Rectal Neuroendocrine Tumor: Clinical Case Report
The rectal neuroendocrine tumor (RNT) is a rare neoplasm that initiates in the neuroendocrine cells of the digestive tract called Kulchitsky cells, which originate from Lieberkün crypts. About 50% of patients are asymptomatic and their diagnosis is made incidentally by routine colonoscopies. This clinical report presents a neoplasm considered rare in a young patient and emphasizes the importance of its early diagnosis. A 23-year-old man, without comorbidities, was referred to the referral service to investigation a single occurrence of postprandial abdominal pain in the left flank. Polypoid fragment of the rectal mucosa was extracted during a colonoscopy, making it possible to perform a complete removal with free margins of the rectal NET. After histopathological and immunohistochemical evaluation, the diagnosis of RNT grade 1 was made. Although RNT is rare and asymptomatic, early screening is necessary to facilitate diagnosis in the early stage of the disease, leading to a greater possibility of treatment and a better prognosis of the disease.
Introduction
The neuroendocrine tumor (NET) had its first description in 1888 by Lubarsch, being found in an autopsy of multiple neuroendocrine tumors in the distal ileum of two patients [1]. The neuroendocrine system consists of endocrine and neuronal cells. These cells share the same characteristics, express common markers, and secrete substances such as hormones, neurotransmitters, or neuropeptides. The characteristics of tumors originating in this system depend on their site of origin, and functional substances may or may not be secreted, with the gastrointestinal tract being the main tumor site [2, 3, 4].
Rectal NETs correspond to 0.49% of malignant tumors, having a much lower incidence when compared to rectal adenocarcinoma [2]. Data from the Surveillance, Epidemiology and End Results (SEER) evidenced 5894 cases with colorectal NET from 2000 to 2015, being 98.1% grades 1-2, and 1.9% grade 3 [5]. The incidence of rectal NETs have been increasing over the last decades, and represented 29% of all gastroenteropancreatic tumors (GEP-NETs) in the latest report, establishing the rectum as the most common location, slightly above the small intestine [6]. The mean age of diagnosis of this neoplasm is 56 years old, with no significant prevalence in gender, race, and heredity [7, 8].
Most rectal NETs do not present symptoms that are specific and that may be a differential to awaken a diagnostic hypothesis for the disease. Therefore, the diagnosis is often made unintentionally, through routine colonoscopies and/or when investigating nonspecific intestinal complaints [9].
The present report aims to present a neoplasm considered rare in a young patient, and to emphasize the importance of its early diagnosis, since the rectal neuroendocrine tumor is the most often present in an asymptomatic way and can be identified in routine colonoscopy exams.
Case Report
This study presents a case of a 23-year-old male patient, with a medical history of dengue fever and Chikungunya, without any comorbidities and family history of breast neoplasia (mother). One year before consultation, he presented a single episode of postprandial abdominal pain in the left flank, leading, to an investigation by doing the following tests: computed tomography (CT) of the abdomen and pelvis, which presented colonic diverticula in the sigmoid region; investigative colonoscopy, in which incidentally a polyp was found in the rectum; chest CT and magnetic resonance imaging of the pelvis, both without alterations. Laboratory tests didn´t present alterations in relation to the reference values adopted by the laboratory exams: leukocytes 4300 mm³, hemoglobin 14.8g/dL, hematocrit 43.2%, platelets 267.000/mm³, TGO 30 U/L, TGP 26 U/L, GGT 36 U/L and alkaline phosphatase 69 U/L.
The polypoid fragment measuring 0.5 cm in the largest axis, extracted from the rectal mucosa, was referred to a laboratory of pathological anatomy, and after analysis, an architectural alteration of the tissue with proliferation of niches and cell cords was identified in the middle of desmoplasia, which may correspond to a carcinoid tumor, and after analysis, an immunohistochemical study was performed for diagnostic confirmation (Figure 1).
In the immunohistochemical evaluation, positivity was identified for the markers synaptophysin, chromogranin-A, cytokeratin, and Ki-67, confirming the diagnosis of grade 1 RNT. After diagnosis, a revision of the biopsy specimen was performed in order to evaluate the surgical margins and the mitotic index. Besides, the pathological staging (pTNM) was requested, confirming the result of well differentiated and low grade 1 rectal NET, with less than 3% of mitotic index. A complete removal of the lesion with surgical margins free of the neoplasm was made, being classified as pathological staging I (pT1aN0M0).
The patient was referred for follow-up consultations and follow-up with a proctologist for future laboratory tests and chromogranin-A dosage. So far, patient is without evidence of locorregional and distance disease.
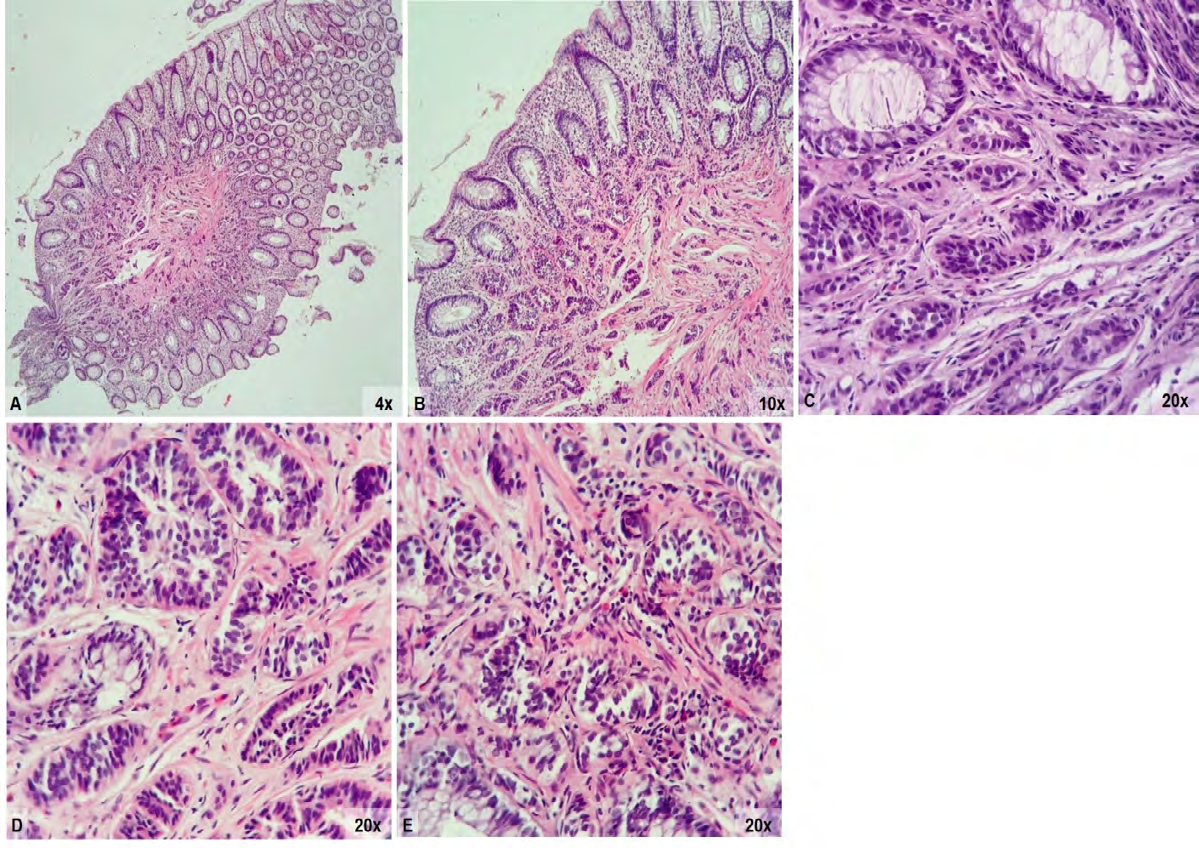
Figure 1: Histopathological features (H&E) A and B: Fragment obtained by mucosectomy of rectal NET limited to the mucosa/ submucosa; C: NET of the rectus consisting of cell nests, sketching glandular lumens; D and E: Neoplastic cells with regular, hyperchromatic with speckled chromatic, rounded or ovoid nuclei, and scarce eosinophilic cytoplasm, with low mitotic index.
Discussion
The rectal neuroendocrine tumor initiates in the neuroendocrine cells of the digestive tract called Kulchitsky cells, which originate from Lieberkün crypts [1]. Due to the increased access to colonoscopy, the incidence of rectal NET has been increasing [2]. Compared to small bowel and colon neuro tumor that produce more serotonin, NET produces glucagon and glycine peptides and are mostly non- functioning tumors, making carcinoid syndromes rare to occur [10].
For the evaluation and histological classification of rectal NET, a basic immunohistochemistry of Ki-67, chromogranin-A and synaptophysin markers is performed. Serum chromogranin A, although not a specific marker, is very useful in follow-up, disease response and progression assessment. High serum concentrations are found in patients with advanced disease and are considered a prognostic marker. In NETs, pancreatic polypeptide, enteroglucagon and β-hCG may be useful tools in the follow-up of this neoplasm. Prostatic acid phosphatase is present in 80-100% of NETs; thus, this marker should always be requested once the diagnosis has been made for the purpose of evaluating the response to treatment and post-surgical follow-up [2].
About 50% of patients are asymptomatic and their diagnosis is made incidentally by routine colonoscopies. Therefore, it highlights the importance of performing screening tests earlier, especially colonoscopy with biopsy, with the aim of making the diagnosis at an early stage of the disease, a period which the probabilities of distant metastases are low and, consequently, the prognosis of the disease is excellent. As the case of the patient reported, the early diagnosis occurred through the incidental discovery of a polyp during colonoscopy, making it possible to perform a complete removal with free margins of the rectal NET. Besides, the association with normal imaging tests that do not evidence metastases, could lead to the cure of the patient [7, 8].
Conclusion
We can conclude that, although rectal neuroendocrine tumors are rare and asymptomatic, early screening is necessary to facilitate diagnosis in the early stage of the disease. Consequently, patients can have a greater possibility of treatment and a better prognosis of the disease.
References
-
Mangueira PA, Fernandes GO, Primo CC, França MAV, Maia HP, et al. (2006) Tumor Carcinóide de Reto. Rev Bras Coloproct 26(2): 162-167.
-
Cesar D, Zanatto RM, da Silva MVMV, De Mello RGELR, De Jesus JP, et al. (2013) Tumores neuroendócrinos do cólon e reto: experiência do Instituto Nacional do Câncer no Brasil. ABCD Arq Bras Cir Dig 26(1): 36-39.
-
Alves JM, de Souza HP, Toneto MC, Reinehr D, Gabbiatti G, et al. (1999) Tumores neuroendócrinos do trato gastrointestinal. Rev Col Bras Cir 26(5): 305-311.
-
Fernandes LC, Pucca L, Matos D (2002) Diagnóstico e tratamento de tumores carcinóides do trato digestivo. Rev Assoc Med Bras 48(1): 87-92.
-
Punekar SR, Kaakour D, Masri-Lavine L, Hajdu C, Newman E, et al. (2020) Characterization of a Novel Entity of G3 (High-grade Well-differentiated) Colorectal Neuroendocrine Tumors (NET) in the SEER Database. Am J Clin Oncol 43(12): 846-849.
-
Rodrigues A, Castro-Poças F, Pedroto I (2015) Neuroendocrine Rectal Tumors. GE Port J Gastroenterol 22(5): 213-220.
-
Guimarães NFRP (2014) Tumores Neuroendócrinos do reto: do diagnóstico à terapêutica Porto: Instituto de Ciências Biomédicas Abel Salazar - Universidade do Porto.
-
Nagtegaal ID, Odze RD, Klimstra D, Paradis V, Ruffe M, et al. (2020) The 2019 WHO classification of tumours of the digestive system. Histopathology 76(2): 182-188.
-
Biazi IM, Sesti FS (2016) Tumor neuroendócrino de reto: relato de caso. GED Gastroenterol Endosc Dig 35(4): 148-154.
-
Viana C, Marques I, Staubus A, Martins SF (2019) Rectal carcinoid tumor: diagnosis and management. J Coloproctol 39(2): 184-189.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma