwest Oncology Group, Eastern Cooperative Oncology Group, and Radiation Therapy Oncology Group, under the support of National Cancer Institute (NCI). The study design employed induction chemotherapy with neoadjuvant chemoradiation per protocol followed by surgery and adjuvant chemotherapy. This trial proposed a new definition of BRPC by radiological criteria according to MDCT findings (Table 1) [8, 9].
- Organisations/
- Centres
- Tumor and SMV/PV relation
- Tumor and SMA
- Tumor and Celiac axis relation relation
- NCCN
- *Severely narrowed or occluded
- *Reconstruction is possible
- *Abutment present *Fat planes with celiac axis and tumor maintained
- *Abutment
- *Encasement
- *Occlusion with reconstruction
- *Abutment
- *No abutment
- *No encasement
- AHPBA feasibility
- MDACC
- *Occluded but reconstruction is feasible
- *Abutment
- *Abutment
- Alliance (A021101)
- *>1800 contact/ reconstruction possible
- *<1800 contact
- *Reconstructable interface between and vessel
- * <1800 contact
Table 1: Various definitions of Anatomic Borderline PC according to the tumor-vessel relationship on MDCT [4-10]
Literature published in the recent past emphasized that the patients with BRPC after R0 resection had survival equivalent to those with primary resectable PC, though the chances of postoperative histopthologically positive margins always remains the main concern [11, 12].
Vascular Involvement: The Decisive Factor in the Management of BRPC
Tumor vessel interface is the most critical step when the treatment for BRPC is planned. A systematic review by Siriwardana, et al. authors have highlighted the oncological outcomes of 1646 patients where PV or SMV had been resected and the reported rates of median postoperative morbidity and mortality were 42% and 5.9% respectively with no improvement in OS [14]. However, Since then, multiple published studies have shown that venous resection and reconstruction in BRPC does not affect postoperative morbidity, mortality and survival [14, 15, 16]. Another meta-analysis reported that there was no difference in perioperative morbidity, mortality or 5-year survival among patients who underwent pancreatic surgery with or without venous resection and vascular reconstruction in BRPC does not comprise OS [17]. On the contrary, two other studies conducted by Castleberry et al. and Worni, et al. found that surgeries involving vascular reconstructions of SMV/PV were associated with increased postoperative morbidity and mortality. However, these researches had used the National Surgical Quality Program database and National Inpatient Sample database respectively which may had involved biases within the data [18, 19] Studies focussing on arterial resection (AR) involving SMA or hepatic artery are very scarce , but proponents of AR do suggest that the oncological outcome is better following AR than offering palliative treatment to these patients [20, 21]. However, other authors propose that morbidity and mortality increases significantly after such reconstruction [22]. A meta-analysis including 366 patients also verifies that, though the AR is associated with increased morbidity and mortality but patients undergoing AR had improved survival compared to those who did not undergo AR [23]. Bockhorn, et al. and Ouaissi, et al. also supported the results. Though, such reconstructions must be accomplished in highly selected patients with good performance status [20, 23].
Margin Status
The definition of R1 resection has not been uniform in the past. European organisation defines the resection as margin positive if, tumor is present ≤ 1mm of the resected margin where as AJCC suggest define positive resection margins when tumor cells are present at the edge of resected specimen. These two slightly different criteria of margin positivity leads to inconsistent reporting of data and hence the results also differ. The oncological outcome after curative resection for BRPC with or without SMV/PV or is highly dependent on histopathological status of margin. The resection is aimed at achieving R0resection as patients with positive margin status perform similar to the patients who did not undergo surgery and survival rates in both the groups is poor [24, 25, 26].
Adjuvant or Neoadjuvant Treatment for BRPC; The Rationale
The intent of neoadjuvant therapy, by definition is to administer treatment prior to curative surgery in patients with potentially resectable disease however, in BRPC the neoadjuvant treatment is also intended to improve R0 resection rates. Various clinical trials have been conducted in the past to justify the implication of NACT or concurrent NACT/RT in BRPC. We tried to summarize the results of the landmark studies conducted so far to address this issue, which is better, chemotherapy or chemo ratio therapy in neoadjuvant setting.
Comparative Studies and Standardisation of Neoadjuvant treatment
Sequencing of Neoadjuvant Treatment; The Rationale
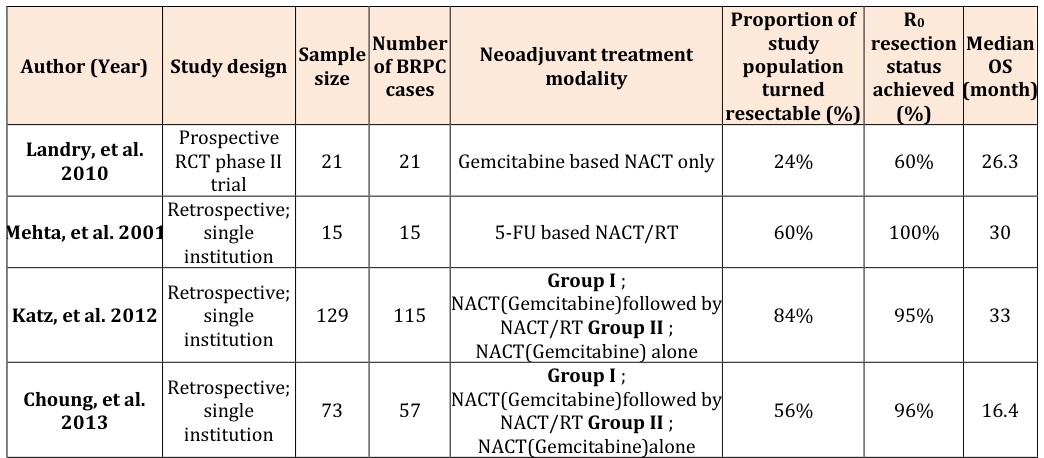
Literature suggests that neoadjuvant therapy offers many advantages over adjuvant therapy and few of those are as follows; (i) It identifies the patient with aggressive tumor biology; (ii) efficacy of radiation therapy is increased; (iii) decreased radiation induced toxicity to adjacent normal tissue; (iv) decreased rate of positive margin status; (v) It increases the rates of resectability of BRPC by downstaging the borderline tumor [27, 28]. Hereby, we tried to discuss the landmark published studies and their end results in table 2, which may guide us to determine which modality is better in neoadjuvant setting i,e; NACT or NACT/RT [9, 29, 30, 31, 32, 33, 34]. Numerous retrospective studies published so far, demonstrate improved median OS by incorporation of concurrent NACT/RT over NACT alone in neoadjuvant setting (Table 2). A retrospective review of 73 patients of pancreatic adenocarcinoma by Choung et al, demonstrates that R0 resection status was achieved in 31 of 32 patients (96.9%) who had BRPC though median OS was comparable (20 months) studies favouring NACT only [31]. However, RCT phase II study by Landry et al demonstrates equivalent median OS of 26.3 months by NACT alone but because of small sample size ( n= 21 patients) this result cannot be extrapolated to the general population of BRPC [9].
- Number
- Author (Year)
- Study design Sample
- Neoadjuvant treatment of BRPC size modality cases
- Prospective
- RCT phase II
- Landry, et al.
- 21
- 21
- Gemcitabine based NACT only
- 24%
- 60%
- 26.3
- 2010 trial
- Retrospective;
- Mehta, et al. 2001 single institution
- 15
- 15
- 5-FU based NACT/RT
- 60%
- 100%
- 30
- Group I ;
- NACT(Gemcitabine)followed by
- Retrospective;
- Katz, et al. 2012 single institution
- 129
- 115
- NACT/RT Group II ;
- NACT(Gemcitabine) alone
- Group I ;
- NACT(Gemcitabine)followed by
- Retrospective;
- Choung, et al. single institution
- 73
- 57
- 2013
- NACT/RT Group II ;
- NACT(Gemcitabine)alone
- Kang, et al. 2012 Retrospective;
- 202
- 35
- NACT/RT (Gemcitabine)
- 91%
- 87%
- 26.3
- Retrospective;
- Stokes, et al. single institution
- 170
- 40
- Cisplatin based NACT/RT
- 46%
- 75%
- 23
- 2011
- Retrospective;
- McClaine, et al. single institution
- 29
- 29
- NACT and NACT/RT both
- 46%
- 67%
- 23.3
Table 2: Studies and their end results in BRPC
In literature, various retrospective studies have reported promising results of adding adjuvant chemotherapy over chemo radiotherapy for BRPC. A recently published GEMCOR LAP 07 phase III study , showed that adjuvant chemo radiation does increase progression free survival ( 6.1 vs. 3.7 months; p = 0.02) however, it fails to show improvement in median overall survival over adjuvant chemotherapy alone arm ( 16.5 vs. 15.3 months, respectively; p= 0.9) [44].
| Study (year) | Patient | Radiotherap | y | Chemotherapy | OS(months) | p value | |||
|---|---|---|---|---|---|---|---|---|---|
| number | (XRT) | ||||||||
| GITSG (1985) vs. Observation | 43 vs. 11 mo | No | 5-Fu ( bolus) | 20 | <0.05 | ||||
| EORTC ( 1999) vs. observation | 114 | No | 5- Fu (infusion) | 17.1 vs. 12.5 mo | <0.05 | ||||
| ESPAC1 (2004) | 541 | Yes | 5-Fu (bolus) | 19.4 mo No effect of XRT | <0.05 | ||||
| RTOG 9704 (2006) | 442 | Yes | Gemcitablinevs. 5-Fu infusion | - | >0.05 | ||||
| CONKO-001 (2007) | 354 | NA | Gemcitabine | 13.4 vs. 6.9 mo | <0.05 | ||||
| ESPAC 3 (2010) | 1088 | NA | Gemcitabine | No difference | >0.05 | ||||
| GERCOR LAP 07 Phase III study ( 2016) Erlotinib | 449 | Yes | Gemcitabline | - | 0.09 |
Table 3: Important Randomised controlled trials for adjuvant treatment for BRPC
Conclusion
Pancreatic adenocarcinoma itself is a detrimental disease with unfavourable outcome in majority of the patients. BRPC poses challenge in management as till date, not any dedicated guidelines have been proposed to manage this entity. Though, vascular resections and reconstructions options have carved a way to treat these tumors surgically, but yet, ambiguity persists in administering adjuvant treatment. Moreover, extensive vascular resection may lead to delayed postoperative recovery which may further delay adjuvant treatment as well. Literature suggests timely incorporation of adjuvant chemotherapy with or without radiation may improve disease free survival as well as median overall survival with high rates of loco regional control. The ongoing randomised control trial may further widen our view to treat this entity more efficiently which may resolve the existing controversies. Acknowledgement: All authors have acknowledged the manuscript. Conflicts of Interest: There are no conflicts of interests among authors.
References
-
Siegel R, Naishadham D, Jemal A (2013) Cancer statistics, CA Cancer J Clin 63(1): 11-30. cancer. Lancet 363(9414): 1049-1057.
-
Yeo CJ, Cameron JL, Lillemoe KD, Sitzmann JV, Hruban RH, et al. (1995) Pancreaticoduodenectomy for cancer of the head of the pancreas. 201 patients. Ann Surg 221(6): 721-731.
-
Tamm EP, Balachandran A, Bhosale PR, Katz MH, Fleming JB, et al. (2012) Imaging of pancreatic adenocarcinoma: update on staging/resectability. Radiol Clin North Am 50(3): 407-428.
-
2008 National comprehensive cancer network practice guidelines in oncology for pancreatic adenocarcinoma-v.1.
-
Callery MP, Chang KJ, Fishman EK, Talamonti MS, William Traverso L, et al. (2009) Pretreatment assessment of resectable and borderline resectable pancreatic cancer: expert consensus statement. Ann Surg Oncol 16(7): 1727-1733.
-
Tran Cao HS, Balachandran A, Wang H, Nogueras- González GM, Bailey CE, et al. (2014) Radiographic tumor-vein interface as a predictor of intraoperative, pathologic, and oncologic outcomes in resectable and borderline resectable pancreatic cancer. J Gastrointest Surg 18(2): 269-278; discussion 278.
-
Katz MH, Marsh R, Herman JM, Shi Q, Collison E, et al. (2013) Borderline resectable pancreatic cancer: need for standardization and methods for optimal clinical trial design. Ann Surg Oncol 20(8): 2787-2795.
-
Landry J, Catalano PJ, Staley C, Harris W, Hoffman J, et al. (2010) Randomized phase II study of gemcitabine plus radiotherapy versus gemcitabine, 5-fluorouracil, and cisplatin followed by radiotherapy and 5- fluorouracil for patients with locally advanced, potentially resectable pancreatic adenocarcinoma. J Surg Oncol 101(7): 587-592.
-
Mahipal A, Frakes J, Hoffe S, Kim R (2015) Mnagement of borderline resectable pancreatic cancer. World J of Gatroenterology 7(10): 241-249.
-
McCracken JD, Ray P, Heilbrun LK, Vaitkevicius VK, Saiki JH, et al. (1980) 5- Fluorouracil, methyl-CCNU, and radiotherapy with or without testolactone for localized adenocarcinoma of the exocrine pancreas: A Southwest Oncology Group Study. Cancer 46(7): 1518-1522.
-
Krzyzanowska MK, Weeks JC, Earle CC (2003) Treatment of locally advanced pancreatic cancer in the real world: Population-based practices and effectiveness. J Clin Oncol 21(18): 3409-3414.
-
Siriwardana HP, Siriwardena AK (2006) Systematic review of outcome of synchronous portal-superior mesenteric vein resection during pancreatectomy for cancer. Br J Surg 93(6): 662-673.
-
Sultana A1, Smith CT, Cunningham D, Starling N, Neoptolemos JP (2007) Meta-analyses of chemotherapy for locally advanced and metastatic pancreatic cancer. J Clin Oncol 25(18): 2607-2615.
-
Adham M, Mirza DF, Chapuis F, Mayer AD, Bramhall SR, et al. (2006) Results of vascular resections during pancreatectomy from two European centres: an analysis of survival and disease-free survival explicative factors. HPB (Oxford) 8(6): 465-473.
-
Illuminati G, Carboni F, Lorusso R, D’Urso A, Ceccanei G, et al. (2008) Results of a pancreatectomy with a limited venous resection for pancreatic cancer. Surg Today 38(6): 517-523.
-
Zhou Y, Zhang Z, Liu Y, Li B, Xu D (2012) Pancreatectomy combined with superior mesenteric vein-portal vein resection for pancreatic cancer: a meta-analysis. World J Surg 36(4): 884-891.
-
Castleberry AW, White RR, De La Fuente SG, Clary BM, Blazer DG, et al. (2012) The impact of vascular resection on early postoperative outcomes after pancreaticoduodenectomy: an analysis of the American College of Surgeons National Surgical Quality Improvement Program database. Ann Surg Oncol 19(13): 4068-4077.
-
Worni M, Castleberry AW, Clary BM, Gloor B, Carvalho E, et al. (2013) Concomitant vascular reconstruction during pancreatectomy for malignant disease: a propensity score-adjusted, populationbased trend analysis involving 10,206 patients. JAMA Surg 148(4): 331-338.
-
Bockhorn M, Burdelski C, Bogoevski D, Sgourakis G, Yekebas EF, et al. (2011) Arterial en bloc resection for pancreatic carcinoma. Br J Surg 98(1): 86-92.
-
Mollberg N, Rahbari NN, Koch M, Hartwig W, Hoeger Y, et al. (2011) Arterial resection during pancreatectomy for pancreatic cancer: a systematic review and metaanalysis. Ann Surg 254(6): 882-893.
-
Amano H, Miura F, Toyota N, Wada K, Katoh K, et al. (2009) Is pancreatectomy with arterial reconstruction a safe and useful procedure for locally advanced pancreatic cancer? J Hepatobiliary Pancreat Surg 16(6): 850-857.
-
Ouaissi M, Hubert C, Verhelst R, Astarci P, Sempoux C, et al. (2010) Vascular reconstruction during pancreatoduodenectomy for ductal adenocarcinoma of the pancreas improves resectability but does not achieve cure. World J Surg 34(11): 2648-2661.
-
Bockhorn M, Uzunoglu FG, Adham M, Imrie C, Milicevic M, et al. (2014) Borderline resectable pancreatic cancer: a consensus statement by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 155(6): 977-988.
-
Neoptolemos JP, Stocken DD, Dunn JA, Almond J, Beger HG, et al. (2001) Influence of resection margins on survival for patients with pancreatic cancer treated by adjuvant chemoradiation and/or chemotherapy in the ESPAC-1 randomized controlled trial. Ann Surg 234(6): 758-768.
-
Winter JM, Cameron JL, Campbell KA, Arnold MA, Chang DC, et al. (2006) 1423 pancreaticoduodenectomies for pancreatic cancer: A single-institution experience. J Gastrointest Surg 10(9): 1199-1210.
-
Fathi A, Christians KK, George B, Ritch PS, Erickson BA, et al. (2015) Neoadjuvant therapy for localized pancreatic cancer: guiding principles. J Gastrointest Oncol 6(4): 418-429.
-
Heestand GM, Murphy JD, Lowy AM (2015) Approach to patients with pancreatic cancer without detectable metastases. J Clin Oncol 33(16): 1770-1778.
-
Mehta VK, Fisher G, Ford JA, Poen JC, Vierra MA, et al. (2001) Preoperative chemoradiation for marginally resectable adenocarcinoma of the pancreas. J Gastrointest Surg 5(1): 27-35.
-
Katz MH, Fleming JB, Bhosale P, Varadhachary G, Lee JE, et al. (2012) Response of borderline resectable pancreatic cancer to neoadjuvant therapy is not reflected by radiographic indicators. Cancer 118(23): 5749-5756.
-
Chuong MD, Springett GM, Freilich JM, Park CK, Weber JM, et al. (2013) Stereotactic body radiation therapy for locally advanced and borderline resectable pancreatic cancer is effective and well tolerated. Int J Radiat Oncol Biol Phys 86(3): 516-522.
-
Kang CM, Chung YE, Park JY, Sung JS, Hwang HK, et al. (2012) Potential contribution of preoperative neoadjuvant concurrent chemoradiation therapy on margin-negative resection in borderline resectable pancreatic cancer. J Gastrointesta Surg 16(3): 509- 517.
-
Stokes JB, Nolan NJ, Stelow EB, Walters DM, Weiss GR, et al. (2011) Preoperative capecitabine and concurrent radiation for borderline resectable pancreatic cancer. Ann Surg Oncol 18(3): 619-627.
-
McClaine RJ, Lowy AM, Sussman JJ, Schmulewitz N, Grisell DL, et al. (2010) Neoadjuvant therapy may lead to successful surgical resection and improved survival in patients with borderline resectable pancreatic cancer. HPB (Oxford) 12(1): 73-79.
-
Assifi MM, Lu X, Eibl G, Reber HA, Li G, et al. (2011) Neoadjuvant therapy in pancreatic adenocarcinoma: a meta-analysis of phase II trials. Surgery 150(3): 466-473. et al. (2016) Effect of Chemoradiotherapy vs Chemotherapy on Survival in Patients With Locally Advanced Pancreatic Cancer Controlled After 4 Months of Gemcitabine With or Without Erlotinib: The LAP07 Randomized Clinical Trial. JAMA 315(17): 1844-1853.
-
Lloyd S, Chang BW, (2013) A comparison of three treatment strategies for locally advanced and borderline resectable pancreatic cancer. J Gastrointest Oncol 4(2): 123-130.
-
Tang K, Lu W, Qin W, Wu Y (2016) Neoadjuvant therapy for patients with borderline resectablepancreatic cancer: A systematic review and meta-analysis of response and resection percentages. Pnacreatology 16(1): 28-37.
-
Kalser MH, Ellenberg SS, (1985) Pancreatic cancer. Adjuvant combined radiation and chemotherapy following curative resection. Arch Surg 120(8): 899- 903.
-
Klinkenbijl JH, Jeekel J, Sahmoud T, Cauvreur C, Veenhof CH, et al. (1999) Adjuvant radiotherapy and 5-fluorouracil after curative resection of cancer of the pancreas and periampullary region: phase III trial of the EORTC gastrointestinal tract cancer cooperative group. Ann Surg 230(6): 776-82.
-
Neoptolemos JP, Stocken DD, Friess H, Claudio B, Dunn JA, et al. (2004) A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. N Engl J Med 350(12): 1200-1210.
-
Regine WF, Winter KW, Abrams R, Safran H, Hoffman JP, et al. (2006) RTOG 9704 a phase III study of adjuvant pre and post chemoradiation (CRT) 5-FU vs. gemcitabine (G) for resected pancreatic adenocarcinoma. J ClinOncol 24: 4007.
-
Oettle H, Post S, Neuhaus P, Gellert K, Langrehr J, et al. (2007) Adjuvant Chemotherapy With Gemcitabine vs Observation in Patients Undergoing Curative-Intent Resection of Pancreatic CancerA Randomized Controlled Trial. JAMA 297(3): 267-277.
-
Neoptolemos JP, Stocken DD, Bassi C, Ghaneh P, Cunningham D (2010) Adjuvant Chemotherapy With Fluorouracil Plus Folinic Acid vs Gemcitabine Following Pancreatic Cancer Resection A Randomized Controlled Trial. JAMA 304(10): 1073-1081.
-
Hammel P, Huguet F, van JL, Goldstein D, Glimelius B,
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma