The Intraoperative Correlation of the Sugarbakers Peritoneal Cancer Index for the Surgical Resectability of Advanced Epithelial Ovarian Cancers
Aim and Objectives: This study aimed to investigate Sugarbaker's peritoneal cancer index (PCI) as an objective indicator for the resectability of epithelial ovarian carcinoma (EOC), as depicted in the study using the completeness of cytoreduction score (CCS). Currently, the intraoperative assessment of operability in EOC surgery is primarily a subjective measurement that is dependent on the surgeon. Methods: The prospective data from 51 patients with EOC FIGO stage III to IV who underwent surgery in a regional cancer institute between July 2015 and June 2017. The PCI and the CCS was recorded intraoperatively using sugarbaker’s PCI chart. The details of cytoreductive procedures done were documented in the patient’s file. A spearman’s rank correlation applied to analyse the surgical predictability of CCS using the PCI. Results: All the 51 cases underwent gynecological surgeries. More than 49% (25 of 51) patients required extensive surgeries in the upper abdomen. The mean PCI’s in CCS 0, CCS 1, CCS 2, and CCS 3 were 8.1, 12.8, 18.6, and 18.5 respectively. There was a strong correlation found between PCI and CCS, and the lower PCI is significantly (P-value <0.0001, r =0.69) associated with better optimal CCS. The 45 (88.2%) of 51 recovered uneventfully, four cases (7.8%) developed surgical site infections, and there were two deaths (3.9%). Conclusion: The PCI more precisely defined the heterogeneous group of patients with EOC stage III. The PCI provided objectivity and reproducibility, and it seems to be a reliable indicator for EOC resectability. We purpose a multi-centric study to define cut-off PCI for the optimal resectability of advanced EOC. Key Words: Epithelial Ovarian cancer, Carcinomatosis, Peritoneal cancer index, Resectability, Cytoreductive surgery.
Introduction
Epithelial ovarian cancer (EOC) is the gynecological malignancy with the highest mortality rate [1]. The treatment is challenging because EOCs are typically diagnosed in advanced stages after the development of peritoneal metastases. Due to this metastatic pattern, surgery for an EOC is often multivisceral and the surgeon must be highly skilled [2]. Primary debulking surgery (PDS)
followed by platinum-based chemotherapy has long been considered the only standard treatment for advanced EOC [3]. The aim of primary surgical treatment of EOC was the complete resection of the tumor [4, 5, 6]. Of the established prognosis factors of EOC, the amount of tumor that remains postoperatively is the one of the prognostic factor that can be effectively influenced [2]. Complete tumor removal is not dependent only on the ability of the gynecological oncologist to perform a multivisceral operation. An excellent surgeon cannot always ensure complete removal of all tumors, and the ability to decide whether the findings are resectable or inoperable is also important.
The preoperative assessment of operability is primarily dependent on the surgeon and is thus subjective. This was currently shown in the CHORUS trial, where a rate of complete resection of only 15% at primary surgery was achieved [7]. Possibly operational options are often underestimated and neoadjuvant chemotherapy is preferred too early. There is not a quantitative and reproducible assessment. The predictive factors for the resectability of EOCs were analyzed in several studies. A well-researched predictor is the AGO score, which was designed for recurrent ovarian cancer only. On the basis of 3 factors (resection at first surgery, performance status, presence/absence of ascites) resectability can be estimated [8, 9].
Among the general surgeons at many institutions, the peritoneal cancer index (PCI) is part of the surgical therapy for gastrointestinal carcinomas [10, 11]. The PCI and the completeness of cytoreduction score (CCS) were developed for gastrointestinal carcinoma in 1996 by Jacquet and Sugarbaker. These scores were meant to standardize the management of patients experiencing peritoneal metastatic gastrointestinal carcinoma [12]. The new WHO classification 2014, it incorporates many major scientific advances in our understanding of epithelial cancers of the ovary, fallopian tubes, and peritoneum. It recognizes probable precursor events, lineages, and molecular characteristics, and the EOC is considered as one of the peritoneal surface malignancy [13].
The PCI scores are used for the intraoperative quantification of peritoneal carcinomatosis and applied at the beginning of the exploration of the abdomen and pelvis, before the start of operative measures. The CCS is applied after completion of the operative measures. Currently, the intraoperative assessment of operability in EOC surgery is primarily a subjective measurement that is dependent on the surgeon. Therefore, we aimed to conduct this study to find a parameter, which, at the beginning of the operation, allows for an objective and standardized assessment of the site and resectability of an ovarian tumor. As the PCI was efficacious in general surgery, our aim was to investigate whether this score could be applied to EOCs.
Methods
This is a prospective study of 51 patients with advanced epithelial ovarian cancers (EOC) International Federation of Gynecology and Obstetrics (FIGO) stage III to IV who underwent cytoreductive surgery in the department of Gynaecological Oncology at a regional cancer institute between July 2015 and June 2017 were analyzed. The departmental board approval was obtained.
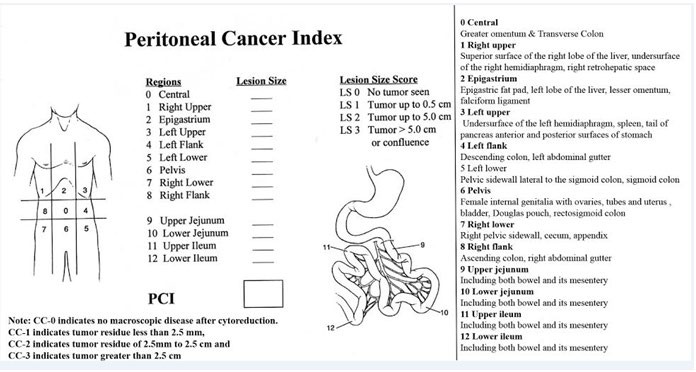
The departmental policy for selecting patients to primary debulking surgery is based on patients good performance status Eastern Cooperative Oncology Group (ECOG) 0-1, optimal resectibility on CT scan study, clinical examination and serum albumin >3g/dl, and the patients with poor performance status ECOG >2, serum albumin <3g/dl, malignant pleural effusion, optimally non-resectable disease on CT scan, age >80 years will receive 2-3 courses neoadjuvant chemotherapy (NACT) followed by interval cytoreduction (IDS). Patients with FIGO stage IVB as well as those assigned to receive neoadjuvant treatment were excluded from the study. The PCI and the CCS was recorded intraoperatively using sugarbaker’s PCI chart (Figure 1). The details of cytoreductive procedures done were documented in the patient’s file. A spearman’s rank correlation test applied to analyse the surgical predictability of CCS using the PCI.
Results
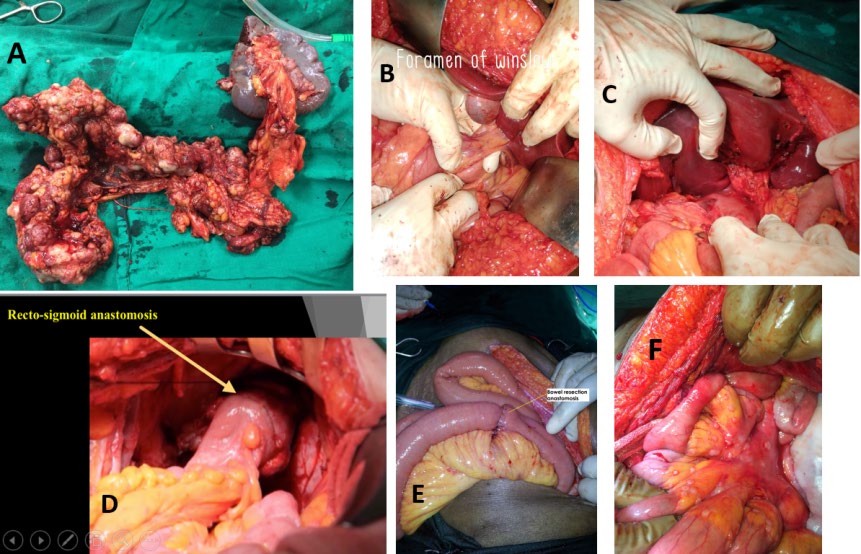
A total of 51 cases with advanced EOC were recorded for the PCI at the beginning PDS and CCS was recorded at the end of PDS and the details of various cytoreductive procedures in each patient were recorded in patient’s files (Table 1). All the 51 cases underwent gynecological procedures, ovarian tumour debulking (TD) with total abdominal hysterectomy with bilateral salpingo-opherectomy (TAHBSO) with total omentectomy (TO) and one of the case which was a post- hysterectomy underwent ovarian tumour debulking with bilateral salpingo-opherectomy with total omentectomy (Table 1), and the additional surgical procedures done to achieve optimal CCS were 29 (56.9%) cases required pelvic peritonectomies, 11(21.6%) cases abdominal peritonectomies, 12 (23.5%) cases diaphragm stripping with or without diaphragm resection / and or liver surface deposit excision (Figure 2), nine cases (17.6%) underwent appendicectomy, six cases (11.8%) with mesenteric deposits excision with or without fulguration, three cases (5.9%) large bowel resection and anastomosis, two cases (3.9%) small bowel resection and anastomosis, one case required cholecystectomy and porta hepatis tumour debulking and one case needed splenectomy (Table 1) (Figure 3).
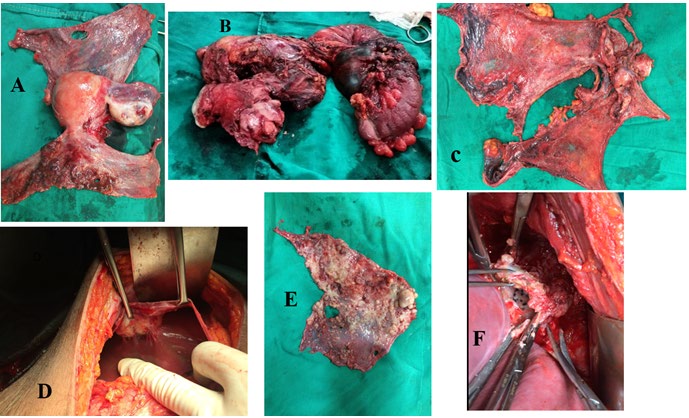
Figure 2: A= enbloc pelvic peritonectomy specimen with uterus and ovaries, B= Enbloc resection of uterus with ovarian tumor and recto-sigmoid in an ovarian cancer infiltrating recto-sigmoid mesentery, C= enbloc pelvic and abdominal peritonectomy, D= perihepatic deposit excision with diaphragm peritonectomy, E= diaphragm peritoneum stripped with tumor deposits, F= diaphragm central tendon excision with a deposit.
| Surgical Procedures | Number |
| Gynaecological procedures: Tumour debulking with TAHBSO with RPLND and total omentectomy | 51 |
| Pelvic peritonectomy (bladder and pouch of Douglas) | 29 |
| Abdominal (para colic) peritonectomy | 11 |
| Diaphragm stripping/resection with or without liver surface tumor excision | 12 |
| Appendicectomy | 9 |
| Mesenteric deposit excision/fulguration | 6 |
| Large Bowel resection anastomosis | 3 |
| Small bowel resection anastomosis | 2 |
| Cholecystectomy with porta hepatis tumor debulking | 1 |
| Splenectomy | 1 |
Table 1: The types of cytoreductive procedures done.
The table 2 reveals the mean PCI’s in CCS 0, CCS 1, CCS 2, CCS 3 were 8.1, 12.8, 18.6, 18.5 respectively, and the PCI range in CCS 0 was 03-19, CCS 1 was 09-21, CCS 2 was 12 -34 and CCS 3 it was 18-19. A spearman’s rank correlation test reveals a strong correlation found between PCI and CCS, and the lower PCI is significantly (P-value <0.0001, r =0.69) associated with better optimal CCS (Table 3).
| CCS 0 | CCS 1 | CCS 2 | CCS 3 | ||
|---|---|---|---|---|---|
| PCI range | 19 | 14 | 13 | 18 | |
| PCI range | 10 | 21 | 34 | 19 | |
| PCI range | 17 | 15 | 21 | ||
| PCI range | 5 | 15 | 21 | ||
| PCI range | 12 | 17 | 14 | ||
| PCI range | 6 | 18 | 16 | ||
| PCI range | 13 | 9 | 18 | ||
| PCI range | 7 | 13 | 12 | ||
| PCI range | 8 | 11 | |||
| PCI range | 7 | 9 | |||
| PCI range | 4 | 10 | |||
| PCI range | 5 | 13 | |||
| PCI range | 9 | 11 | |||
| PCI range | 7 | 10 | |||
| PCI range | 6 | 11 | |||
| PCI range | 7 | 9 | |||
| PCI range | 5 | 11 | |||
| PCI range | 4 | 12 | |||
| PCI range | 3 | 13 | |||
| PCI range | 11 | ||||
| PCI range | 14 | ||||
| PCI range | 15 | ||||
| *Mean PCI | 8.1 | 12.8 | 18.6 | 18.5 | |
| Total cases | 19 | 22 | 8 | 2 | |
| PCI= peritoneal cancer index, CCS= completeness cytoreduction score. | |||||
| *A spearman's rank correlation test P-value <0.0001, r=0.69 |
Table 2: PCI and CCS distribution.
| Principle | Progressiveness/Aim | Advantages | Disadvantages | |
|---|---|---|---|---|
| Eisenkop score [15] | Score from 0 to 15; 5 anatomical regions; ranks from 0 to 3 per region | Ovary; prediction survival | Includes pelvic and para-aortic lymph nodes | Less precise than the PCI |
| Fagotti score [16] | Score from 0 to 14; 7 anatomical structures; 0/2 points per region | Ovary; prediction resectability | Concise | Based on laparoscopy |
| Fagotti-modified score [17] | Score from 0 to 8; 4 anatomical structures; 0/2 points per region | Ovary; prediction resectability | Concise | Based on laparoscopy |
| Gilly classification [18] | G0-G4; information regarding location of carcinomatosis (locally, disseminated) | Colorectal tumors | Concise | Imprecise localization of the lesions |
| P-Score of the Japanese Research Society of Gastric Cancer [19] | P0-P3; information about the location of the metastases | Gastric carcinoma | Specially for gastric carcinoma | Imprecise localization and sizing of the lesions only for gastric carcinoma |
| PCI [12] | Score from 0 to 39; 13 abdominal and pelvic regions, per region LS 0-3 | Gastrointestinal tumors; management standardized | Very precise description of the peritoneal carcinomatosis, can be universally used | Lymph nodes not included |
| Simplified PCI [20] | Score from 0 to 21; 7 abdominal and pelvic regions, per region LS 0-3 | Colorectal and appendix tumors; staging | Concise | Less precise than the PCI |
Table 3: Of these scores, the PCI is the most precise for describing peritoneal carcinomas. Because the PCI creates 13 abdominope
The post-operative period events in our study, the 45 (88.2%) of 51 recovered uneventfully, four cases (7.8%) developed surgical site infections were managed with sensitive antibiotics and sterile dressings. There were two deaths (3.9%) one case developed acute pulmonary thromboembolism on 5th post-operative day, and the other case had a myocardial infarction on 3rd post-operative day.
Discussion
The majority of EOCs are diagnosed at an advanced stage. The FIGO classification reflects tumor spread relatively imprecisely, particularly in disease stages III and IV. In FIGO stage III is a heterogeneous group, patients with peritoneal metastases outside the pelvis are grouped with patients without peritoneal metastases whose lymph nodes are affected [14]. Various scores have been developed to describe tumor spread more precisely. Among others, the Eisenkop-, Fagotti-, and the Fagotti-modified scores have been developed to describe EOCs. For gastrointestinal carcinomas, the classification scores include the Simplified PCI, the P-Score of the Japanese Research Society for Gastric Cancer, and the Gilly classification. An overview of those scores is shown in Table 4. Of these scores, the PCI is the most precise for describing peritoneal carcinomas. Because the PCI creates 13 abdominopelvic regions, the description of the affected zones is markedly precise. The lesion size component allows for a description of the size of the tumor mass in the score. The PCI is the most precise score for describing the location of a carcinomatosis. The other scores create only 2 to 7 abdominopelvic regions. Only the PCI score and the Gilly classification refer to the size of the tumor mass. Other scores can be applied to EOCs to a certain extent. The Fagotti- and the Fagotti-modified scores are laparoscopy based. The P-score is particularly adapted for stomach cancer. The PCI can be applied, in principle, to any type of peritoneal cancer from any source. This score describes the distribution of tumors in the abdomen and pelvis, without particularly weighing a certain region. For the prognosis of resectability, the PCI and Fagotti-modified score were the most suitable. In 2012, Koppitsch and Sebek analyzed various preoperative and intraoperative classification systems. They emphasized that the PCI can be used universally and with much more precision than the P-score and the Gilly classification [21]. Our results have shown that the PCI can be used for EOCs. It precisely mirrors the extent of the tumor and can be used for the assessment of resectability. Our statistical analysis resulted in to a strong correlation of the PCI to the surgical outcome, shown in the study by the CCS.
The current practices by most Gynaecological oncological surgeons is the intraoperative assessment of resectability in EOC surgery is primarily a subjective measurement that is dependent on the surgeon. It was the aim of this study to identify the PCI as a parameter that would standardize and objectify the management of EOCs. The entire site must be explored using a predefined scheme to determine the PCI. The assignment of a lesion size to each region is simple and clear, and it automatically leads to a precise exploration. There is little room for subjective interpretation in the given scheme.
In 1998, Sugarbaker reported that the PCI has 2 weak points. In cases in which more critical areas are affected, that is, the root of the mesentery, a possibly lower score does not properly reflect that it cannot be respected. In the case of a non-invasive pseudomyxoma peritonei, it is possible that even with a high PCI, surgery can result in a tumor- free outcome. In these cases, the PCI does not reflect the resectability [22]. In our study two cases had PCI with PCI 18 and 19 had CCC 3 due involvement of tumour deposits at the root of mesentery at multiple places. One case with PCI 19 achieved CCS 0 as the carcinomatosis was confined mainly over the parietal peritoneum.
The root of the mesentery was significantly affected in more than 11.8 % (6/51) of the cases. More than 49% of the patients required extensive intervention in the upper abdomen such as diaphragm stripping/resection with few cases underwent liver surface tumour excision, splenectomy, resection of the lesser omentum, and cholecystectomy with porta hepatis tumour debulking. The grading of peritoneal carcinomatosis, according to Sugarbaker, requires the precise exploration of 13 regions. Frequently, if problematic regions such as the celiac trunk or portal vein are affected, it is impossible to achieve a macroscopic tumor-free outcome. The apparently low rate of macroscopically tumor-free outcomes possibly reflects the precise exploration of these problem regions in which we could not achieve freedom from tumors despite advanced surgical techniques.
In this study, the PCI and CCS scores were determined prospectively, based on intraoperative findings, and a possible criticism of the study is, it’s a single centre small number prospective determination of the scores. For this analysis, consistency in the determination of the scores was efficacious and was assured by having the determination performed by the same person.
A study to investigate whether there is a cut-off that would be useful for determining resectability would be useful. May be PCI could then be of help deciding on operability. Of course, the surgeon will always use several parameters to decide on operability, other than only the PCI. The patient’s general status and the location of the tumor play a role, too. In case of inoperability, the authors would always remove the omentum as this simple procedure leads to an enormous relief of symptoms with improvement in quality of life. It is possible that the PCI could be used to measure the quality of the surgeon and thus create an opportunity for comparison. The objective documentation is preferred over the currently practised subjective assessment.
The PCI score, which is already established in general surgery, seems applicable to other peritoneal metastasizing tumors. It is markedly precise and all abdominal and pelvic regions are weighted equally in the description. It is a useful extension of the existing classification systems for the treatment of EOCs and could be used as a parameter for the assessment of resectability (Table 3).
Conclusion
The PCI more precisely defined the heterogeneous group of patients with EOC stage III. The PCI provided objectivity and reproducibility, and it seems to be a reliable indicator for EOC resectability. We purpose a multi-centric study to define cut-off PCI for the optimal resectability of advanced EOC.
References
-
Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, et al. (2015) Global cancer statistics, 2012. CA Cancer J Clin 65(2): 87-108.
-
Lampe B, Kroll N, Piso P, Forner DM, Mallmann P (2015) Prognostic Significance of Sugarbaker’s Peritoneal Cancer Index for the Operability of Ovarian Carcinoma. Int J Gynecol Cancer 25(1): 135-144.
-
Ledermann JA, Raja FA, Fotopoulou C, AGonzalez- Martin A, Colombo N, et al. (2013) Newly diagnosed and relapsed epithelial ovarian carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow- up. Ann Oncol 24(6): vi24-vi32.
-
du Bois A, Reuss A, Pujade-Lauraine E, Harter P, Ray- Coquard I, et al. (2009) Role of surgical outcome as prognostic factor in advanced epithelial ovarian cancer: a combined exploratory analysis of 3 prospectively randomized phase 3 multicenter trials by the Arbeitsgemeinschaft Gynaekologische Onkologie Studiengruppe Ovarialkarzinom (AGO-Ovar) and the Groupe d’Investigateurs Nationaux Pour les Etudes des Cancers de l’Ovaire (GINECO). Cancer 115(6): 1234- 1244.
-
Luyckx M, Leblanc E, Filleron T, Morice P, Darai E, et al. (2012) Maximal cytoreduction in patients with FIGO stage IIIC to stage IV ovarian, fallopian, and peritoneal cancer in day-to-day practice: a retrospective French Multicentric Study. Int J Gynecol Cancer 22(8): 1337- 1343.
-
Ghisoni E, Katsaros D, Maggiorotto F, Aglietta M, Vaira M, et al. (2018) A predictive score for optimal cytoreduction at interval debulking surgery in epithelial ovarian cancer: a two- centers experience. J Ovarian Res 11: 42.
-
Kehoe S, Hook J, Nankivell M, Jayson GC, Kitchener HC, et al. (2013) Chemotherapy or upfront surgery for newly diagnosed advanced ovarian cancer: results from the MRC CHORUS trial. J Clin Oncol 31(15).
-
Harter P, du Bois A, Hahmann M, Hasenburg A, Burges A, et al. (2006) Surgery in recurrent ovarian cancer: the Arbeitsgemeinschaft Gynaekologische Onkologie (AGO) DESKTOP OVAR trial. Ann Surg Oncol 13(12): 1702- 1710.
-
Harter P, Sehouli J (2011) Prospective validation study of a predictive score for operability of recurrent ovarian cancer: the Multicenter Intergroup Study DESKTOP II. A project of the AGO Kommission OVAR, AGO Study Group, NOGGO, AGO-Austria, and MITO. Int J Gynecol Cancer 21(2): 289-295.
-
Cavaliere F, De Simone M, Virzi S, Deraco M, Rossi CR, et al. (2011) Prognostic factors and oncologic outcome in 146 patients with colorectal peritoneal carcinomatosis treated with cytoreductive surgery combined with hyperthermic intraperitoneal chemotherapy: Italian multicenter study S.I.T.I.L.O. Eur J Surg Oncol 37(2): 148- 154.
-
Yonemura Y, Tsukiyama G, Miyata R, Sako S, Endou Y, et al. (2010) Indication of peritonectomy for peritoneal dissemination. Gan To Kagaku Ryoho 37(12): 2306- 2311.
-
Jacquet P, Sugarbaker PH (1996) Current methodologies for clinical assessment of patients with peritoneal carcinomatosis. J Exp Clin Cancer Res 15: 49-57.
-
Meinhold-Heerlein I, Fotopoulou C, Harter P, Kurzeder C, Mustea A, et al. (2016) The new WHO classification of ovarian, fallopian tube, and primary peritoneal cancer and its clinical implications. Arch Gynecol Obstet 293(4): 695-700.
-
Prat J, FIGO Committee on Gynecologic Oncology (2015) FIGO’s staging classification for cancer of the ovary, fallopian tube, and peritoneum: abridged republication. J Gynecol Oncol 26(2): 87-89.
-
Eisenkop SM, Spirtos NM, Friedman RL, Michael Lin WC, Pisani AL, et al. (2003) Relative influences of tumor volume before surgery and the cytoreductive outcome on survival for patients with advanced ovarian cancer: a prospective study. Gynecol Oncol 90(2): 390-396.
-
Fagotti A, Ferrandina G, Fanfani F, Ercoli A, Lorusso D, et al. (2006) A laparoscopy-based score to predict surgical outcome in patients with advanced ovarian carcinoma: a pilot study. Ann Surg Oncol 13(8): 1156-1161.
-
Brun JL, Rouzier R, Uzan S, Daraï E (2008) External validation of a laparoscopic-based score to evaluate resectability of advanced ovarian cancers: clues for a simplified score. Gynecol Oncol 110(3): 354-359.
-
Gilly FN, Carry PY, Sayag AC, Brachet A, Panteix G, et al. (1994) Regional chemotherapy (with mitomycin C) and intra-operative hyperthermia for digestive cancers with peritoneal carcinomatosis. Hepatogastroenterology 41(2): 124-129.
-
Kajitani T (1981) The general rules for the gastric cancer study in surgery and pathology. I. Clinical classification. Jpn J Surg 11(2): 127-139.
-
Verwaal VJ, van Tinteren H, van Ruth S, Zoetmulder FAN (2004) Predicting the survival of patients with peritoneal carcinomatosis of colorectal origin treated by aggressive cytoreduction and hyperthermic intraperitoneal chemotherapy. Br J Surg 91(6): 739-746.
-
Koppitsch C, Sebek M (2012) Peritoneal neoplasms: scoring systems and their significance. Interdisz Onkol 4: 12-16.
-
Sugarbaker PH (1998) Current indications for cytoreductive surgery and intraperitoneal chemotherapy. In: Sugarbaker PH, Management of Peritoneal Surface Malignancy Using Intraperitoneal Chemotherapy and Cytoreductive Surgery, A Manual for Physicians and Nurses, Grand Rapids, MI: The Ludann Company.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma