Occupational Radiation Hazards and Competency Assessment
Non-ionizing radiation is the energy traveling through space and is crucial to life, but extreme exposures will cause tissue damage and mutations. The ionizing radiations have sufficient energy due to high frequency and may cause DNA damage. Radiation sources are prevalent in occupational settings, like hospitals, research institutions, nuclear reactors, nuclear weapon production facilities. On earth, sunlight is the most common source of ultraviolet (UV) radiation. Man-made UV sources include UV lamps, arc welding, and mercury vapor lamps. The UV radiation is extensively used in industrial processes and medical and dental practices for a variety of purposes. Excessive exposure to UV radiation is associated with skin cancer, sunburn, accelerated skin aging, and eye disease. The new wireless technology appliances have been used extensively without studying their hazardous effects on society. For instance, the issue of so-called non-thermal effects and potential long-term effects of low-dose exposure were barely examined before the introduction of these technologies. These hazardous sources of radiation can pose a considerable health risk to the workers if not adequately controlled. This review provides a starting point for technical and regulatory information regarding the recognition, evaluation, and control of occupational radiation health hazards.
Introduction
Radioactivity occurs naturally in earth’s crust. It seeps in our food and water through biogeochemical cycles. Even muscles, bones, and tissue of humans contain naturally occurring radioactive elements. Man is exposed to different sources of natural radiation. Radiation from outer space is known as cosmic radiation. X-rays radiation is used as radiation therapy in cancer patients, which cause proteinuria [1]. Other human-made exposures relate to nuclear explosives testing or from coal and nuclear power plants. Sources of radioactive exposure
- Natural radiation of terrestrial origin
- Natural radiation of cosmic origin
- Natural internal radioisotopes
- Medical radiation
- Scientifically improved natural radiation
- Nuclear power
- Work-related exposure This chapter deals with occupational radiation hazard.
Professionals and specialists are exposed to radiation during radiology procedures such as diagnostic, therapeutic, and nuclear medicine procedures. New techniques are continuously introduced in the field of radiology. The 600% increase in medical radiation exposure to the US population since 1980 has provided immense benefit, but potential future cancer risks to patients [2]. Both ionizing radiation and non-ionizing radiation exposure cause almost 10% of invasive cancers [3]. Majority of non-melanoma skin cancers (non-invasive cancers) are caused by non-ionizing UV radiation. On the electromagnetic spectrum, UV radiations are on the boundary between ionizing and non-ionizing radiations.
Non-ionizing radiations such as radiation from mobile phones, electric power transmission, and other similar sources have been defined as a possible carcinogen by the World Health Organization's International Agency for Research on Cancer, but the link remains unproven [4]. The molecular mechanism of cancer due to ionizing radiation is well understood, but quantitative models to predict the level of risk remains debatable. There is a linear relationship between the effective radiation dose and the incidence of cancers. The natural background radiation is the most hazardous source of radiation to general public health, followed by medical imaging [5]. Ionizing radiation (IR) causes double-strand DNA break. Whereas, non-ionizing radiation (NIR) induces oxidative stress and interfere with DNA damage repair mechanism, and both (IR and NIR) lead to cancer.
Furthermore, free-radical generation from a mobile phone, cell phone base stations, broadcast antennas, radar installations, and NIR (ELF-EMF and RFR) increase the risk of cancer [4]. By ICRP recommendations, most regulators permit nuclear energy workers to receive up to 20 times more radiation dose than is allowed for the general public [5]. There is a regulatory limit of exposure annually, and workers are supposed to be kept well within statutory limits. However, globally, a few essential technicians approach their maximum each year due to accidental overexposures. Miscarriage was associated with flight attendant work during sleep hours and high physical job demands and may be related to cosmic radiation exposure [6].
Electromagnetic Frequency Spectrum
The electromagnetic radiations produced due to ionization strips electron from atoms and molecules. Ionization produces little modifications leading biological tissue damage and may affect the DNA [1]. This interaction requires emissions with a high-energy electromagnetic spectrum, including X-rays and gamma rays, which readily ionize organic material. Whereas non- ionizing radiations of radio wave and microwave radiation do not have sufficient energy to ionize atoms and molecules. Other examples of the non-ionizing radiations are visible, infrared, and electromagnetic emissions with relatively low frequencies. In general, the term radiation is applied to ionizing radiation like the one emissions related to nuclear power plants. The portion of the spectrum lying below radiofrequency is known as ELF (extremely low frequency). The electromagnetic (EM) spectrum comprises of the radio frequency in the range of about 3 kilohertz (3 KHz) to 300 gigahertz (300 GHz). The EM spectrum consists of a series of electromagnetic waves from the extremely low frequency and very low frequency (ELF/VLF), through RF and Microwaves, to Infrared (IR) Light, Visible Light, Ultraviolet (UV) light, X- rays, and Gamma rays. Microwaves are a distinct category of radio waves where frequencies range between several hundred MHz to GHz. The extensive use of wireless communication includes AM and FM radio, television broadcast stations, mobile and cellular phones, radar, and microwave systems.
Measurement of Radiation Exposure
The dosimetric units used in radiation protection to limit radiation exposure of nuclear workers and the public include rem and Sievert (SI unit), and their interrelation is depicted below. 1 rem = 10-2 sievert (Sv) 1 millirem (mrem) = 10-5 sievert (Sv) 1 millisievert (mSv) = 10-3 sievert (Sv) 1 millisievert (mSv) = 0.1 rem
Ionizing Radiation
An international study of cancer risk among early nuclear workers from France, UK, and the USA was conducted using a common core protocol, and this study subsequently was expanded to include 15 more countries, and each of these cohorts has been updated recently [7, 8, 9, 10]. Furthermore, as part of the International Nuclear Workers Study (INWORKS), the epidemiological analysis of cancer mortality was carried out from these pooled cohorts. In the world, these cohorts are among the largest, oldest, and most informative groups of nuclear workers. They include men and women who have been monitored for external exposure to radiation using personal dosimeters and have been followed up over decades to collect information on causes of death. Here, we report on analysis of all cancer mortality, and solid cancer mortality. Analyses of death due to lymphatic and hematopoietic cancer (including leukemia) have been reported previously, and analyses of deaths due to non-malignant disease and specific types of solid cancer will be reported subsequently [11].
We aimed to strengthen the scientific basis for the protection of adults from exposures to ionizing radiation with low doses and low dose rates. Even though substantial evidence of low dose radiation effects on cancer after exposure in utero and supportive evidence of such associations following low dose exposures of diagnostic radiation in childhood, epidemiological evidence of low dose radiation effects following exposure in adulthood has been more limited [12, 13, 14].
Types of Radiation
Alpha: Positively charged and consist of two protons and two neutrons. The alpha particles have little penetrating power and may enter the body through ingestion and causes intense local radiation leading to immense damage to the affected tissues. Beta: High-speed electrons with lesser ionizing power and higher penetrating power than alpha particles. There are two routes of entry into body – inhalation, and ingestion. Gamma: Electromagnetic radiations with higher penetrating power than alpha or beta particles. It is produced during nuclear reactions. X-rays: Electromagnetic radiations with energy- dependent penetrating power. X-ray machines are a common source of X-rays; the emissions cease when the computer is switched off. Neutrons: High ionizing and penetrating powers, emitted during nuclear fission. Bremsstrahlung or braking radiation: It is produced by the deceleration of a charged particle, for instance, the slowing down of a beta particle produces these electromagnetic radiations with high penetrating power.
Sources of Ionizing Radiation
Ionizing radiations are deliberately used to different workplaces like healthcare zone, the nuclear industry, academic research centers, and the construction sector. X- rays are used for non-destructive testing in the building enterprise. Also, low levels of ionizing radiation are applied in smoke detectors used in offices and homes. Radon, a radioactive gas, is the best example of naturally occurring ionizing radiations, which occurs near granite outcrops in the vicinity of uranium. Fortunately, we are exposed to environmental radiation at a level that is not considered harmful and is referred to as background radiation, and its primary sources are:
- Sunlight which outsources visible light, ultraviolet light, and infrared light.
- Radioactive materials contained in coal, granite, etc. on the earth’s surface.
- Poisonous gasses like Radon leaking from the ground.
- Cosmic rays coming from outer space to earth through the ionosphere.
• A human body that undergoes natural radioactivity.
X-Rays
X-rays are a form of electromagnetic radiation. Wavelength: 0.01 to 10 nanometers (shorter than UV rays and longer than gamma rays) Frequencies: 3×1016 Hz to 3×1019 Hz Energies: 100 eV to 100 keV X-rays are used to treat various kinds of cancers and the treatment known as radiation therapy. However the dose of radiation used for radiation therapy is higher than the doses used for the imaging such as CT scan. A lower dose of X-ray radiations are used to treat skin cancer whereas, a higher dose of radiation are used to treat cancers within the body such as brain, lung, prostate, and breast [15, 16]. The X-Ray radiation is hazardous for human health and caused podocytopathy in kidney [1].
The researchers in the radiation laboratory are at risk of exposure to X-rays. (Figure 1) The people employed in health facilities including radiation oncologists, radiologists, and other physicians, dentists, pediatricians, and chiropractors whose occupations utilize the use of X- rays and radionuclides. The healthcare staff may be exposed to small doses of radiations or patient who has received treatment with radioactive substances.
These technicians who assist in the production of images, the staff involved in the management of patients, radiological physicists, installers, and fixing of instruments are also at risk of hazardous exposure.

- Mammography and Cancer Therapy
- Bone Density Scans for the detection of osteoporosis.
Diagnostic X-rays (primarily from CT scans due to the large dose used) increase the risk of developmental problems and cancer in those exposed [17]. X-rays are classified as a carcinogen by both the World Health Organization's International Agency for Research on Cancer and the U.S. government [17]. It is estimated that 0.4% of current cancers in the United States are due to computed tomography (CT scans) performed in the past and that had increased up to 1.5-2% by 2007 [18].
Gamma Rays
Gamma rays are lesser ionizing and more penetrating than alpha or beta particles and cause diffuse damage throughout the body. A lower dose of gamma rays caused mutations that cause a stochastic health risk. Higher doses of gamma rays are detrimental to human health and cause acute tissue damage. The efficacy of gamma rays are measured in term s of the physical quantity of the dose absorbed and is measured in grey (Gy).
Body Response
The lower dose of gamma rays causes severe and complex irreparable DNA damage. Whereas DNA damage caused by a higher dose is less severe and more accessible to repair [19]. In radiobiology, radiopharmaceuticals are used for diagnosis some diseases of internal organs such as hyperactive thyroid glands and prostate cancer.
Radiotherapy
Radiotherapy is a branch for the treatment of cancer by using high doses of radiation targeted to kill cancer cells leaving surrounded tissues unharmed (Figure 2).

The doses used in radiotherapy are expected to be a thousand times stronger than those used in diagnostic procedures.
Harmful Effects of Ionizing Radiation
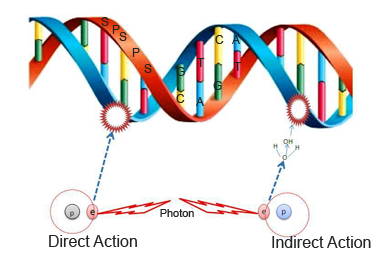
Ionizing radiation ionizes cells in the body and produces free radicals. This cause chemical changes in cell DNA, leading to abnormal cell growth. The ionizing radiation modifies DNA of the body through two mechanisms, direct and indirect action. Indirect action, DNA is ionized, Whereas, radiolytic free radicals produced, indirectly ionizes DNA constituents (Figure 3). This interaction may cause first mutations or strand break, which generate clastogenic damage to DNA, like cutting of double strand (Figure 4). If a single DNA mutation occurs, it is repaired by viable reproduction of the cell or if not repaired causes ‘apoptosis’ or cell death.

Many individuals are exposed to ionizing radiation in the course of their work. The epidemiological study of occupationally irradiated groups such as the Japanese survivors of the atomic bombings of Hiroshima and Nagasaki in 1945 offers a significant opportunity to complement the radiation health hazards [20].
Protection from Ionizing Radiation
The medical use of ionizing radiation is continuously increasing. The European directives Euratom are based on publications of the International Commission on Radiological Protection (ICRP). The goal of ICRP is to assess the hazardous effects of radiation on health care professionals and patients and to draft the new rules and regulations to minimize the impact. These professionals must be trained in RP for patients. However, only a minority of doctors performing radiological examinations inform their patients about any health risk after exposure [21]. Surgical procedures with intraoperative ionizing radiation are on the rise, and it is relevant to implement compliance and ethical rules of RP practices in this environment. As regards the European directives Euratom, professionals exposed to ionizing radiation, such as operating room (OR) doctors, must be trained in RP for workers [22, 23]. Not only training is beneficial for optimizing the use of X-rays machines [23] but promotes awareness of ionizing radiation hazards among staff.
Moreover, analysis of workstation (evaluation of the projected dosimetry of workers which determines functional categorization) and the use of dosimeters (passive and electronic) in areas exposed to ionizing radiation are mandatory and require coordination between occupational Health Department, RP technical advisors, and employers. Otherwise, doctors in OR must have a reinforced medical follow-up. Several surgical specialties such as vascular, urological or neurosurgery are particularly exposed to ionizing radiation [24, 25]. Although the whole-body doses received by OR medical staffs are lower than regulatory dose limit, radiological exposure is likely to be high at hands and eyes lens. Despite radioactive exposure in OR, RP devices are not adequately considered, resulting in lack of the use of protective clothing and dosimeters among staff. Degree of involvement in RP varies per surgical specialty, level of experience, and occupational status.
Indeed, team leaders’ recognition of RP rules is the determinant factor. In addition to occupational practices, studies showed that knowledge in RP is not well known by OR staff and lower than that of the radiologists. Many OR professionals request be trained in RP, and they are aware of radiological hazards, especially radiation- induced cataract. One study showed the interventional cardiologists have a four times higher risk developing a radio-induced cataract than an unexposed population. In this context in 2011, the ICRP issued a recommendation to decrease current annual regulatory limit from 150 mSv to 20 mSv for the eyes lens and integrated into the European Directive 2013/59 Euratom [26]. Access to leaded glasses and installation of collective protective equipment such as ceiling suspended screen significantly reduce lens’ radiology exposure and suspicion of stochastic mechanism for radiation-induced cataract confirm using RP devices to minimize, as much as reasonably possible, received doses according to the As Low As Reasonably Achievable (ALARA) principle.
Bibliographic data on decreasing lens dose, significant radiological exposure in OR, and lack of RP awareness among OR doctors justify evaluating professional practices and knowledge in RP in this population, and relevance of regulatory RP training. To our knowledge, there is no paper conducted with both surgeons and anaesthetists about RP before and after training on this topic. This study evaluates occupational practices and expertise in RP among OR surgeons and anesthetists before and after a training session [27].
Non-Ionizing Radiation
Non-ionizing radiation refers to any electromagnetic radiation that does not carry enough energy per quantum to ionize atoms or molecules.
Health Risk of Non-Ionizing Radiation: Non-ionizing radiation provokes thermal energy in the tissue and cause non-mutagenic effects such as skin burn. More recently, the International Agency for Research on Cancer (IARC) from the World Health Organization (WHO) added radiofrequency electromagnetic fields (including microwave and millimeter waves) to the list of potential carcinogens to human [28]. Based on the possible biological effects, the non-ionizing portion of the spectrum can be subdivided into the following optical radiation portion:
- Portion of the non-ionizing range where electron excitation can occur (visible light, infrared light).
- The part of the non-ionizing spectrum where the wavelength is smaller than the body and heating may occur via induced currents. There are some more undefined hazardous effects such as MW and higher- frequency RF.
- The portion of the non-ionizing spectrum where the wavelength is much more significant than the body. The lower radio frequency, power frequencies, static fields seldom cause heating via induced currents [29].
Types of Non-Ionizing Electromagnetic Radiation
1. Static electromagnetic fields from direct current (0 Hz)
Low-frequency wave of electrical power (50-60 Hz)
2. Extremely Low Frequency (ELF) and Very Low
Frequency (VLF) up to 30 kHz) 3. Radio Frequencies (RF) include 4. Low Frequency (LF), 5. Medium Frequency (MF) 6. High Frequency (HF), 7. Very High Frequency (VHF), 8. Ultra-High Frequency (UHF) 9. Microwave (MW) 10. Infrared (IR) Light, Visible Light and Ultraviolet (UV) light above 300 GHz With the advent of cellular phone technology, antennas radiate non-ionizing radiation of little power. Potential health hazards linked to excessive exposure to high-power densities of non-ionizing radiation include cancer, tumors, headaches, fatigue, Alzheimer’s disease, Parkinson's disease [19, 20]. Other non-ionizing radiations and their effects are discussed in subsequent sections of this chapter.
ELF and VLF-EM Radiation
ELF and VLF range of EMR occur naturally and artificially both. Natural EMR includes those created by thunderstorms, solar and cosmic activity and by the earth. Man-made ELF/VLF occurs due to the generation, transmission, and use of electrical energy. When electricity passes through a conductor electromagnetic field is created. The strength of the electric field depends upon the voltage carried while the magnetic field strength depends on the amount of current carried. Hence, household electrical appliances such as motors in refrigerators, hair dryers, electric blankets, vacuum cleaners, microwaves, televisions, irons, and computers produce electromagnetic field far more significant than levels generated by transmission lines on high towers. The main difference between the two is appliances create electromagnetic fields when in use, whereas in the transmission line electromagnetic fields are continuous. These human-made ELF/VLF electromagnetic fields may cause biological effects, and their effect on health is controversial and still under study [20].
Radio Frequency Radiation
Radio frequency radiation includes LF, MF, HF VHF, UHF, or Microwaves. The biological effects of RF energy are proportional to the rate of energy absorption, and the level of absorption varies little with frequency. RF energy can heat human tissue, and be hazardous if the exposure is intense and continuous. Tissue damage occurs by exposure to high levels of RF energy as the body does not dissipate the excess load of heat generated. Some possible injuries include skin burns, deep burns, heat exhaustion, and heat stroke. Eyes were especially vulnerable to extended exposure to RF energy; lack of blood flow to cool the cornea can result in cataracts.
Broadcast Stations
Radio and TV broadcast stations transmit high levels of RF energy. These antennas radiate several megawatts level of power but, fortunately, placed on tall towers. As a result, they cause little danger to human beings. People absorb RF energy from FM radios; TV broadcast station antennas, mobile telephone, and base station antennas.
Cellular Telephones, Cordless Phones, and Hand-Held Radios
Most cellular and cordless telephones bear a small antenna or the antenna integrated into the body of the phone [21, 22]. Since the antenna of a cell phone is in proximity to the user’s head. As a result, these telephones cause greater danger of RF exposure than any other system. A similar effect is generated by cordless home phones and other two-way hand-held radios.
Base Stations and Radio Sites
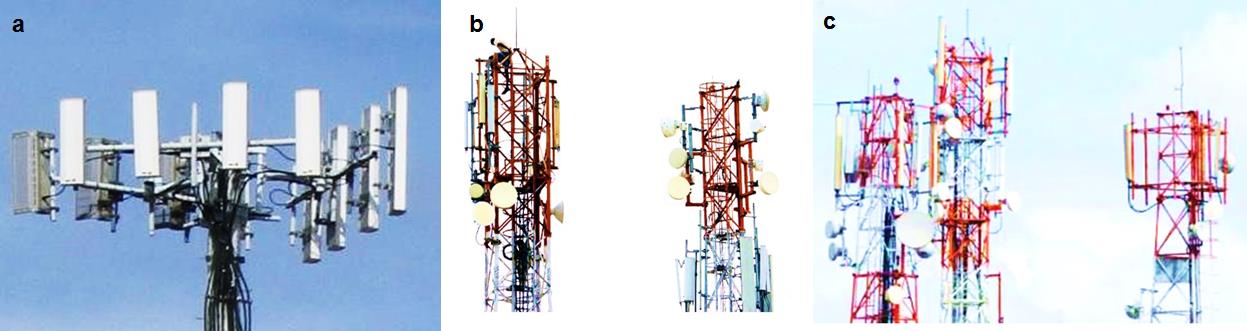
Cellular and other base stations of radio system produce RF energy. Thereby, people working on or in the vicinity of base stations are exposed to this type of energy [23, 24]. However, the effect produced by exposure is minimal because the power generated is less than 100 watts, and the antennas placed on towers that are away from the living zone (Figures 5a-c).
RF Exposure Concerns
The rapid growth of technologies like cellular/cordless and hand-held radios have raised concern over health, particularly brain cancer. These systems possess billions of times the lower energy required to damage DNA in human tissues. The topic of any association between EMR generated by these devices and cancer captured the attention of researchers in the United States and other countries. Many experts believe that EMR with the higher wattage ranges cause cancer risk, whereas base stations at radio sites do not cause any health hazard as far as people are not in proximity to radiation antennas. However, studies are going on issues resulting from cellular phones or mobiles. Hence, a good “precautionary” advice would be to keep cell phone conversations short and avoid its extended use.
A Consequence of Microwave Ovens on Human Health and Food
Unlike ionizing radiation such as X-rays which cause chemical damage to the molecules, nonionizing radiation, like microwaves, do not destroy molecules but generate thermal energy, to evaporate water from wet food or tissue kept in the oven. A particular precaution should be taken while designing microwave ovens so that negligible radiation escapes from the closed door. Many people have the concern that food prepared by microwave ovens is toxic and may cause entirely hypothetical cancer. However, the damaged gasket of the microwave can allow radiation leakage, which might be an unsafe condition.
Microwave Communication Links
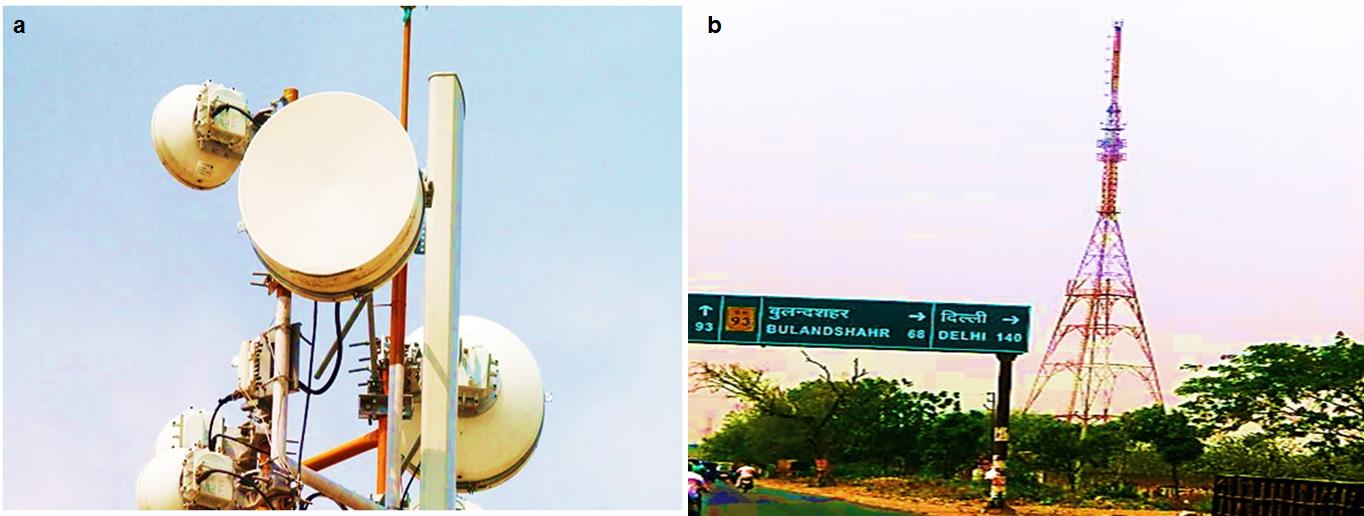
The frequency bands for microwave communication links are in between 1 GHz and 60 GHz. The extensive research on the cellular effects of microwaves radiation on animals has shown reports of lens cataracts and eye damage on exposure to high frequencies of radiation. Microwave communications links make use of highly focused energy beams sent through space between antennas placed at high altitude towers (Figure 6a and b).
Magnetic Resonance Imaging (MRI)
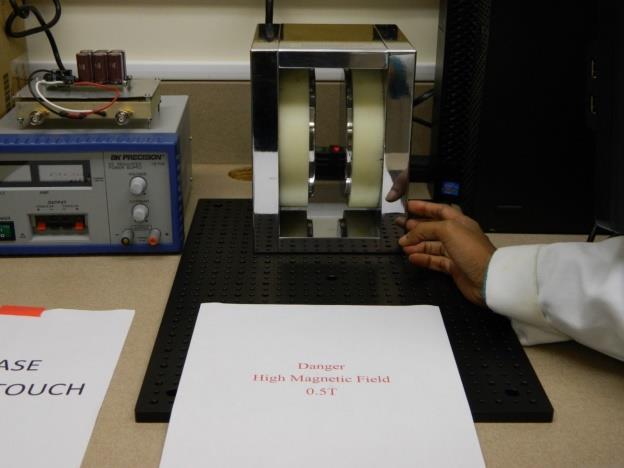
The intrinsic health hazards of MRI procedures should be taken into consideration. Possible health hazards associated with MRI procedures are increasing because of the increasing availability of MR scanners with high static magnetic fields (> 3 T). The term “dosimetry” has begun to be used for non-ionizing techniques such as MRI because of the possible health risks associated with it. Modern techniques are increasingly used in MRI to study the interactions of electromagnetic fields with the human body. These techniques analyze aspects relative to the signal for assuring patient safety and comfort [30]. There are intrinsic hazards of MRI procedure must be understood, acknowledged, and taken into consideration. These hazards are relative to all three types of fields which can affect patients, staff, and other persons within the MR environment [31]. MRI therapy has known to cause adverse damage or injuries. These hazards generated due to interference caused by high magnetic fields from MRIs with implanted electronic devices such as pacemakers (Figure 7).
Near Ultraviolet Radiation
Ultraviolet light can cause cataracts to the eyes and skin burns [11]. UV could be classified into three categories based on the energy:
- Near UV radiation
- Medium UV radiation
- Far UV radiation All UV wavelengths can cause photochemical reactions that may cause DNA damage and carcinogenesis like ionizing radiations.
UV radiation above 10 eV and wavelength shorter than 125 nm, is considered ionizing radiation. Technically, the rest of the UV spectrum is non- ionizing. They can produce photochemical reactions that can cause DNA damage by some mechanism other than pure heat. The ionizing radiation and entire UV spectrum are considered to be equivalent because of their very similar mechanism of damage in many systems including biological system. For example, some non-ionizing range of UV can generate free radicals that may cause oxidative stress and can induce cancer. UV like non-ionizing radiations may also cause pyrimidine dimer formation in DNA and induces melanin production from melanocyte cells to cause sun tanning of the skin. Overexposure of UV to the eyes causes snow blindness, which is a risk, particularly on the sea or when there is snow on the ground. The largest vulnerable group comprise of people spending prolong duration in the sun [27]. Further, the human-made source of UV light that extensively used by the personnel involved in developing photocopy daily. The Xerox- machine has a UV lamp which may prove to be harmful if exposed for long hours (Figure 8).

Infrared Radiation Exposure
The spectrum of solar radiation reaching the Earth ranges from 290 to more than 1,000,000 nm and is divided as follows: 6.8% UV, 38.9% visible, and 54.3% near infrared radiation (NIR) [32]. IR radiation can penetrate the epidermis, dermis, and subcutaneous tissue to differing extents depending on the specific wavelength range being studied. Exposure to IR is perceived as heat [33].
So far, our knowledge of the effects of IR radiation or heat on skin aging is limited. Recent work demonstrates that IR and heat exposure each induces cutaneous angiogenesis, and inflammatory cellular infiltration disrupts the dermal extracellular matrix by inducing matrix metalloproteinases, and alters dermal structural proteins, thereby adding to premature skin aging [32]. Technician working in radiation oncology lab are at risk of IR exposure (Figure 9).

Conclusion
The chapter successfully discussed sources and applications of electromagnetic radiations in everyday life and occupational exposure to unwanted or harmful emissions. With the advent of more advanced technologies, professional and technical personnel in the various fields of research, pathology, medicine, dentistry, and veterinary medicine are exposed to electromagnetic radiation while administering various procedures. Field of radiology would become more advanced with time bringing more people to unwanted unnatural emissions. An effort has been made to control the effect of different types of exposure and efforts that could be used to minimize the effects.
Conflict of Interest
The author confirms that these chapter contents have no conflict of interest.
References
-
Ahmad A, Mitrofanova A, Bielawski J, Yang Y, Marples B, et al. (2017) Sphingomyelinase-like phosphodiesterase 3b mediates radiation-induced damage of renal podocytes. FASEB J 31(2): 771-780.
-
Linet MS, Slovis TL, Miller DL, Kleinerman R, Lee C, et al. (2012) Cancer risks associated with external radiation from diagnostic imaging procedures. CA Cancer J Clin 62(2): 75-100.
-
Anand P, Kunnumakara AB, Sundaram C, Harikumar BK, Tharakan ST, et al. (2008) Cancer is a preventable disease that requires major lifestyle changes. Pharm Res 25(9): 2097-2116.
-
Havas M (2017) When theory and observation collide: Can non-ionizing radiation cause cancer? Environ Pollut 221: 501-550.
-
Ludlow JB, Davies-Ludlow LE, White SC (2008) Patient risk related to common dental radiographic examinations-The impact of 2007 International Commission on Radiological Protection recommendations regarding dose calculation. Journal of the American Dental Association 139(9): 1237- 1243.
-
Grajewski B, Elizabeth Whelan A, Christina Lawson C, Misty Hein J, Martha Waters A, et al. (2015) Miscarriage among flight attendants. Epidemiology 26(2): 192-203.
-
Cardis E, Vrijheid M, Blettner M, Gilbert E, Hakama M, et al. (2005) Risk of cancer after low doses of ionising radiation: retrospective cohort study in 15 countries. BMJ 331(7508): 77.
-
Metz-Flamant C, Laurent O, Samson E, Caër-Lorho S, Acker A, et al. (2013) Mortality associated with chronic external radiation exposure in the French combined cohort of nuclear workers. Occup Environ Med 70(9): 630-638.
-
Muirhead CR, O'Hagan JA, E Haylock RG, Phillipson MA, Willcock T, et al. (2009) Mortality and cancer incidence following occupational radiation exposure: third analysis of the National Registry for Radiation Workers. Br J Cancer 100(1): 206-212.
-
Schubauer-Berigan MK, Daniels RD, Bertke SJ, Tseng CY, Richardson DB, et al. (2015) Cancer Mortality through 2005 among a Pooled Cohort of U.S. Nuclear Workers Exposed to External Ionizing Radiation. Radiat Res 183(6): 620-631.
-
Leuraud K, Richardson DB, Cardis E, Daniels RD, Gillies M, et al. (2015) Ionising radiation and risk of death from leukaemia and lymphoma in radiation- monitored workers (INWORKS): an international cohort study. Lancet Haematol 2(7): 276-281.
-
El Ghissassi F, Baan R, Straif K, Grosse Y, Secretan B, et al. (2009) A review of human carcinogens - Part D: radiation. Lancet Oncology 10(8): 751-752.
-
Pearce MS, Salotti JA, Little MP, McHugh K, Lee C, et al. (2012) Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: a retrospective cohort study. Lancet 380(9840): 499-505.
-
Mathews JD, Forsythe AV, Brady Z, Butler MW, Goergen SK, et al. (2013) Cancer risk in 680,000 people exposed to computed tomography scans in childhood or adolescence: data linkage study of 11 million Australians. BMJ 346: f2360.
-
Hill R, Healy B, Holloway L, Kuncic Z, Thwaites D, et al. (2014) Advances in kilovoltage x-ray beam dosimetry. Phys Med Biol 59(6): R183-R231.
-
Thwaites DI, Tuohy JB (2006) Back to the future: the history and development of the clinical linear accelerator. Phys Med Biol 51(13): R343-R362.
-
Roobottom CA, Mitchell G, Morgan-Hughes G (2010) Radiation-reduction strategies in cardiac computed tomographic angiography. Clin Radiol 65(11): 859- 867.
-
Brenner DJ, Hall EJ (2007) Computed tomography--an increasing source of radiation exposure. N Engl J Med 357(22): 2277-2284.
-
Rothkamm K, Lobrich M (2003) Evidence for a lack of DNA double-strand break repair in human cells exposed to very low x-ray doses. Proc Natl Acad Sci USA 100(9): 5057-5062.
-
Wakeford R (2009) Radiation in the workplace-a review of studies of the risks of occupational exposure to ionising radiation. J Radiol Prot 29(2A): A61-A79.
-
Gervaise A, Esperabe-Vignau F, Pernin M, Naulet P, Portron Y, et al. (2011) Evaluation of the knowledge of physicians prescribing CT examinations on the radiation protection of patients. J Radiol 92(7-8): 681-687.
-
Directives (2013) Council Directive 2013/59/Euratom of 5 December 2013. Official Journal of the European Union, pp: 221.
-
Kuon E, Weitmann K, Hoffmann W, Dörr M, Hummel A, et al. (2015) Role of Experience, Leadership and Individual Protection in the Cath Lab--A Multicenter Questionnaire and Workshop on Radiation Safety. Rofo 187(10): 899-905.
-
Weiss DJ, Pipinos II, Longo GM, Lynch TG, Rutar FJ, et al. (2008) Direct and indirect measurement of patient radiation exposure during endovascular aortic aneurysm repair. Ann Vasc Surg 22(6): 723-729.
-
Soylemez H, Sancaktutar AA, Silay MS, Penbegül N, Bozkurt Y, et al. (2013) Knowledge and attitude of European urology residents about ionizing radiation. Urology 81(1): 30-35.
-
Stewart FA, Akleyev AV, Hauer-Jensen M, Hendry JH, Kleiman NJ, et al. (2012) ICRP publication 118: ICRP statement on tissue reactions and early and late effects of radiation in normal tissues and organs- threshold doses for tissue reactions in a radiation protection context Ann. ICRP 41(1-2): 1-322.
-
Seals KF, Lee EW, Cagnon CH, Al-Hakim RA, Kee ST, et al. (2016) Radiation-Induced Cataractogenesis: A Critical Literature Review for the Interventional Radiologist. Cardiovasc Intervent Radiol 39(2): 151- 160.
-
IARC (2011) IARC Classifies Radiofrequency Electromagnetic Fields As Possibly Carcinogenic To Humans.
-
John E Moulder (2000) Static Electric and Magnetic Fields and Human Health.
-
Hartwig V (2015) Engineering for safety assurance in MRI: analytical, numerical and experimental dosimetry. Magn Reson Imaging 33(5): 681-689.
-
Formica D, Silvestri S (2004) Biological effects of exposure to magnetic resonance imaging: an overview. Biomed Eng Online 3: 11.
-
Cho S, Shin MH, Kim YK, Seo JE, Lee YM, et al. (2009) Effects of infrared radiation and heat on human skin aging in vivo. J Investig Dermatol Symp Proc 14(1): 15-19.
-
Schieke SM, Schroeder P, Krutmann J (2003) Cutaneous effects of infrared radiation: from clinical observations to molecular response mechanisms. Photodermatol Photoimmunol Photomed 19(5): 228- 34.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma