EBRT Modality-Specific Treatment Outcome of Cervical Cancer Patients for Real-World Practice
Purpose: To compare the clinical outcome while treating cervical cancer patients with intensity modulated radiation therapy (IMRT) versus 3-dimensional conformal radiation therapy (3DCRT). Methods: Analyzed a very large dataset from real-world practice using the National Cancer Database (NCDB) for FIGO IB-IIIB inoperable cervical cancer patients treated with chemoradiation from 2004 to 2014. Patients who received initial treatment with external beam radiation therapy (EBRT), either IMRT or 3DCRT, of 40-60Gy dose were included. Patients who received EBRT boost were stratified based on treatment modality (IMRT or 3DCRT for initial and boost). Also considered another group where EBRT is followed by brachytherapy, i.e. the standard of care. IBM-SPSS was used for statistical analysis; p-value
Introduction
Carcinoma of the cervix is one of the common malignancies among women with estimated 13,800 new diagnosis and 4,290 deaths in the United States in 2020. Radiation therapy (RT) plays a critical role in the management of cervical cancer, especially when surgery is not a viable option. Radiation therapy consists of initial external beam radiation (EBRT) with concurrent chemotherapy followed by boost radiation therapy. Pelvic radiation is associated with significant acute and long-term gastro-intestinal side effects affecting the quality of life of these patients. EBRT is commonly delivered using two different techniques: (1) 3-dimensional conformal radiation therapy (3DCRT) and (2) intensity modulated radiation therapy (IMRT). Finer dose modulation and more accurate dose painting are achievable with IMRT, which is an advanced technique, to the target while sparing more critical surrounding normal tissues. Whereas 3DCRT is more conventional technique with limited provision for dose modulation or dose sculpturing.
However, both the techniques are used for treating patients with cervical cancer. Some studies reported no significant difference in overall survival rate (OS), locoregional control rate (LRC) and progression-free survival rate (PFS) when treated with IMRT or 3DCRT [1, 2, 3, 4]. Some studies reported IMRT as a dosimetrically superior technique for cervical cancer treatment resulting in superior clinical outcomes [5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17]. Results from a prospective randomized study demonstrated the superiority of 3DCRT over IMRT for 27 months disease-free survival (79.4% vs. 60%) while treating IIB-IIIB squamous cell carcinoma of the cervix [13]. However, they found lower acute toxicity (grade 2 and grade 3) and higher overall survival when using IMRT (OS 76% vs. 85.7%). It is to be noted that the sample size of this study was small, total 44 patients (22 in 3DCT arm and another half in IMRT arm) and the median follow-up was short with 21.7 months. Good clinical outcome of radiation treatment has been demonstrated in several reports when EBRT is followed by image-guided brachytherapy (IGBT) [18, 19, 20]. Recently the EMBRACE-II study has emphasized the use of IMRT for treating cervical cancer patients [21]. However, there is lack of consensus and large randomized data showing significant benefit of utilizing IMRT over 3D CRT in treatment of cervical cancer. Additionally, studies on real-world scenario are sparse.
In this current study, NCDB (real-world data) from 2004 to 2014 has been analyzed to investigate the relative efficacy of conventional 3DCRT and advanced IMRT techniques for treating cervical cancer. We have also, studied the effectiveness of brachytherapy (BT) boost that is standard of care. The major clinical outcome is the overall survival (OS) of the studied patient population.
Materials and Methods
Data Source and Patient Selection
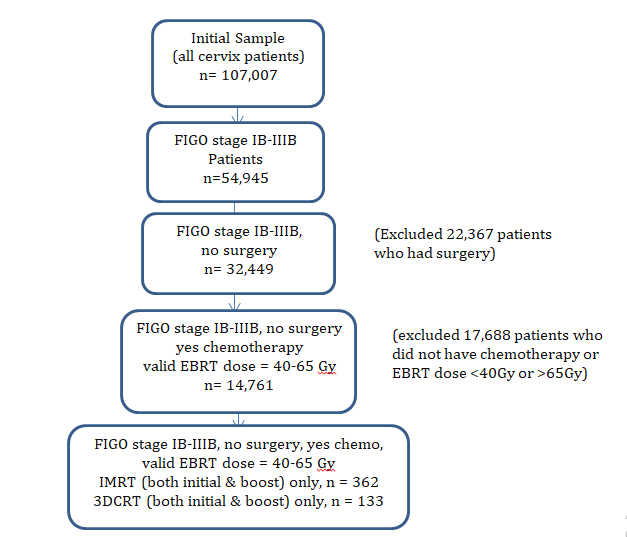
Analyzed the National Cancer Database (NCDB) for locally advanced cervical cancer patients with the International Federation of Gynecology and Obstetrics (FIGO) stage IB- IIIB who were treated between 2004 and 2014. NCDB is a nationwide registry developed and sponsored by the American College of Surgeons and American Cancer Society [22], this dataset captures the real-world practice scenario. Clinical outcome, i.e. overall survival was compared by stratifying the patients in two groups based on the utilization of the treatment techniques. We have considered surgically inoperable patients who received both chemotherapy and EBRT. These patients received primary, i.e. initial treatment with either IMRT (n=362) or 3DCRT (n=133) of 40-65Gy radiation dose. The patients were stratified based on treatment modality; one group received IMRT for both initial and boost while the other group received 3DCRT for initial as well as for boost treatment. Patients who had EBRT boost dose 10-25Gy were included in this study (Figure 1).
Clinical and Demographic Characteristics
The demographic data analyzed and included in this study are (Table 1): age (<40, 40–60, ≥60 years), race (white, black, other), income (median household income in a patient’s zip code), education (percentage of adults in a patient’s zip code that did not graduate high school; <7%, 7–12.9%, 13– 20.9%, ≥21%), residential location (metro, urban, rural) and insurance status (no insurance, private, Medicare, Medicaid, other Govt. and unknown). Comorbidity was measured using the Deyo classification of the Charlson comorbidity score (0, 1, 2). Included patients had FIGO tumor stage IB–IIIB. Patients were identified by using following histology codes: 8070, 8071, 8072, 8140 which corresponded to squamous cell carcinoma not otherwise specified (NOS), keratinizing squamous cell carcinoma NOS, non-keratinizing squamous cell carcinoma, adenocarcinoma NOS, respectively.
Statistical Analysis
IBM SPSS (version 24.0) was used for the data analysis. Any p-value less than or equal to 0.05 was considered statistically significant. Frequency distributions were compared between categorical variables using χ2 tests and trends analyzed using Mantel–Haenszel tests. The overall survival curves for patients receiving different treatment modalities (3DCRT initial and boost vs. IMRT initial and boost) were estimated non-parametrically using the Kaplan- Meier method and the mean survival times were compared with each-other via a two-tailed t-test. The median survival times for the two groups were also compared using a Wilcoxon-Mann-Whitney test. Significant individual predictor of mortality was found by fitting a Cox proportional hazard model for each of the predictor variables considered in this study. Subsequently, a multivariate Cox proportional hazard models involving all predictors was fitted to see if it corroborates the predictor significance results obtained from the individual fits. Similar analyses were carried out for the comparison between patients receiving an EBRT boost after an initial EBRT (IMRT/3DCRT) and those receiving a Brachytherapy boost after an initial EBRT (IMRT/3DCRT). The overall survival curves for all the patients were estimated using the Kaplan-Meier method and compared for each of the three clinical stages of cervical cancer separately, as well as for all three stages combined.
Results
IMRT vs. 3DCRT (Both Initial and Boost)
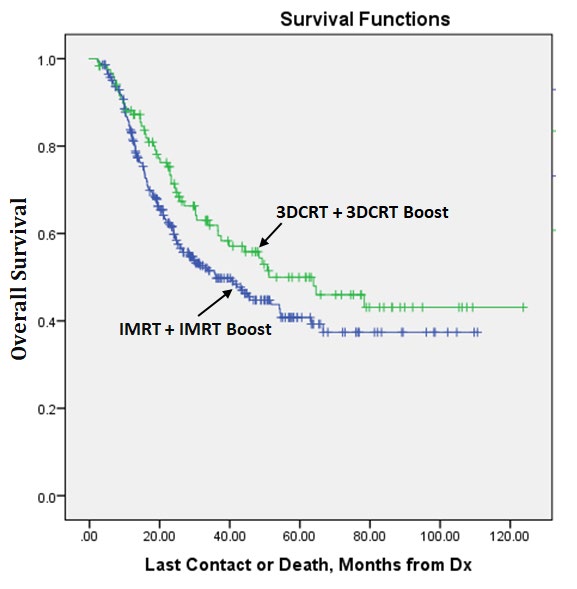
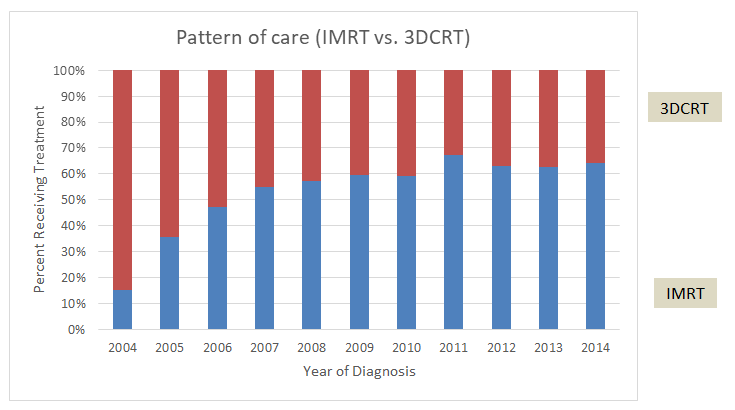
The demographic characteristics of this set of patients (n = 495) are presented in Table 1; majority patient belong to 40-60 years age bracket and living in metro areas. The median age of the patients was 53 years (range: 24–90) and the median follow-up was 24.4 months (range: 2.2–123.7). Effectiveness of these two treatment techniques (IMRT and 3DCRT) in regards to overall survival is presented in the Figure 2 and Table 2 below. Median overall survival was 36.1 months for the patients treated with IMRT while those for 3DCRT was 51.2 months, which was statistically significant (p < 0.05). 2-year and 5-year overall survival were about 9%, and 7% higher for the patients treated with 3DCRT (p < 0.007). However, as shown in Figure 3, the trend of using IMRT technique over the years since 2004 was increasing rapidly till 2007 and then increased relatively slowly. Results from univariate and multivariate analysis are presented in Table 3. Younger patients or patients with higher income seem to have higher overall survival (Table 3; p-value < 0.05).
| All Patients N (%) | IMRT Modality IMRT Boost N (%) | 3DCRT Modality 3DCRT Boost N (%) | P-Value | ||
|---|---|---|---|---|---|
| Overall | 495 | 362 | 133 | ||
| Age | < 40 yr | 45 (13.3) | 45 (12.4) | 21 (15.8) | 0.578 |
| Age | 40 – 60 yr | 248 (50.1) | 185 (51.1) | 63 (47.4) | 0.578 |
| Age | > 60 yr | 181 (36.6) | 132 (36.5) | 49 (36.8) | 0.578 |
| Stage | I (1B-1B2) | 47 (9.5) | 32 (8.8) | 15 (11.3) | 0.222 |
| Stage | II (2-2B) | 149 (30.1) | 103 (28.5) | 46 (34.6) | 0.222 |
| Stage | III (3-3B) | 299 (60.4) | 227 (62.7) | 72 (54.1) | 0.222 |
| Histology | 8070 | 392 (79.2) | 287 (79.3) | 105 (78.9) | 0.164 |
| Histology | 8071 | 32 (6.5) | 28 (7.7) | 4 (3.0) | 0.164 |
| Histology | 8072 | 30 (6.1) | 20 (5.5) | 10 (7.5) | 0.164 |
| Histology | 8140 | 41 (8.2) | 27 (7.5) | 14 (10.5) | 0.164 |
| Comorbidity | 0 | 412 (83.2) | 308 (85.1) | 104 (78.2) | 0.189 |
| Comorbidity | 1 | 65 (13.2) | 42 (11.6) | 23 (17.3) | 0.189 |
| Comorbidity | 2 | 18 (3.6) | 12 (3.3) | 6 (4.5) | 0.189 |
| Race (unknown = 5) | White | 357 (72.1) | 257 (71) | 100 (75.2) | 0.495 |
| Race (unknown = 5) | Black | 95 (19.2) | 71 (19.6) | 24 (18.0) | 0.495 |
| Race (unknown = 5) | Other (all other) | 38 (7.7) | 29 (8.0) | 9 (6.8) | 0.495 |
| High School Education2012 (missing = 5) | 21% or more | 145 (29.3) | 98 (27.5) | 47 (35.3) | 0.217 |
| High School Education2012 (missing = 5) | 13% - 20.9% | 160 (32.3) | 121 (33.9) | 39 (29.3) | 0.217 |
| High School Education2012 (missing = 5) | 7% - 12.9% | 124 (25.1) | 89 (24.9) | 45 (26.3) | 0.217 |
| High School Education2012 (missing = 5) | Less than 7% | 61 (12.3) | 49 (13.7) | 12 (9.0) | 0.217 |
| Income (missing = 5) | Less than $38,000 | 144 (29.1) | 109 (30.5) | 35 (26.3) | 0.547 |
| Income (missing = 5) | $38,000 - $47,999 | 108 (21.8) | 76 (21.3) | 32 (24.1) | 0.547 |
| Income (missing = 5) | $48,000 - $62,999 | 142 (28.7) | 99 (27.7) | 42 (32.3) | 0.547 |
| Income (missing = 5) | $63,000 + | 96 (19.7) | 73 (20.4) | 23 (17.3) | 0.547 |
| Residence Location (missing = 4) | Metro counties | 408 (82.4) | 297 (83.0) | 111 (83.5) | 0.756 |
| Residence Location (missing = 4) | Urban counties | 75 (15.2) | 56 (15.6) | 19 (14.3) | 0.756 |
| Residence Location (missing = 4) | Rural counties | 8 (1.6) | 5 (1.4) | 3 (2.3) | 0.756 |
| Insurance | No Insurance | 79 (16.0) | 59 (16.3) | 20 (15.0) | 0.157 |
| Insurance | Private Insurance | 153 (30.9) | 105 (29.0) | 48 (36.1) | 0.157 |
| Insurance | Medicare | 115 (23.2) | 95 (26.2) | 20 (15.0) | 0.157 |
| Insurance | Medicaid | 132 (26.7) | 92 (25.4) | 40 (30.1) | 0.157 |
| Insurance | Other Govt. | 4 (0.8) | 3 (0.8) | 1 (0.8) | 0.157 |
| Insurance | Unknown | 12 (2.4) | 8 (2.2) | 4 (3.0) | 0.157 |
Table 1: Clinical and demographic characteristics of the cohort stratified by type of EBRT (IMRT vs. 3DCRT) utilized.
| IMRT With IMRT Boost | 3DCRT With 3DCRT Boost | P-Value | |
|---|---|---|---|
| No. of patients | 362 | 133 | 0.001 |
| 2-year OS (%) | 64.0 | 73.3 | 0.005 |
| 5-year OS (%) | 52.4 | 58.3 | 0.004 |
| Median OS (months) | 36.1 | 51.2 | 0.044 |
Table 2: Overall survival (OS) of the patients treated with IMRT and 3DCRT.
| Factor | N (%) | Univariate Analysis | Cox-proportional Hazard | ||
|---|---|---|---|---|---|
| Unadjusted HR | p-Value | Adjusted HR | p-Value | ||
| Age (years) | |||||
| Age < 40 | 248 (50.1) | Ref | Ref | Ref | Ref. |
| 40 ≤ age ≤ 60 | 181 (36.6) | 1.43 (0.87 – 2.37) | 0.160 | 1.50 (0.86 – 2.60) | 0.146 |
| age > 60 | 66 (13.3) | 1.60 (0.96 – 2.67) | 0.073 | 1.46 (0.78 – 2.74) | 0.242 |
| Stage | |||||
| One | 149 (30.1) | Ref | Ref | Ref | Ref |
| Two | 299 (60.4) | 0.99 (0.56 – 1.72) | 0.961 | 1.00 (0.56 – 1.78) | 0.997 |
| Three | 47 (9.5) | 1.31 (0.78 – 2.20) | 0.315 | 1.30 (0.75 – 2.25) | 0.349 |
| Histology | |||||
| 8071 | 32 (6.5) | Ref | Ref | Ref | Ref |
| 8072 | 30 (6.1) | 1.17 (0.69 – 1.99) | 0.558 | 1.17 (0.66 – 2.05) | 0.592 |
| 8140 | 41 (8.2) | 0.71 (0.36 – 1.39) | 0.314 | 0.84 (0.42 – 1.71) | 0.639 |
| 8070 | 392 (79.2) | 0.62 (0.35 – 1.11) | 0.110 | 0.68 (0.36 – 1.28) | 0.228 |
| Comorbidity | |||||
| 0 | 65 (13.2) | Ref | Ref | Ref | Ref |
| 1 | 18 (3.6) | 1.57 (1.07 – 2.31) | 0.020 | 1.59 (1.05 – 2.40) | 0.028 |
| 2 or more | 412 (83.2) | 1.95 (1.03 – 3.70) | 0.041 | 2.04 (1.01 – 4.10) | 0.046 |
| Race | |||||
| Black | 95 (19.2) | Ref | Ref | Ref | Ref |
| Others | 43 (7.7) | 0.89 (0.62 – 1.27) | 0.520 | 0.93 (0.62 – 1.38) | 0.709 |
| White | 357 (72.1) | 0.82 (0.46 – 1.45) | 0.491 | 1.00 (0.55 – 1.83) | 0.990 |
| Education High School | |||||
| Less than 7% | 61 (12.3) | Ref | Ref | Ref | Ref |
| 7% - 12.9% | 124 (25.1) | 1.74 (1.01 – 2.76) | 0.018 | 1.80 (1.03 – 3.14) | 0.040 |
| 13% - 20.9% | 160 (32.3) | 1.51 (1.03 – 2.20) | 0.035 | 1.31 (0.81 – 2.12) | 0.276 |
| 21% or more | 145 (29.3) | 1.19 (0.82 – 1.74) | 0.358 | 1.07 (0.71 – 1.62) | 0.745 |
| Income | |||||
| Less than $38,000 | 144 (29.1) | Ref | Ref | Ref | Ref |
| $38,000 - $47,999 | 108 (21.8) | 0.64 (0.42 – 0.97) | 0.033 | 0.84 (0.48 – 1.46) | 0.541 |
| $48,000 - $62,999 | 142 (28.7) | 0.87 (0.57 – 1.33) | 0.519 | 1.17 (0.69 – 1.98) | 0.559 |
| $63,000 + | 96 (19.7) | 0.61 (0.40 – 0.92) | 0.019 | 0.67 (0.43 – 1.04) | 0.076 |
| Location | |||||
| Urban counties | 75 (15.2) | Ref | Ref | Ref | Ref |
| Rural counties | 8 (1.6) | 1.05 (0.71 – 1.55) | 0.806 | 0.94 (0.61 – 1.44) | 0.760 |
| Metro counties | 408 (83.1) | 1.10 (0.35 – 3.44) | 0.871 | 0.73 (0.22 – 2.42) | 0.609 |
| Insurance | |||||
| Pvt. Ins. / Mng Care Medicaid | 153 (30.9) 115 (23.2) | Ref 1.00 (0.63 – 1.60) | Ref 0.991 | Ref 0.92 (0.56 – 1.49) | Ref 0.727 |
| Medicare | 132 (26.7) | 1.36 (0.85 – 2.18) | 0.204 | 1.27 (0.78 – 2.09) | 0.338 |
| Other Government | 4 (0.8) | 1.46 (0.93 – 2.30) | 0.101 | 1.26 (0.71 – 2.05) | 0.435 |
| Not Insured | 79 (16.0) | 1.18 (0.28 – 4.97) | 0.821 | 0.86 (0.20 – 3.80) | 0.843 |
Table 3: Univariate and multivariate predictors of mortality (treated with either IMRT or 3DCRT).
IMRT + BT Boost vs. 3DCRT + BT Boost
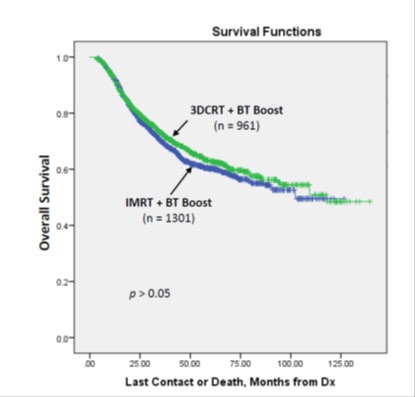
Generally, EBRT is followed by BT boost as the standard of practice for treating stage IB-IIB cervical patients. It is interesting to note (Figure 4) that when BT boost is added to either IMRT or 3DCRT the difference in OS is very little and statistically not significant (p >0.05). Seems BT boost is effective in eliminating the shortcoming in IMRT so far the overall survival is concerned.
Discussion
Since the introduction of IMRT technology in 2000, it has been used in treating various cancers for superiority in reducing both early and late side effects and in improving outcome. While it has been accepted as the standard approach in head and neck malignancies and prostate cancers, for any other cancer types it remains controversial. This is mostly because of lack of good randomized data proving the benefit of IMRT. Similarly, in cervical cancers the use of IMRT has controversies. Although more recently, GEC- ESTRO has recommended the use of IMRT technique over 3DCRT technique in the treatment of cervical cancer. There is no large randomized data comparing two modalities. The study from India has its own limitation with small sample size. The meta-analysis recently published suggested equivalent 3-year survival outcome with better toxicity profile of IMRT [23]. However, this meta-analysis included 6 studies of which 3 were prospective and rest retrospective showing strong evidence in support of IMRT. In this report, analyzing NCDB data in the modern era between 2004-2014 we showed the use of IMRT has steadily increased since 2004 from under 20% to 60% in 2009 and remains steady afterwards. We also demonstrated that while EBRT was used as a boost modality, brachytherapy boost remains the primary modality for boost treatment. Long-term (11 yrs) outcome, overall survival, analysis using NCDB data revealed that 3DCRT modality performed better than IMRT for cervical cancer patients when treated without brachytherapy boost. This relative inferiority in overall survival of IMRT may be due the geometric miss or under dosing of the tumor/target which may be caused by the finer/over modulation of the radiation beam in IMRT technique, while the daily variation of patient’s anatomy as well as the tumor/target motion and set up interplay might not be negligible. If the daily position of the tumor is uncertain, the beam modulation in IMRT may result in inadequate coverage of the target. Whereas, the 3DCRT is less susceptible to inter-fractional or inter- fractional uncertainties of tumor/target position as well as the interplay of small IMRT segments and the target location. Therefore, application of IMRT vs 3DCRT should be carefully decided based on the daily variation of patient’s anatomy and other associated setup issues. The use of IMRT also requires daily imaging for better target positioning and also needs robust QA program to implement it. Cervical cancer is a disease of low income countries with limited resources. It also requires a steep learning curve that may be difficult to achieve in the poor countries. With wide acceptance of IMRT utilization without proper QA proves or IGRT in these low income countries can have a detrimental outcome and needs to be considered.
This study has some limitations as well. It is not possible to make any comments regarding the toxicity from this database as it is not captured in the NCDB data base. Given the retrospective nature of the study, the patient selection may have bias. Patients were treated in different facilities with varied standard. However, NCDB is the largest hospital- based real-world data set in the United States capturing 70% of all new cancer diagnosis. We included patients from 2004 with more modern technique with information on chemotherapy use. To avoid immortal time bias, we analyzed time specific survival outcome rather than median survival.
Conclusion
It appears from this large real-world data base analysis that 3DCRT modality performed better than IMRT in terms of overall survival of cervical cancer patients when no brachytherapy boost was utilized. However, the difference in OS disappeared when brachytherapy boost was added to either modality of EBRT (IMRT or 3DCRT). Therefore, it is important to use the brachytherapy boost following the EBRT (IMRT or 3DCRT).
Conflict of Interest Statement
The authors have no conflicts of interest or disclosures.
Acknowledgment
The National Cancer Database (NCDB) is jointly sponsored by the American College of Surgeons and the American Cancer Society.
References
-
de Souza Lawrence L (2017) Radiation Oncology Management of Stage I-III Cervix Cancer. Surg Oncol Clin N Am 26(3): 477-489.
-
Pötter R, Georg P, Dimopoulos JCA, Grimm M, Berger D, et al. (2011) Clinical outcome of protocol based image (MRI) guided adaptive brachytherapy combined with 3D conformal radiotherapy with or without chemotherapy in patients with locally advanced cervical cancer. Radiother Oncol 100(1): 116-123.
-
Ribeiro I, Janssen H, De Brabandere M, Nulens A, De Bal D, et al. (2016) Long term experience with 3D image guided brachytherapy and clinical outcome in cervical cancer patients. Radiother Oncol 120(3): 447-454.
-
Du XL, Tao J, Sheng XG, Lu CH, Yu H, et al. (2012) Intensity-modulated radiation therapy for advanced cervical cancer: A comparison of dosimetric and clinical outcomes with conventional radiotherapy. Gynecol Oncol 125(1): 152-157.
-
Lujan AE, Mundt AJ, Yamada SD, Rotmensch J, Roeske JC (2003) Intensity-modulated radiotherapy as a means of reducing dose to bone marrow in gynecologic patients receiving whole pelvic radiotherapy. Int J Radiat Oncol Biol Phys 57(2): 516-521.
-
Brixey CJ, Roeske JC, Lujan AE, Yamada SD, Rotmensch J, et al. (2002) Impact of intensity modulated radiotherapy on acute hematologic toxicity in women with gynecologic malignancies. Int J Radiat Oncol Biol Phys 54(5): 1388- 1396.
-
Kidd AE, Siegel BA, Dehdashti F, Rader JS, Mutic S, et al. (2010) Clinical outcomes of definitive intensity modulated radiation therapy with fluro-deoxy glucose positron emission tomography simulation in patients with locally advanced cervical cancers. Int J Radiat Oncol Biol Phys 77(4): 1085-1091.
-
Wang W, Meng Q, Hou X, Lian X, Yan J, et al. (2017) Efficacy and toxicity of image-guided intensity-modulated radiation therapy combined with dose-escalated brachytherapy for stage IIB cervical cancer. Oncotarget 8(61): 102965-102973.
-
Naik A, Gurjar OP, Gupta KL, Singh K, Nag P, et al. (2016) Comparison of dosimetric parameters and acute toxicity of intensity-modulated and three-dimensional radiotherapy in patients with cervix carcinoma: a randomized prospective study. Cancer Radiothérapie 20(5): 370-376.
-
Klopp AH, Yeung AR, Deshmukh S, Gil KM, Wenzel L, et al. (2016) A Phase III Randomized Trial Comparing Patient- Reported Toxicity and Quality of Life (QOL) During Pelvic Intensity Modulated Radiation Therapy as Compared to Conventional Radiation Therapy. Int J Radiat Oncol 96(2): S3.
-
Thawani N, Vainshtein JM, Hannan R, Kalnicki S, Yaparpalvi R, et al. (2008) Comparison of intensity modulated radiation therapy (IMRT) with conventional radiotherapy for cervical cancer with concurrent cisplatin (CDDP). J Clin Oncol 26(15): 5562.
-
Hasselle MD, Rose BS, Kochanski JD, Nath SK, Bafana R, et al. (2011) Clinical outcomes of intensity-modulated pelvic radiation therapy for carcinoma of the cervix. Int J Radiat Oncol Biol Phys 80(5): 1436-1445.
-
Gandhi AK, Sharma DN, Rath GK, Julka PK, Subramani V, et al. (2013) Early clinical outcomes and toxicity of intensity modulated versus conventional pelvic radiation therapy for locally advanced cervix carcinoma: a prospective randomized study. Int J Radiat Oncol Biol Phys 87(3): 542-548.
-
Mundt AJ, Lujan AE, Rotmensch J, Waggoner SE, Yamada SS, et al. (2002) Intensity-modulated whole pelvic radiotherapy in women with gynecologic malignancies. Int J Radiat Oncol Biol Phys 52(5): 1330-1337.
-
Mundt AJ, Mell LK, Roeske JC (2003) Preliminary analysis of chronic gastrointestinal toxicity in gynecology patients treated with intensity modulated whole pelvic radiation therapy. Int J Radiat Oncol Biol Phys 56(5): 1354-1360.
-
Beriwal S, Gan GN, Heron DE, Selvaraj RN, Kim H, et al. (2007) Early clinical outcome with concurrent chemotherapy and extended-field, intensity-modulated radiotherapy for cervical cancer. Int J Radiat Oncol Biol Phys 68(1): 166-171.
-
Chen CC, Lin JC, Jan JS, Shih-Chu H, Wang L, et al. (2011) Definitive intensity-modulated radiation therapy with concurrent chemotherapy for patients with locally advanced cervical cancer. Gynecol Oncol 122(1): 9-13.
-
Macdonald DM, Lin LL, Biehl K, Mutic S, Nantz R, et al. (2008) Combined intensity-modulated radiation therapy and brachytherapy in the treatment of cervical cancer. Int J Radiat Oncol Biol Phys 71(2): 618-624.
-
Sturdza A, Pötter R, Fokdal LU, Haie-Meder C, Tan LT, et al. (2016) Image guided brachytherapy in locally advanced cervical cancer: improved pelvic control and survival in RetroEMBRACE, a multicenter cohort study. Radiother Oncol 120(3): 428-433.
-
Lin AJ, Kidd E, Dehdashti F, Siegel BA, Mutic S, et al. (2019) Intensity modulated radiation therapy and image-guided adapted brachytherapy for cervix cancer. Int J Radiat Oncol Biol Phys 103(5): 1088-1097.
-
Potter R, Tanderup K, Kirisits C, de Leeuw A, Kirchheiner K, et al. (2018) The EMBRACE II study: The outcome and prospect of two decades of evolution within the GEC- ESTRO GYN working group and the EMBRACE studies. Clin Transl Radiat Oncol 9: 48-60.
-
The National Cancer Data Base.
-
Lin Y, Chen K, Lu Z, Zhao L, Tao Y, et al. (2018) Intensity- modulated radiation therapy for definitive treatment of cervical cancer: a meta-analysis. Radiation Oncology 13(1): 177.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma