Molecular Profile of Breast Cancer in Women at Pointe Noire (Congo Brazzavile)
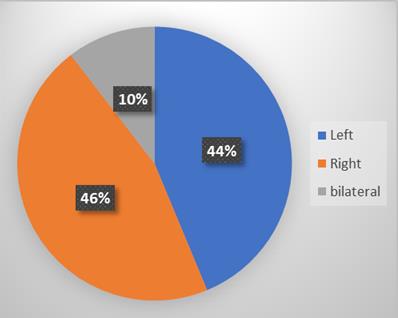
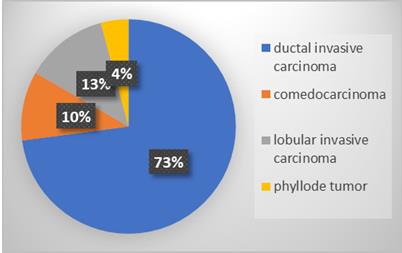
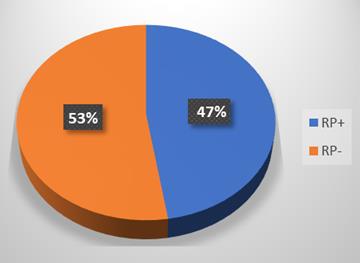
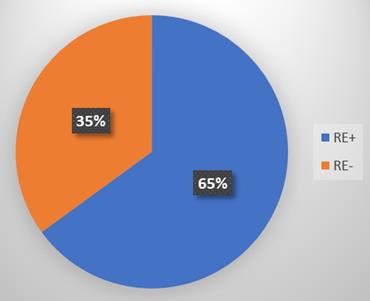
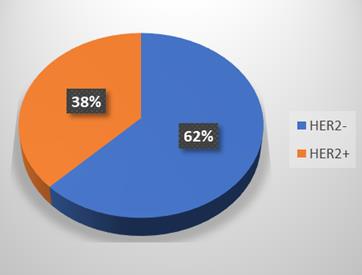
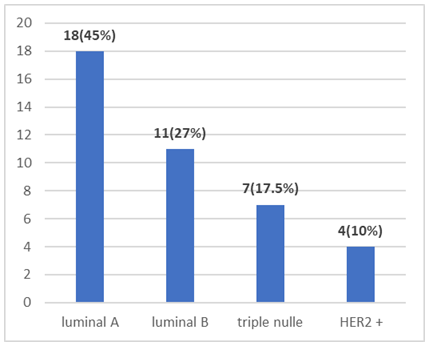
Objective: To determine molecular profile of breast cancer in Pointe Noire. Patients and Methods: We conducted a cross-sectional study covering the period of January 2018 to September 2019, one (1) year and nine (09) months in the General Hospital of Pointe-Noire. 48 records of patients who were diagnosed with breast cancer with or not immunohistochemistry results at Loandjili General hospital. The variables studied were: Age; the family breast cancer history; tumor localization, histological type, estrogen receptors status, progesterone receptors status; HER2 receptors expression, and molecular profile. The comparison of the qualitative variables was made by the chi2 test and the comparison of the quantitative variables was made by the student test (t-test). The p-values were calculated with the data comparison program that uses chi2 tests (Pearson and Fischer) and t-test. Results were statistically significant for P˂0.05. Results: The average age was 45.7 years with extremes of 22 and 79 years. Two women had a history of breast cancer. Breast cancer was more located in right in 46 % of cases. Ductal invasive carcinoma was the most represented histologic type in 73 %. The histopronostic grade II of Scarff bloom Richardson (SBR) was the most represented in 47.5% of cases. 65% of the estrogen receptors were negative. Negative progesterone receptors were the most represented in 53% of cases. Negative expression of the HER2 were the most represented in 62 % of cases. The molecular profile Luminal A were the le most represented molecular profile accounted for 45. In our study, we noted a prevalence of the age group of 40 to 49 years of 25% of which 15% of Luminal A was also observed. There was not relationship between age and molecur profile (P˃ 0.05). A relationship was noted between molecular profile and histological grade (p ˂0.05). Conclusion: Breast cancer is a real public health problem worldwide. It is the first cancer and the leading cause of cancer death in women worldwide. In Pointe Noire the molecular profile is dominated by Luminal A. This study is important and help to the best therapeutic choice of breast cancer.
LM, Moukassa D and Nkoua Mbon JB
Medicine, Loandjili General Hospital and Faculty of Health Sciences Brazzaville,
Congo, Tel: 00242066764164, Email: christianngatali2003@yahoo.fr
Objective: To determine molecular profile of breast cancer in Pointe Noire.
statistically significant for P˂0.05.
help to the best therapeutic choice of breast cancer.
Keywords: Molecular Profile; Breast Cancer; Pointe Noire
Introduction
Breast cancer is a real public health problem worldwide. It is the first cancer and the leading cause of cancer death in women worldwide [1]. According to the World Health Organization (WHO), incidence and mortality rates are generally high in North America, Australia, New Zealand, Western and Northern Europe ; they are intermediate in Central and Eastern Europe, Latin America and the Caribbean ; and low in Africa and Asia [2]. However, in Congo, over 12 years of operation of the cancer registry of the city of Brazzaville, breast cancer accounted for 30.1% of all cancers in 2013 in women [3]. Gombe Mbalawa et al. in 1981 put this cancer at the forefront of female cancers before that of the cervix [4]. The peculiarity of this cancer is that it is a curable cancer at a very early stage [4]. Breast cancer is a major public health problem, so treatment is a major challenge [2]. WHO's anatomo-clinical classification used to optimize treatment is in default in a number of cases, leading to overtreatment or inappropriate treatment [5]. It is therefore necessary to rely on current classifications including both morphological and molecular criteria, which would be more suitable in the therapeutic management [6]. Three predictive biomarkers are used routinely for the therapeutic management of patients with breast cancer ; namely the status of hormone receptors (estrogen receptors and progesterone receptors), the expression of the HER2 gene (Human Epidermal growth factor Receptor 2) and to a certain extent the expression of the Ki67 antigen [7]. Protein fragments are sometimes considered with the presentation of uPA / PAI-1, the only prognostic marker currently validated with a level of evidence [5]. HER2 is a protein whose gene encoding is a proto-oncogene called HER2 / neu. It is a cell proliferation marker with high metastatic potential; thus, tumors overexpressing HER2 are of poor prognosis. Its evaluation involves immunolabeling techniques including paraffin-embedded immunohistochemistry [8]. In countries with limited resources; especially south of the Sahara in general and in the Congo in particular, standard morphological examination remains the only recourse to the diagnosis of certainty and for the prediction of the prognosis. The use of immunohistochemistry techniques in determining the molecular profile of breast cancer has greatly altered therapeutic strategies, which are not commonly used in our context. To our knowledge few studies are curried out about moleculaire in our context in Pointe Noire Our objective was to determine molecular profile of patients with breast cancer in our context of limited resources at Pointe Noire.
Patients and Methods
This was a cross-sectional and descriptive study covering the period from 1 January 2018 to 31 September 2019, one (1) year and nine (09) months which took place at the General Hospital of Loandjili in the Oncology department, Gynecology-Obstetrics department and the Laboratory of Medical and Morphological Analyzes. The general population of our study consisted of all patients with the diagnosis of breast cancer with or not a result of the molecular profile by immunohistochemistry or not. The study sample consisted of forty-eight (48) patients. The variables studied were : Age ; the family breast cancer history ; tumor localization, estrogen receptors status, progesterone receptors status; HER2 receptors expression. The molecular profile was defined by luminal group A: Tumors expressing at least one hormone receptor and not expressing the HER2 receptor. (ER + and / or PR +, HER2-) ; luminal group B : Tumors expressing at least one hormone receptor and expressing the HER2 receptor. (ER+ and / or PR+, HER2 +) ; HER2 + group : HER2 + group tumors are those overexpressing the HER2 receptor without hormone receptor expression. (ER-, PR-, HER2 +); triple negative group : Tumors expressing neither hormone receptor neither HER2 receptor. (ER-, PR-, HER2-). The statistical analysis was done by the following software: Microsoft Excel version 2016 for the preparation of the database and the development of graphs ; the Graph Pad Prism version 5.0.0.3 for data processing. The results were expressed as average for the quantitative variables and in number and / or percentage for the qualitative variables. The comparison of the qualitative variables was made by the chi2 test and the comparison of the quantitative variables was made by the student test (t-test). The p-values were calculated with the data comparison program that uses chi2 tests (Pearson and Fischer) and t-test. Results were statistically significant for P˂0.05.
Results
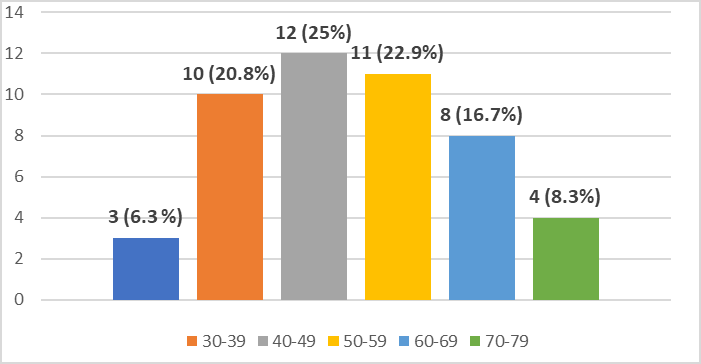
At the end of our study, we obtained 48 breast cancer patients. Out of 48 patients. 8 patients did not benefit from immunohistochemistry for the moelecular study. The average age was 45.7 years with extremes of 22 and 79 years. The median was 48 years. About 25% of the study population was between 40 and 49 years old. Patients over 70 years of age accounted for 8.3% and those between 20 and 29 years of age accounted for 6.3% Figure
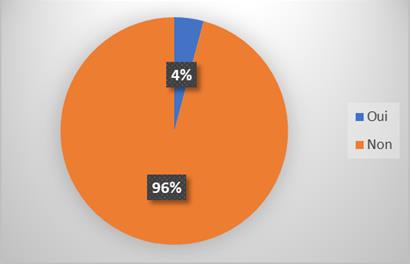
- The majority of the study population (96%) had no family breast cancer history, two (
- patients had a family breast cancer history (mother at age 52, aunt at age 48), Figure
| Molecular profile | |||||||
|---|---|---|---|---|---|---|---|
| Age (years) | Luminal A | Luminal B | HER2+ | Triple nulle | Total | ||
| 20-29 | 1 | 0 | 0 | 2 | 3 | ||
| 30-39 | 4 | 2 | 1 | 0 | 7 | ||
| 40-49 | 6 | 2 | 0 | 2 | 10 | ||
| 50-59 | 4 | 4 | 0 | 1 | 9 | ||
| 60-69 | 2 | 2 | 2 | 1 | 7 | ||
| ≥70 | 1 | 1 | 1 | 1 | 4 | ||
| Total | 18 | 11 | 4 | 7 | 40 |
Table 1: Distribution of patients according to molecular profile and age. P= 0,4509 (DNS).
| Molecular profile | |||||||
|---|---|---|---|---|---|---|---|
| Histological type | Luminal A | Luminal B | HER2+ | Triple nulle | Total | ||
| Ductal invasive carcinoma | 13 | 8 | 4 | 4 | 29 | ||
| Lobular invasive carcinoma | 3 | 2 | 0 | 1 | 6 | ||
| Comedocarcinoma | 2 | 1 | 0 | 2 | 5 | ||
| Phyllode tomor | 0 | 0 | 0 | 0 | 0 | ||
| Total | 18 | 11 | 4 | 7 | 40 |
Table 2: Distribution of patients according to molecular profile and histological type.
| Molecular profile | |||||||
|---|---|---|---|---|---|---|---|
| SBR Grade | Luminal A | Luminal B | HER2+ | Triple nulle | Total | ||
| Grade I | 4 | 4 | 1 | 0 | 9 | ||
| Grade II | 12 | 5 | 0 | 2 | 19 | ||
| Grade III | 2 | 2 | 3 | 5 | 12 | ||
| Total | 18 | 11 | 4 | 7 | 40 |
Table 3: Distribution of patients according to histopronostic grade of Scarff Bloom Richardson and molecular profile P= 0,0154.
Discussion
Although the sample size of our study was small with a sample of 48 patients. We achieved our goal to determine histological and the molecular profile of breast cancer in women at Pointe Noire. Breast cancer is the exclusive preserve of women under 65 according to the WHO [2]. The average age of our patients 45.7 years with extremes of 22 and 79 years. The age group from 40 to 49 years was the most represented 25% (12 cases) in our study, this data were comparable to those reported in the international literature, particularly those observed in Morocco by Affane M, et al. [9] who had a average age of 45 years and those observed by Darré T, et al. [10] in Togo, Fouad A, et al. [11] in Morocco, Ayadi L, et al. [12] in Tunisia who had respectively an average age of 49.7 years, 45 years and 51.5 years. Family history of breast cancer appeared to have no significant association with the occurrence of breast cancer; almost all (96%) of the study population had no family history of breast cancer. In our carcinoma and 22.5% lobular carcinoma inflating. Priti Lal [16] reported percentages of 81.75% for infiltrating ductal carcinomas and 9.76% for invasive lobular carcinomas. Darré T, et al. [10] reported on 450 cases of breast cancer, 73.16% ductal invasive carcinoma followed by 7.3% invasive lobular carcinoma. In our series of 40 cases of breast cancers, the evaluation of the histopronotic grade of Scarff Bloom Richardson (SBR) resulted in grade II in 19 cases (47.5%) followed by grade III in 12 cases (30%). %) and grade I in nine cases (22.5%). Dunnwald [17] in a series evaluating the status of hormone receptors and the prognosis of these different tumors as a function of receptor positivity or negativity reported 49.3% of breast cancers at grade II. Darré T, et al. [10] reported 54.67% Grade II breast cancer, 34.95% Grade III and 10.38% Grade III breast cancer out of 289 cases. Stierer, et al. [18] out of 299 breast carcinomas reported 163 carcinomas at grade II or 54.51%. Our data are similar to those of the literature with a predominance of grade II. In our study, 65% of patients expressed estrogen receptors. This result was similar to that described in the literature, notably Ayadi L [11] and Fouad A [12], which reported respectively 59.4% and 55.5%. This result also seemed to correspond to that obtained in a French study by Vincent A Salomon, et al. [19] who reported 68% of the estrogene receptor. In our 48-case series, 47% of patients expressed progesterone receptor, this result corresponded to that of Ayadi L, et al. [12] who reported in a study on the correlation of HER2 expression and clinical parameters in mammary carcinomas in Tunisia 52.3% of cases. Fouad A. et al. obtained 64.5% of patients expressing RP [11]. In our study, we obtained 38% of HER2 positive patients. Our results corroborate with those of the international literature, particularly those obtained by Ayadi L [11] and Fouad A, [12] who reported 26% and 27.5% respectively. Affane M [9] had found higher ratent at 53%. The molecular profile was obtained from the results of hormone receptors and HER2. Thus, in our series, we obtained 45% of cancers that are Luminal A group, 27.5% Luminal B, 10% HER2 positive and 17.5% of breast cancers Triple negative group. Fouad A, et al. [11] reported a predominance of the Luminal A group, with 54.3% of breast cancers, 16% of B luminal group, 11.3% of HER2 group and 18.3% of Triple negative. Affane M, et al. [9] had 27% of breast cancers that were Luminal A, 21% Luminal B, 31% HER2 positive and 21% breast cancers were Triple negative. In contrast, Aloulou [20] in 2013 in a retrospective study of 130 cases in the determination of the molecular profile of breast cancer reported 30.8% of cancers in the Luminal B group, 6.9% Luminal A, 36% HER2 + and 6,9% Luminal A. In our study, there was no statistically significant difference in the correlation between molecular classification and age (p = 0.4509). However, there has been a predominance of age group from 40 to 49 years of 25% of which 15% luminal A. In our series, there was no statistically significant difference between the molecular profile and the histological type (p = 0.7530). In all molecular groups there was a predominance of infiltrating ductal carcinoma. The HER2 + group consisted exclusively of correlating the molecular profile and the SBR grade, the Luminal A group had the highest histological grade II and the lowest histological grade II, whereas the Triple Negatives had a high histological grade III. The crossover between the molecular profile and the histopronotic grade of Scarff Bloom Richardson in our series noted a statistically significant difference (p = 0.0154). Fouad [11] reported that the Luminal A group had the highest histological grade I (18.8%) and the lowest grade of histologic grade III (24.3%), where as the Triple Negatives had a high rate of histological grade III (52.2%) and a low proportion of grade I (5.3%). This cross was statistically significant (p = 0.036).
Conclusion
Breast cancer is a major public health problem in both developed and resource-poor countries such as Congo, where it accounts for 30.1% of all hospitalizations in 2013 for women. In the city of Pointe-Noire. The molecular profile of breast cancer at Pointe Noire is dominated by luminal A profile. The overall results have a major contribution in the therapeutic management of breast cancer in the Congo and could be used for an adequate therapeutic approach. Moreover further studies are important in order to get more information About Breast Cancer Molecular Profile In Our Context Of Limited Resources.
Conflict of Interest
There were no conflict of interest during this work
References
-
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, et al. (2018) Global cancer statistics: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Cancer J clin 68: 394- 424.
-
Torre LA, Siegel RL, Ward EM, Jemal A (2015) Global cancer statistics 2012. CA Cancer J Clin 65(2): 87-108.
-
Nsondé Malanda J, Nkoua-Mbon JB, Tozoula Bambara A, Ibara G, Minga B, et al. (2013) Douze années de fonctionnement du registre des cancers de Brazzaville. Bull Cancer 100: 135-139.
-
Gombé Mbalawa C (1981) Le cancer au Congo. Afr Méd 20(195): 593-596.
-
Lamy PJ, Romieu G, Rouanet P, Jacot W (2010) Molecular classification of breast cancers: clinical utility. Méd Nucl 34(1): 32-43.
-
Weigelt B, Geyer FC, Reis-Filho JS (2010) Histological types of breast cancer: how special are they? Mol Oncol 4(3): 192-208.
-
Sorlie T, Perou CM, Tibshiramir, Aas T, Geisler S, et al. (2001) Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc Natt Acad Sci USA 98: 10869- 10874.
-
Press MF, Slamon DJ, Flom KJ, Park J, Zhou JY, et al. _(_2002) Evaluation of HER-2/neu gene amplification and overexpression: comparaison of frequently used assay methods in a molecular characterized cohort of breast cancer specimens. J Clin Oncol 20: 3095-3105.
-
Affane M, Aloulou S, Eroui M, Elomrani A, Khouchani M (2014) Epidemiological, Clinical and Molecular Characteristics of Inflammatory Breast Cancer. Research 1: 835.
-
Darré T, Amégbor L, Sonhaye L, Kouyate M, Aboubaraki A, et al. (2013) Profil histo- épidémiologique des cancers du sein à propos de 450 cas observés au CHU de Lomé. Med Afr Noire 60: 53- 58.
-
Fouad A, Yousra A, Kaoutar Z, Omar EM, Afaf A, et al. (2012) Classification moléculaire du cancer du sein au Maroc. Pan Afr Med J 13: 91.
-
Ayadi L, Khabir A, Amouri H, Karray S, Dammak A, et al. (2008) Correlation of HER2 over expression with clinic-pathological parameters in Tunisian breast carcinoma. Word J Surg Oncol 6: 112.
-
Meye JF, Belemboago E, Ngomo K, Nienge S (2003) Le cancer du sein chez la femme à Libreville. Aspects épidémiologiques, diagnostiques et thérapeutiques. Abstracts VIIème congrès des sociétés africaines de gynécologie et d’obstétrique.
-
Traoré LI (2005) Le cancer du sein dans le service de chirurgie à l’hôpital national du Point G: Aspects cliniques et thérapeutiques. Méd Afr Noire 48(9): 135-150.
-
Jovicié-Milentijevié M, Ilié R, Katié V, Zivkovie V (2004) Correlation of steroid hormone recepteur status with histological and nuclear grading in breast carcinoma. J Buon 9(2): 173-177.
-
Priti Lal, Lee K, Tan, Beiyun Chen (2005) Correlation of HER2 status with estrogen and progestérone receptors and histologie features in 3655 breast carcinomas. Am J Clin Patho 123: 541-546.
-
Lisa Dunnwald, Mary A, Christopher I (2007) Hormone receptor status, tumor characteristics and prognostis: a prospective cohort of breast cancer patients. Breast Cancer Res 9(1): 6.
-
Michael Stierer, Harald R, Hanns H, jurgen S, Heinz TL (1993) Company immunohistochemical and biochemical measurement of estrogen and progesterone receptors in primary breast cancer correlation of histopathology and prognostic factors. Annals of surgery 218(1): 13-21.
-
Vincent-Salomon A, Rousseau A, Jouve M, Beuzeboc P, Sigal-Zafrani B, et al. (2004) Proliferation markers predictive of the pathological response and disease outcome of patients with breast carcinomas treated by anthracycline-based preoperative chemotherapy. Eur J Cancer 40(10): 1502-1508.
-
Aloulou S, Belgadi S, Saadi Z, Khouchni M (2013) Profil moléculaire du cancer du sein : étude rétrospective de 130 cas. Cancer Radiol, 24ème Congrès national de la société francaise de radiothérapie oncologique (SFRO) 17(5-6): 613-614.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma