Combating Immunosuppression within Tumor Microenvironment: A Novel Approach for Drug Design
Recent efforts for cancer treatment include chemotherapy, radiation therapy, surgery, molecular targeted therapy and immunotherapy. Most of these therapies can be beneficial in patients with early stage disease, but this therapy is ineffective to treat advanced stage of metastatic cancer. During cancer initiation and metastasis innate or acquired immune suppression are among the reason for reduced responsiveness to therapy. Majority of the studies of decreased responsiveness focus on marked “immune-suppression†within tumor microenvironment. Several studies have emphasized the impact of therapy-induced physiological changes in cancer cell that can inhibit anti-tumor effect by promoting immunosuppression. These undesired host effects can enhance tumor growth and even malignancy. These effects fall out as a result of systemic release of various regulatory cytokines, chemokines and host immune regulatory cells, which can infiltrate into the tumor. In short, the preferred therapy to target tumor can be offset by reactive effector immune response; by preventing or combating the immunosuppression represents a potentially new approach to boost the effectiveness of systemic and local cancer therapies.
Introduction
Evasion of immune control of tumor growth is a hallmark of cancer. Most of the tumor secreted factors attract and enhance suppressive functions of immune regulatory cells that negatively regulate anti-tumor immunity. The term ‘opposing effect’ is well recognized as an elucidation of the description of the negative consequences of cancer therapy, such as host toxicity. Fundamentally all types and classes of anticancer therapies are accompanying with several adverse effects, Combating Immunosuppression within Tumor Microenvironment: A Novel Approach for Drug Design which can be serious and life-threatening. Such therapy related negative effects not only affect patient health but also effectively reduce the efficacy of therapy. When toxicities become evident, particularly in high grade, therapy might terminate or reduced, causes decreased total intensity of therapy. These alterations in therapy might contribute to the development of immune suppression which leads to reduced responsiveness to treatment and untimely results in tumor progression [1, 2]. Not as much appreciated are the host negative immune response that are associated with reduced anti- J Cancer Oncol
tumor efficacy. Tumors are made up of cancer cell, fibroblasts, vasculature and infiltrating immune cells, together they form tumor microenvironment (TME). The TME is vital for tumor growth, metastasis and escape from host immunity. This paradigm is related to the cancer therapy to induce systemic changes in TME and tumor physiology to promotes immune suppression thereby facilitate tumor invasiveness and/or metastasis.
Thus, cancer therapy represents the metaphorical ‘double-edged sword’, as the inhibit host immune suppressive mechanism and induce desired antitumor immune response. These tumor reactive host immune response actively involved in tumor cell killing by activating cytotoxic CD8 and NK cell response [3, 4, 5]. Tumor growths do not typically revert in the absence of immune therapy; it indicates tumors have escaped immune control. Immune therapy such as immune checkpoint blockade (ICB) stimulates host immune system to control tumor spread by targeting immune suppression within TME. Despite the ICB success, initial response rates with ICB are entirely depend on host pre- existing immune response to tumor and it limited due to tumor associated immune suppression. Methods to decrease suppressive environment and increase immune therapy response are under investigation and include targeting immune suppressive factors in combination with established therapies. In this review, the role of tumor associated immune suppression and how its targeting enhances antitumor immune responses is described. The basics of regulatory responses and its impact on TME will be discussed. Additionally, this review summarizes the preclinical and clinical evidences describing the nature and induction of such host immune regulatory responses mediated by different types of cancer therapies, which either act locally or systematically against tumors. How host immune suppression can reduce tumor response to therapy, and what strategies are available to target immune suppression to improve overall anti-tumor effective immune response are discussed.
Tumor Immuno-Modulation and Progression
The progression of cancer in immune compromised individual demonstrates the deficiencies of cancer immune-surveillance. The immune system does affect tumor development and growth. Transplantation studies showed that tumor growth in immune-competent mice are different. A palpable size of tumor raised in RAG1-/- mice was rejected when grafted in syngeneic host with complete immune system [5, 6]. These observations lead to emerging concept of cancer immune-editing. It proposes evolving tumor are influenced by their environment, including the nature and activation of innate and adaptive immune cells. The most immunogenic tumor cells will be efficiently recognized and eliminated by immune system whereas less immunogenic; due to their low MHC expression and poor antigen presentation will not be detected and express [7, 8]. In this way, the TME somehow shapes the immune system and can subvert the immune response to their benefit. Tumor cells do not only use their advantage the angiogenesis and inflammation reaction but also they actively recruit the suppressors cells to inhibit anti-tumor immunity, such as myeloid-derived suppressor cells (MDSC), regulatory T (Treg) cells and regulatory B (Breg) cells [9, 10, 11]. In human and mice, this population involves a vastly heterogeneous collection of suppressor cells in various stages of tumor growth. Hence, they differ according to tumor with which they are associated, but share the ability to suppress cytotoxic activity.
Depletion of amino acids like arginine, tryptophan or cysteine, which are essential for T cell proliferation and activation and by producing reactive oxygen and nitrogen species MDSCs and Treg cells support tumor development through escape from immune control. As a result, developing tumors use regulatory immune cells to shape their environment in order to prevent effector T cell response and avoid elimination by immune system [12, 13]. Interestingly, tumor cells also able to modulate their non-hematopoietic environment. In mouse melanoma model, secretion of CCL21 chemokine induce the formation of lymph node paracortex-like structures in the tumor stroma, and MDSCs and Treg cells were highly abundant in these structures than in CCL21-/- tumors, which shows reduced tumor growth [14]. It clearly, demonstrates developing tumors subvert innate and adaptive effector cells to promote immunosuppressive activities in order to block cytotoxic activities.
Targeting Immune-Suppression
TME is a Hurdle to Effector Immune Cells
Metastatic tumors escaped the host immunity despite presence of tumor reactive T cells. ICB may recapture immune control of tumor by impeding tumor induced immune suppression. In addition to expression of inhibitory receptors, mechanisms by which the TME can hinders efficacy of effector immune response are listed in Table 1/.. Altered cancer cell growth can lead to tumor intrinsic immune suppressive factors, for instance increased level of lactate and regions of hypoxia can function [2]. Among that, immune checkpoint receptors have gathered the major attention, with proven clinical success.
| Mediator | Mechanism | Reference |
| Cell surface receptors | ||
| PD-1 | Induce T-cell tolerance/anergy | [17,18] |
| CTLA-4 | Inhibit activation of effector T cells, enhance Treg function | |
| Tim-3 | Inhibit Th1 responses and the expression of cytokines such as TNF and INF-γ. | |
| LAG-3 | Negatively regulates cellular proliferation, activation, and homeostasis of T cells, | [19,20] |
| ↓MHC-I | Escape detection by effector CD8 T cells | |
| ↓FAS, TRAIL | Avoid FAS and TRAIL mediated cell killing | [1,8] |
| Secreted cytokines | ||
| TGF-β | Suppress effector cell cytotoxicity and induces Treg cells | |
| IL-10 | Suppress M1 cytokine secretion, induce T cell energy | [21,22] |
| IL-35 | Suppress CD8 T cells and enhance Breg cells | |
| VEGF | Inhibit dendritic cell maturation and induce PD-1 expression | |
| Metabolic pathways | ||
| Hypoxia | Inhibit effector T cell function | |
| IDO, Adenosine | Inhibit T cell proliferation and activation | [15,16] |
| Arginase | Degrades L-arginine needed for cytotoxic T cell function | |
| Lactate | Suppress effector CD8 T cell function | [23,24] |
| Prostaglandin E2 | Recruit MDSCs and suppress M1 macrophages |
Table 1: Mechanism of immune suppression in TME.
Targeting Tumor Cell Derived Immune Suppression
Tumor cells often express immune suppressive antigens on their surface which can inhibit function of effector T cells or induce apoptosis of tumor specific CD8 T cells. One of the best described receptor is PD-1. Binding to its ligand PD-L1 or PD-L2 causes blockade of kinases involved in T cell activation and proliferation [17]. The expression of PD-L1 or PD-L2 on tumor cells negatively correlates with prognosis in malignant melanoma, gastric cancer, ovarian cancer, and renal cell carcinoma highlights the therapeutic potential of this immune checkpoints. Antibodies blocking PD-L1, PD-L2 or PD-1 have shown notable effects in preclinical models [17, 25]. The blocking of PD-L1 signaling enhances the cytolytic activity of tumor specific CD8 T cells and cytokines production from Th cells. The first clinical result from Phase I trial are very promising. Brahmer et al showed prolonged stabilization of disease in patients with advanced cancer treated with PD-L1 antibody BMS- 936559 [26]. As PD-L1 expression in cancer cells seems to predict therapeutic outcome, greater response rate can achieve by selection of PD-L1 positive patients. Targeting PD-L1 by agent MPDL3280A in metastatic bladder cancer, revealed higher response rate [27]. Recently, clinicaltrials.gov lists two ongoing clinical trials with PD- L1 antibody MSB0010718C and MPDL3280A in advanced metastatic cancers. There are several agents under clinical study which targets PD-1. The first published study of nivolumab, a human anti PD-1 antibody, included patients with advanced and heavily spread solid cancers and revealed durable remission in patients responding to the therapy [28]. Few years follow up of several responding patients revealed an ongoing complete remission of tumor growth and re-induction of immune response. Using pidilizumab, another humanized PD-1 antibody, it demonstrated that blocking PD-1 pathway enhance CD8 and NK T cell activity in hematological malignancies. A phase I clinical trial of pidilizumab with multiple myeloma, non-Hodgkin’s lymphoma and acute myeloid leukemia showed a good tolerability [29]. A recently published study assessing pidilizumab in combination with rituximab in B cell lymphoma revealed increased response rate with improved anti-tumor immunity. Moreover, the study showed correlation of pre- existing T cell activation with response to anti-PD-1 treatment [30, 31]. Lambrolizumab another anti-PD-1 antibody was shown to increase response rate of 44% with durable response in advanced melanoma patients. Above represented results of targeting PD-1 signaling represent a key revolution in immunotherapy with durable response in several malignancies. Together with ipilimumab they represent the utmost successful strategy to overcome tumor induced immune suppression and underscore the pronounced therapeutic potential of effective induction of tumor specific immune response [32]. In addition, the expression on Treg; there are studies showing the surface expression of CTLA-4 on human cells in solid and hematological malignancies. An expression of CTLA-4 by cancer cells associated with lymph node metastases in non-small cell lung cancer [33]. Therapeutic strategies targeting CTLA-4 have been demonstrated the efficiency of ICB. Therapies targeting other inhibitory receptors, such as Tim-3, LAG-3, B7-H3 are under development and demonstrate great therapeutic potential [19, 20]. Indoleamine 2,3-dioxygenase (IDO) is another immunosuppressive soluble factor produced by tumor cells and inhibits systemic immune response. IDO catabolize tryptophan and decreases it availability which causes suppression of effector T cells and increased Treg cells in TME. Wang et al demonstrated that depletion of IDO in ovarian cancer leads to slower tumor growth. Systemic injections of INCB024360 (IDO inhibitor) also decreased tumor growth in mice [34]. A tumor antigen attracts immune effector cells and is critical for effective anti-tumor immune response. Reduced antigen presentation as another characteristic of immune escape, which can be main hurdle in overcoming tumor initiated immune suppression. Impaired expression of MHC-I is frequently associated with poor prognosis is many types of cancer. In addition, antigen processing mechanism can be defective, so that tumor cells express MHC-I in normal level, but relevant antigens are not loaded on MHC-I. The antigen processing pathways contains several molecules: TAP1, TAP2, LMP2, LMP7 and chaperones like calretikulin, tapasin and calnexin [35]. Defect in these proteins leads to diminished tumor infiltrating lymphocytes, enhanced tumor growth and advanced rate of metastasis. Recent findings demonstrate that downregulation of MHC-I is mostly regulated by MAPK pathway and MAPK inhibitors elevates MHC-I expression, indicating that alteration in MHC-I might reverse immune suppression and improve response to conventional immunotherapy [36]. Tumor cells often secrets TGF-β and elevated serum level of TGF-β have been demonstrated in ovarian cancer, lung cancer, gastric cancer, breast cancer and others. TGF-β is known to suppress stimulatory cytokines such as IL-2 and IL-12 and is a potent inhibitor of IFN-γ. Moreover, TGF-β affects T cell homing by inhibition of CD8 T cells and stimulation of Treg cell generation. The clinical outcome with GC-1008, a TGF-β- neutralizing antibody, was reported for malignant mesothelioma and demonstrated enhanced mesothelioma specific immune responses [37]. Other factors targeting the TGF-β signaling are under clinical investigation.
Immune Based Therapies to Restrain Tumor Associated Immune-Suppression
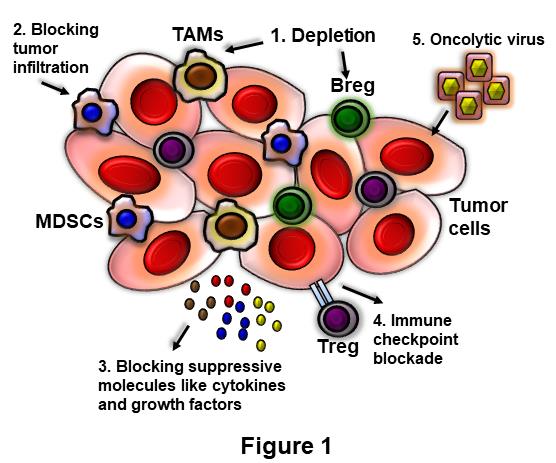
The adaptive immune system can recognize and eliminate malignant cells; in murine model this response limit growth of transplanted and spontaneous tumor and antigen specific T cells detected in human tumors. However, the efficacy of this antitumor action is restricted by TME. Tolerance to tumor antigen me occur due to antigen persistence, downregulation of MHC or presence of Treg and Breg cells [7, 9, 11]. Predominance of Treg in tumor and peripheral blood with expression of PD-L1 in cancer are predictors of poor survival [38]. Nonspecific innate tolerance can also be maintained through secretion of anti-inflammatory and immune suppressive cytokines and downregulation of antigen presentation activity. The TME favors immune suppressive regulators rather than immune effectors. Potential cancer cell intrinsic mechanism of immune elution reduces expression of MHC molecules and increases expression of immune regulatory molecules, such as, FasL and cytokines IL-10, IL-35 and TGF-β. The tumor infiltrating immune cells favorably differentiated towards a regulatory and anti- inflammatory state, because of the expression of immune suppression markers on surface expression like PD-L1 [9]. Furthermore, tumor associate macrophages (TAMs), tumor associated fibroblasts, Treg and secretory factors produced by regulatory cells contribute to tumor induced immune suppression. The accumulation of MDSCs in patients with advanced cancer is related to the extent of disease and disease stage [39]. In addition, increased infiltration of Treg, reduced number of T effector cells and biased towards Th2 response correlates with disease stage [40]. Increase in Treg has been reported in peripheral blood of patients with cancer with associated diminished response to tumor antigens. TAM can drive several pro-tumor processes, including angiogenesis, secretion of tumor growth factors and immune suppression [41, 42]. Tumor infiltrating Treg cells highly expressed cell surface markers OX40 and CTLA-4. Targeting OX-40 and CTLA-4 resulted in systemic anti- tumor immune response capable of eradicating malignant tumor (Figure 1). The effect of this immunotherapy was even detectable at distant, therapy constrained sites like central nervous system (CNS). In clinical trials CTLA-4 or PD-1 antagonists have been promising. Patients do respond to the treatment, even in advanced and malignant stage of cancer [43].
Immunotherapies have potential for the cancer treatment, since immune based treatments act through mechanism that is diverse from radiation or chemotherapy and they characterize non-cross-resistant treatments [14]. T cells and B cells are able to recognize a distinct tumor antigens and can differentiate small antigen difference between normal and transformed cells, providing specificity while reducing toxicity. Numerous studies have sought to characterize different aspects of the immunosuppressive TME and the possible responsible mechanism. There is clinical evidence that activation of an antitumor immune response can result in tumor clearance and provide clinical benefits, however the natural cytotoxic T lymphocyte (CTL) immune response against tumor often falls short of preventing the development of metastasis. Attempt to expand the natural response include using antibodies like PD-1, CTLA-4 blocking antibodies, vaccines like provenge and cytokines like IL-2, IL-12 and IFN- γ [43, 44, 45]. However, the clinical response to these interventions remains low and there is no method to identify whether patient responds to the therapy. Immunotherapy aimed at harnessing host endogenous antitumor immunity by modifying immune suppressive mechanism. In order to release the complete potential and attractive specificity of the antitumor immune response and achieve the better clinical response, the multiple immune regulatory networks co- opted by tumors need to be defined.
Targeting Immunosuppressive Cells and Adoptive Cell Therapy
Depletion of Treg cells is one of the most potent anti- tumor therapies and it has been shown to enhance adoptive immunotherapy in preclinical model. Developing new strategy to precisely target Treg cells in human remains an important research goal. This research is hampered by the fact that both CTLA-4 and CD25 which are expressed of Foxp3+ Treg cells are also expressed on activated effector cells [46]. It has been showed that efficacy of anti-CTLA-4 in melanoma is at least relatively attributable to the specific depletion of Treg cells [47]. Similarly, targeting MDSCs can enhance the efficacy of immunotherapy. Decreased intra-tumoral MDSCs using toxin directed against CCR2 or blockade of their recruitment via the use of CSF-1R inhibitor shown to enhance anti-tumor activity [48, 49]. Blocking suppressive function of MDSCs has been shown to enhance chimeric antigen receptor (CAR) T cell function in xenograft model [50]. Alternative aspect that is gradually recognized is phenotype of T cells being transferred. Preclinical studies indicate that providing effector CD4 T cell help to adoptively transferred CTLs can maximize their antitumor activity in vivo. Parallel transfer of CD4+ and CD8+ CAR T cells was shown to give the highest immune activity against tumor in immunocompetent SCID mice [51]. In addition, a latest trial comparing unselected tumor infiltrating lymphocytes (TILs) and CD8+ enriched TILs found that the patients treated with unselected TILs were more probably to respond. Incorporation of an inducible T cell co-stimulator signaling domain with CAR resulted in greater Th1 differentiation and antitumor effect [52]. In sum, this observation suggests that the presence of CD4 T cells in adoptively transferred T cell population is highly important.
Combat Immunosuppressive Cytokines and Genetic Modification CTL Functions
Immune suppressive cytokines within TME represents a main barrier to function of CTLs. Therefore, genetically modified CTLs to bypass these cytokines signals has the potential to enhance their antitumor efficiency. This is highlighted by the fact that TGF-βRII-/- T cells show greater potency than wild type (WT) control when used in adoptive immunotherapy, showing increased T cell infiltration and cytokine secretion within TME [53, 54]. A more therapeutically appropriate approach is to over- express a receptor that inhibits the effect of TGF-β. The use of adeno virus expressing soluble form of TGF-β receptor was shown to enhance CD8 T cell response. Moreover, expression of dominant negative receptor for TGF-β in tumor specific CD8 T cells and NK cells lead to enhanced antitumor efficacy [53]. While the effect of IL- 17 in the context of antitumor immune response is complex, it is usually considered to be immunosuppressive to the activity of Th1 cells [55]. Therefore, similar approaches are being developed to target IL-17 in the context if immunotherapy.
While targeting regulatory cytokines can boost antitumor immunity, a direct method is to exogenously deliver T cell activated cytokines such as IL-2, IL-12 or IFN-γ which have to show to enhance activity of effector T cells in TME [56] (Figure 1). Another approach is to develop technique to genetically engineer the passively transferred lymphocytes to express IL-2, IL-12 or IFN-γ and locally enhance antitumor immunity. Particular, IL-12 helps to maintain Th1 phenotype which is known to be beneficial for enhancing CD8 T cells, thus making strategies to enhance IL-12 secretion is attractive [57]. On the other hand, modification of intracellular signaling pathways in passively transferred T cells can improve antitumor immunity by avoiding immunosuppressive pathways. For example, Modifying CAR T cells to constitutively express STAT4, which activates by IL-12 signaling, was reported to improve CAR T cells cytotoxic activity against tumor and made them less susceptible to IL-10 and IL-35 mediated suppression [51]. STAT4 is a shared signaling pathway between few regulatory cytokines like IL-35 and IL-27, making this a conceivable path to bypass tumor-induced immunosuppression. Another mechanism by which cancer cells escape the activity of killer CD8 and NK T cells is to induce their apoptosis through FAS-FASL pathway [58]. A potential strategy to avoid this is the use of lncRNA or miRNA to reduce the expression of FAS on T cells and NK cells. It has been also reported over-expression of anti-apoptotic proteins can enhance survival of tumor specific cytotoxic cells [59]. However, these strategies have yet to be assessed in vivo and yet there is few safety concern arising from use of cytotoxic cells that modified with apoptotic molecules.
Combining Radiation with Immune Therapy to Target Immune Suppression in TME
Targeting the immunosuppressive TME might stimulate adaptive immune cell activation and enhance the efficacy of effector cell killing and cytotoxic response. Radiation is a reasonable choice to synergize with immune therapies since it induces intra-tumoral cell death and activates adaptive immune response with enhancing infiltration of CD8 T cells into tumors [60]. Clinical success with ICB has revealed the potential for targeting the TME to boost immune control of tumors. Numbers of active phase 3 clinical trials are assessing combination of radiation and coexisting immune therapies to target immunosuppressive TME [61, 62]. The results from these trials can direct future research on novel targeted immune therapies and conventional immune therapy combination.
Conclusion & Future Perspective
A variety of approaches have been designed and tested in preclinical models to overcome tumor associated immune suppression that need additional testing in clinic and may rise the number of different cancers that can be treated with this therapy. The long term revocation of solid malignancies attained by administration of ICB to overcome tumor mediated immune suppression. While majority of immunotherapeutic approaches like adoptive cell transfer and vaccination focused on an enrichment of tumor specific effector immune response by dictating the immune system towards cancer antigens. Considering limited clinical effects of these therapies, tumor mediated immune suppression have been the main hindrance for these therapies. Consistent with this concept the combination of pre-existing tumor specific immunity and surface expression of inhibitory receptors on cancer cells seem to predict the response to the corresponding ICB. Eventually these therapies may need to combined with other immune checkpoint blockade therapy to increase the infiltration of cytotoxic cells to the tumor site. Recent clinical trial suggests that combining immunotherapies can lead to better antitumor effectiveness without adverse side effects [63]. The multi immunotherapy approach in combination with adoptive cell therapy has substantial potential to overcome tumor associated immune suppression. Checkpoint inhibitors are distinct from conventional chemotherapeutics and have vast potential particularly in combinatorial approaches. Several pre-clinical studies demonstrated synergistic effect of ICB with vaccination, immune-stimulatory factors, radiotherapy or adoptive cell therapy. Recent published results demonstrate that enhanced systemic antitumor immunity in B cell lymphoma after intra- tumoral administration of CTLA-4 and OX-40 I combination with CpG [64, 65]. The synergistic effects of radiation therapy and PD-L1 blockade has been revealed in Kras-mutant lung cancer [66, 67]. These examples underscore great therapeutic potential by combining ICB and immune stimulatory agents with adoptive T cell therapy, CAR and vaccination to combat immunosuppression and direct the immune system against tumor antigens. Tumor mediated immune suppression impede with immune checkpoint blockade; for example, IDO as a resistance mechanism against CTLA- 4 blockade in melanoma model. As there are great differences regarding the immune response to tumor between different patients with same cancer, it might be possible to identify patients to respond for therapies directing to overcome tumor associated immune suppression. Additional clinical studies are needed to understand which immune enhancing strategies are best and essentially where their use is safe. In conclusion, our understanding of the initiation of immune response towards tumor cells is still partial, and further research must be done to develop novel immunotherapeutic strategies.
References
-
Tormoen GW, Crittenden MR, Gough MJ (2018) Role of the immunosuppressive microenvironment in immunotherapy. Adv Radiat Oncol 3(4): 520-526.
-
Marçais A, Walzer T (2018) An immunosuppressive pathway for tumor progression. Nat Med 24(3): 260- 261.
-
Martínez-Lostao L, Anel A, Pardo J (2015) How Do Cytotoxic Lymphocytes Kill Cancer Cells? Clin Cancer Res 21(22): 5047-56.
-
Paul S, Lal G (2017) The Molecular Mechanism of Natural Killer Cells Function and Its Importance in Cancer Immunotherapy. Front Immunol 8: 1124.
-
Kenney LL, Shultz LD, Greiner DL, Brehm MA (2016) Humanized Mouse Models for Transplant Immunology. Am J Transplant 16(2): 389-397.
-
Benichou G, Yamada Y, Yun SH, Lin C, Fray M, et al. (2011) Immune recognition and rejection of allogeneic skin grafts. Immunotherapy 3(6): 757-770.
-
Blankenstein T, Coulie PG, Gilboa E, Jaffee EM (2012) The determinants of tumour immunogenicity. Nat Rev Cancer 12(4): 307-313.
-
Escors D (2014) Tumour immunogenicity, antigen presentation and immunological barriers in cancer immunotherapy. New J Sci, pp: 734515.
-
Lindau D, Gielen P, Kroesen M, Wesseling P, Adema GJ (2013) The immunosuppressive tumour network: myeloid-derived suppressor cells, regulatory T cells and natural killer T cells. Immunology 138(2): 105- 115.
-
Sarvaria A, Madrigal JA, Saudemont A (2017) B cell regulation in cancer and anti-tumor immunity. Cell Mol Immunol 14(8): 662-674.
-
Zhang Y, Gallastegui N, Rosenblatt JD (2015) Regulatory B cells in anti-tumor immunity. Int Immunol 27(10): 521-530.
-
Ohl K, Tenbrock K (2018) Reactive Oxygen Species as Regulators of MDSC-Mediated Immune Suppression. Front Immunol 9: 24-99.
-
Lu T, Gabrilovich DI (2012) Molecular pathways: tumor-infiltrating myeloid cells and reactive oxygen species in regulation of tumor microenvironment. Clin Cancer Res 18(18): 4877-4882.
-
Lin Y, Sharma S, John MS (2014) CCL21 Cancer Immu notherapy. Cancers (Basel) 6(2): 1098-110.
-
Morrot A, da Fonseca LM, Salustiano EJ, Gentile LB, Conde L, et al. (2018) Metabolic Symbiosis and Immunomodulation: How Tumor Cell-Derived Lactate May Disturb Innate and Adaptive Immune Responses. Front Oncol 8: 81.
-
Sugiura A, Rathmell JC (2018) Metabolic Barriers to T Cell Function in Tumors. J Immunol 200(2): 400-407.
-
Wei SC, Duffy CR, Allison JP (2018) Fundamental Mechanisms of Immune Checkpoint Blockade Therapy. Cancer Discov 8(9): 1069-1086.
-
Seidel JA, Otsuka A, Kabashima K (2018) Anti-PD-1 and Anti-CTLA-4 Therapies in Cancer: Mechanisms of Action, Efficacy, and Limitations. Front Oncol 8: 86.
-
He Y1, Cao J, Zhao C, Li X, Zhou C, et al. (2018) TIM-3, a promising target for cancer immunotherapy. Onco Targets Ther 11: 7005-7009.
-
Long L, Zhang X, Chen F, Pan Q, Phiphatwatchara P, et al. (2018) The promising immune checkpoint LAG-3: from tumor microenvironment to cancer immunotherapy. Genes Cancer 9(5-6): 176-189.
-
Mirlekar B, Michaud D, Searcy R, Greene K, Pylayeva- Gupta Y (2018) IL35 Hinders Endogenous Antitumor T-cell Immunity and Responsiveness to Immunotherapy in Pancreatic Cancer. Cancer Immunol Res 6(9): 1014-1024.
-
Landskron G, De la Fuente M, Thuwajit P, Thuwajit C, Hermoso MA (2014) Chronic inflammation and cytokines in the tumor microenvironment. J Immunol Res 2014: 19.
-
Labadie BW, Bao R, Luke JJ (2019) Reimagining IDO Pathway Inhibition in Cancer Immunotherapy via Downstream Focus on the Tryptophan-Kynurenine- Aryl Hydrocarbon Axis. Clin Cancer Res 25(5): 1462- 1471.
-
Uotila P (1993) Inhibition of prostaglandin E2 formation and histamine action in cancer immunotherapy. Cancer Immunol Immunother 37(4): 251-254.
-
Alsaab HO, Sau S, Alzhrani R, Tatiparti K, Bhise K, et al. (2017) PD-1 and PD-L1 Checkpoint Signaling Inhibition for Cancer Immunotherapy: Mechanism, Combinations, and Clinical Outcome. Front Pharmacol 8: 561.
-
Brahmer JR, Tykodi SS, Chow LQ, Hwu WJ, Topalian SL, et al. (2012) Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. N Engl J Med 366(26): 2455-2465.
-
Powles T, Eder JP, Fine GD, Braiteh FS, Loriot Y, et al. (2014) MPDL3280A (anti-PD-L1) treatment leads to clinical activity in metastatic bladder cancer. Nature 515(7528): 558-562.
-
Guo L, Zhang H, Chen B (2017) Nivolumab as Programmed Death-1 (PD-1) Inhibitor for Targeted Immunotherapy in Tumor. J Cancer 8(3): 410-416.
-
Abdin SM, Zaher DM, Arafa EA, Omar HA (2018) Tackling Cancer Resistance by Immunotherapy: Updated Clinical Impact and Safety of PD-1/PD-L1 Inhibitors. Cancers (Basel) 10(2).
-
Westin JR, Chu F, Zhang M, Fayad LE, Kwak LW, et al. (2014) Safety and activity of PD1 blockade by pidilizumab in combination with rituximab in patients with relapsed follicular lymphoma: a single group, open-label, phase 2 trial. Lancet Oncol 15(1): 69-77.
-
Bryan LJ, Gordon LI (2014) Pidilizumab in the treatment of diffuse large B-cell lymphoma. Expert Opin Biol Ther 14(9): 1361-1368.
-
Barbee MS, Ogunniyi A, Horvat TZ, Dang TO (2015) Current status and future directions of the immune checkpoint inhibitors ipilimumab, pembrolizumab and nivolumab in oncology. Ann Pharmacother 49(8): 907-937.
-
Paulsen EE, Kilvaer TK, Rakaee M, Richardsen E, Hald SM, et al. (2017) CTLA-4 expression in the non-small cell lung cancer patient tumor microenvironment: diverging prognostic impact in primary tumors and lymph node metastases. Cancer Immunol Immunother 66(11): 1449-1461.
-
Wang D, Saga Y, Mizukami H, Sato N, Nonaka H, et al. (2012) Indoleamine-2,3-dioxygenase, an immunosuppressive enzyme that inhibits natural killer cell function, as a useful target for ovarian cancer therapy. Int J Oncol 40(4): 929-934.
-
Concha-Benavente F, Srivastava R, Ferrone S, Ferris RL (2016) Immunological and clinical significance of HLA class I antigen processing machinery component defects in malignant cells. Oral Oncol 58: 52-58.
-
Brea EJ, Oh CY, Manchado E, Budhu S, Gejman RS, et al. (2016) Kinase Regulation of Human MHC Class I Molecule Expression on Cancer Cells. Cancer Immunol Res 4(11): 936-947.
-
Stevenson JP, Kindler HL, Papasavvas E, Sun J, Jacobs- Small M, et al. (2013) Immunological effects of the TGFβ-blocking antibody GC1008 in malignant pleural mesothelioma patients. Oncoimmunology 2(8): e26218.
-
Que Y, Xiao W, Guan YX, Liang Y, Yan SM, et al. (2017) PD-L1 Expression Is Associated with FOXP3+ Regulatory T-Cell Infiltration of Soft Tissue Sarcoma and Poor Patient Prognosis. J Cancer 8(11): 2018- 2025.
-
Gonda K, Shibata M, Ohtake T, Matsumoto Y, Tachibana K, et al. (2017) Myeloid-derived suppressor cells are increased and correlated with type 2 immune responses, malnutrition, inflammation and poor prognosis in patients with breast cancer. Oncol Lett 14(2): 1766-1774.
-
Niccolai E, Ricci F, Russo E, Nannini G, Emmi G, et al. (2017) The Different Functional Distribution of "Not Effector" T Cells (Treg/Tnull) in Colorectal Cancer. Front Immunol 8: 1900.
-
Noy R, Pollard JW (2014) Tumor-associated macrophages: from mechanisms to therapy. Immunity 41(1): 49-61.
-
Cassetta L, Kitamura T (2018) Targeting Tumor- Associated Macrophages as a Potential Strategy to Enhance the Response to Immune Checkpoint Inhibitors. Front Cell Dev Biol 6: 38.
-
Rotte A (2019) Combination of CTLA-4 and PD-1 blockers for treatment of cancer. J Exp Clin Cancer Res 38(1): 255.
-
Cheever MA, Higano CS (2011) PROVENGE (Sipuleucel-T) in prostate cancer: the first FDA- approved therapeutic cancer vaccine. Clin Cancer Res 17(11): 3520-3526.
-
Conlon KC, Miljkovic MD, Waldmann TA (2019) Cytokines in the Treatment of Cancer. J Interferon Cytokine Res 39(1): 6-21.
-
Jago CB, Yates J, Câmara NO, Lechler RI, Lombardi G (2004) Differential expression of CTLA-4 among T cell subsets. Clin Exp Immunol 136(3): 463-471.
-
Lipson EJ, Drake CG (2011) Ipilimumab: An anti- CTLA-4 antibody for metastatic melanoma. Clin Cancer Res 17(22): 6958-6962.
-
Lesokhin AM, Hohl TM, Kitano S, Cortez C, Hirschhorn-Cymerman D (2012) Monocytic CCR2(+) myeloid-derived suppressor cells promote immune escape by limiting activated CD8 T-cell infiltration into the tumor microenvironment. Cancer Res 72(4): 876-86.
-
Kumar V, Donthireddy L, Marvel D, Condamine T, Wang F (2017) Cancer-Associated Fibroblasts Neutralize the Anti-tumor Effect of CSF1 Receptor Blockade by Inducing PMN-MDSC Infiltration of Tumors. Cancer Cell 32(5): 654-668.
-
Scarfò I, Maus MV (2017) Current approaches to increase CAR T cell potency in solid tumors: targeting the tumor microenvironment. J Immunother Cancer 5: 28.
-
Avanzi MP, Yeku O, Li X, Wijewarnasuriya DP, van Leeuwen DG (2018) Engineered Tumor-Targeted T Cells Mediate Enhanced Anti-Tumor Efficacy Both Directly and through Activation of the Endogenous Immune System. Cell Rep 23(7): 2130-2141.
-
Dotti G, Gottschalk S, Savoldo B, Brenner MK (2014) Design and development of therapies using chimeric antigen receptor-expressing T cells. Immunol Rev 257(1): 107-126.
-
Yang L, Pang Y, Moses HL (2010) TGF-beta and immune cells: An important regulatory axis in the tumor microenvironment and progression. Trends Immunol 31(6): 220-227.
-
Dahmani A, Delisle JS (2018) TGF-β in T Cell Biology: Implications for Cancer Immunotherapy. Cancers (Basel) 10(6).
-
Murugaiyan G, Saha B (2009) Protumor vs antitumor functions of IL-17. J Immunol 183(7): 4169-4175.
-
Waldmann TA (2018) Cytokines in Cancer Immunotherapy. Cold Spring Harb Perspect Biol 10(12).
-
Díaz-Montero CM, El Naggar S, Al Khami A, El Naggar R, Montero AJ, et al. (2008) Priming of naive CD8+ T cells in the presence of IL-12 selectively enhances the survival of CD8+CD62Lhi cells and results in superior anti-tumor activity in a tolerogenic murine model. Cancer Immunol Immunother 57(4): 563-572.
-
Modiano JF, Bellgrau D (2016) Fas ligand based immunotherapy: A potent and effective neoadjuvant with checkpoint inhibitor properties, or a systemically toxic promoter of tumor growth? Discov Med 21(114): 109-116.
-
Pandey MK, Prasad S, Tyagi AK, Deb L, Huang J, et al. (2016) Targeting Cell Survival Proteins for Cancer Cell Death. Pharmaceuticals (Basel) 9(1).
-
Demaria S, Formenti SC (2012) Role of T lymphocytes in tumor response to radiotherapy. Front Oncol 2: 95.
-
Wang Y, Deng W, Li N, Neri S, Sharma A, et al. (2018) Combining Immunotherapy and Radiotherapy for Cancer Treatment: Current Challenges and Future Directions. Front Pharmacol 9: 185.
-
Asna N, Livoff A, Batash R, Debbi R, Schaffer P, et al. (2018) Radiation therapy and immunotherapy-a potential combination in cancer treatment. Curr Oncol 25(5): e454-e460.
-
Cushman TR, Caetano MS, Welsh JW, Verma V (2018) Overview of ongoing clinical trials investigating combined radiotherapy and immunotherapy. Immunotherapy 10(10): 851-860.
-
Houot R, Levy R (2009) T-cell modulation combined with intratumoral CpG cures lymphoma in a mouse model without the need for chemotherapy. Blood 113(15): 3546-3552.
-
Kvarnhammar AM, Veitonmäki N, Hägerbrand K, Dahlman A, Smith KE, et al. (2019) The CTLA-4 x OX40 bispecific antibody ATOR-1015 induces anti- tumor effects through tumor-directed immune activation. J Immunother Cancer 7(1): 103.
-
Herter-Sprie GS, Koyama S, Korideck H, Hai J, Deng J, et al. (2016) Synergy of radiotherapy and PD-1 blockade in Kras-mutant lung cancer. JCI Insight 1(9): e87415.
-
Gong J, Le TQ, Massarelli E, Hendifar AE, Tuli R (2018) Radiation therapy and PD-1/PD-L1 blockade: the clinical development of an evolving anticancer combination. J Immunother Cancer 6(1): 46.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma