Sentinel Lymph Node in Breast Cancer, Our First Experience at Nicaragua. Case Report
Morton introduced cutaneous lymphoscintigraphy in melanoma. His results permitted to reproduce sentinel lymph nodes(SLN) in other areas. Krag and Weaver implemented portable gamma radiation detectors in breast cancer. The aim of this article is to describe the first expertise in our hospital using nuclear medicine in breast cancer and the methodological aspects of SLN and reviewing the international literature. Case Report: Female 54 years, no family history of breast cancer. Medical exam detected a mass of 3x2 cm in the upper outer quadrant of the left breast, there is no axillary mass. The Ultrasound: BIRADS IV A. Mammography: BI-RADS V Preoperative Classification: T2N0M0 Tru Cut Biopsy: Invasive carcinoma no type determined. Triple negative. Extension studies were negative. The lymphoscintigraphy done according to international protocol. Methylene blue was used in conjunction with the radiotracer; a periareolar sub dermal injection was given in the operating room. The Surgery performed on the day marked. After localized the scintigraphic hot spots in vivo with the gamma probe Nuclear Lab DGC II. The intraoperative frozen section analysis used with Haematoxylin and Eosin staining. Two SLN reported as metastases Negative. The axillary dissection was deferred. There were no complications. Post-surgical pathologic report showed invasive carcinoma no type determined size 35 x 30 x 28 mm, unifocal. In situ ductal carcinoma and in situ lobular carcinoma unidentified and lympho-vascular unidentified invasion. There is no tumoral extension to the skin. All margins were reported negative.pT2pN0. Conclusion: Each time that a new therapeutic tool is within reach of the oncologic patients, principally when his effectiveness have been demonstrated to long time. It to make true in low income country increase the challenge for her implementation. However, the multidisciplinary effort of the human resources and the help of the technology development of our institutions permeated to jump the hard barrier that this entails, achieving a great achievement to the patients with breast cancer in our country. This first effort is not distant from the reported in the international literature.
Introduction
Morton in 1977 introduced cutaneous lymphoscintigraphy as a method to identify the regional lymph basin of primary drainage for melanoma [1, 2]. Intraoperative mapping permit selective identification and removal of the sentinel lymph nodes (SLN) and their intraoperative evaluation by frozen section and rapid Immunohistochemistry (IHC) The Morton’s results with highest success rate in identifying of the SLN of this specimen in melanoma of trunk or leg was reproduced in other locations as axilla and neck [3]. Krag and Weaver developed a pilot study in patients with breast cancer; they used a gamma probe for radio localization of the SLN. Their results demonstrated that the SLN appears to predict correctly the status of the axilla [4]. The sensitivity for detecting lymphatic metastasis in patients with melanoma and breast carcinoma has significantly increased by the use of SLNB [5, 6].
The 96% negative predictive value of a negative SLN underlines the high reliability of the technique. The principles of SLN are universally accepted as follows. According to the definition by the International Union Against Cancer [7]. The SLN techniques was gaining more popularity due to the results reported in several researchers, therefore it was expanded to other areas as head and neck, cancer of the cervix, stomach, colorectal cancer etc [8, 9, 10, 11]. The aim of this article is to summarize the result of the first expertise in our hospital with a patient in early breast cancer using nuclear medicine. Besides, it helped to the methodological aspects of SLN and review of the international literature.
Case Report
Female 54 years old, no family history of breast cancer. Menarche 12 years old, four pregnancies, three caesarean and one abortion. Two months ago, a mass was felt in her left breast. Medical exam detected a mass of 3x2 cms in the upper outer quadrant of the left breast.
• Ultrasound of left breast reported: In the B area at the 2 HS axis shows a solid mass hypoechoic imagine, irregular edges that measuring 25 x22 mm, no cysts, no ductal ectasia BIRADS IV A (Mammography image: Figure 1-2).
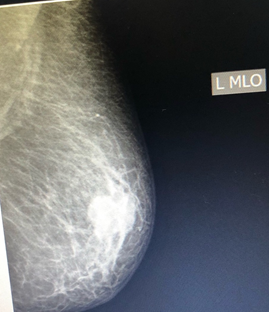
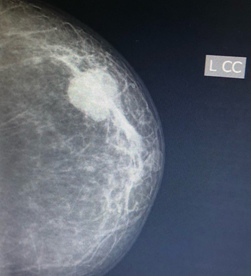
Heterogenous mass with irregular edges BI-RADS V [12].
- Preoperative classification: T2N0M0 [13]
- Tru cut biopsy Q 404-21: invasive carcinoma no type determined [14]. Estrogen and Progesterone hormone receptor negative, HER2 Negative and Ki-67 less than 9% [15]. Extension Studies were Negative. The lymphoscintigraphy was done five hours prior of the surgery. The standard dose that was used: 3 mci of 99mTc with linfofast. The injection site was periareolar applying a soft massage. The Static scintigraphic images were obtained early and late images in anterior, oblique and the mark position acquired by 400 seconds in dual -headed gamma camera: Infinia General Electric and processed using xeleris program. (Figure 3) Focal accumulations of radioactivity (hot spot) seen on scintigraphy were localized and marked on the skin [16].
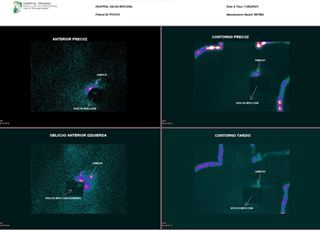
Figure 3: The lymphoscintigraphy, the static scintigraphic images. The Surgery was performed on the day marked, five hours after injection of the tracer; methylene blue was used in conjunction with the radiotracer a periareolar subdermal injection of 1.5 mL was given in the operating room. The radioactive background counts were checked in the lymphatic basin after the excision of the sentinel ‘hot’ node. The first step was an upper out quadrantectomy, and after localizing the scintigraphic hot spots in vivo using the (sterile packed) gamma probe Nuclear Lab DGC II, the site of node localized was crosschecked with the gamma probe.
The intraoperative frozen section analysis was used the standard method with hematoxylin and Eosin staining (H & E), two SLN sent 1,2 x 1x1 cm reported as metastases Negative, and the axillary dissection was deferred. There were no complications and the patient was discharged the next day.
Post-surgical pathologic report showed invasive carcinoma no type determined size 35 x 30 x 28 mm, unifocal. In situ ductal carcinoma and in situ lobular carcinoma unidentified and lympho-vascular unidentified invasion. There is no tumoral extension to the skin. All margin were reported negative.pT2pN0.
Discussion
The Histopathological stage of regional lymph nodal permit to classify the clinical stage during the assessment initial of the patients, principally when the patient is clinically N0. Several factors relate to the primary tumors histologic characteristics, heterogeneity behavior, some toxic habit of the patients between others, can help to predict the higher possibility of microscopic lymph nodal disease [17, 18]. Prior of the research in malignant Melanoma by Morton, generally the patients with tumors with higher risk of occult lymph node disease were approached with lymphadenectomy as prophylactic procedures. However some of the lymph node was negative to metastasis, without modifying the overall survival or the percentage of regional recurrence. On the other hand, high morbidity, complication and patients costs were added to the patients [19, 20].
The excellent results in malignant Melanoma permitted to others research teams to develop studies with similar goal in their field [21, 22, 23]. The patients with breast cancer diagnosed in early stage will be a good candidate because the axillary lymph node dissection is primarily a staging procedure, required to determine prognosis and select appropriate adjuvant therapy [24, 25].
The fundamental aims of this tools is to make it available to patients caught in early stages as our patient with palpable mass in the left breast but her axilla is negative. Screening breast cancer reduces breast cancer mortality and earlier detection. Unfortunately, current screening modalities are imperfect, suffering from limited sensitivity and high false- positive rates. Novel techniques in the field of breast imaging may soon play a role in breast cancer screening: digital breast tomosynthesis, contrast material–enhanced spectral mammography, US (automated three-dimensional breast US, transmission tomography, elastography, optoacoustic imaging), MRI, and molecular breast imaging. Artificial intelligence and radiomics have the potential to further improve screening strategies [26, 27].
Fluorodesoxiglucosa Positron emition tomography (FDG PET) and PET / CT have been shown to be most helpful in staging recurrent or metastatic breast cancer and in evaluating the response of locally advanced and metastatic breast cancer to treatment. These are the only current clinical indications for FDG PET/CT in breast cancer. Emerging data support the use of FDG PET / CT in advanced axillary disease and evaluation of regional nodal spread [28]. Axillary ultrasonography (US) can be easily incorporated into preoperative staging breast US. Thus, preoperative axillary US has become routine practice in many institutions for breast cancer management to predict axillary nodal status [29].
Giuliano applied intraparenchymal patent blue lymphatic mapping for lymph node evaluation of breast cancer. The development of portable gamma radiation detectors led Krag to investigate the use of intraparenchymal colloidal 99mTc- sulfide as a mapping agent to localize SLN in breast cancer. At the same time, Drs. Reintgen and Cox were developing a combined radio colloid and patent blue technique for mapping patients with melanoma or breast cancer. Multiple studies have shown that using radioisotopes or patent blue or a combination of both, SLN identification was 92%, 81% and 93% respectively, while false negative rates were 7%, 9% and 5% respectively [30, 31].
The radiopharmaceutical must have the ability to be retained in the first lymph node found along the path. Various formulations are being used such as: 99mTc-antimony trisulfite, 99mTc-colloidal sulfide, 99mTc-rhenium sulfide and human serum albumin Nano colloid or micro colloid. Colloidal 99mTc-sulfide is most commonly used. Several technique have been use for the administration of a radio colloid agent for selective lymph node biopsy in breast cancer surgery; our case the periareolar technique. All techniques have been reliable in experienced hands. It has been seen that the dermal technique identifies SLNs in the axilla more frequently compared to the peritumoral injection technique (98% vs. 90%). Regarding the dose, the dosage of these radiocolloid agents varies considerably within the literature and has been reported as low as 0.1 mCi (3.7 MBq) and up to 10 mCi (370 MBq) [32, 33]. Generally, in current practice, these radiocolloid agents are most commonly administered on the day of surgery in a dosage ranging between 0.4 mCi (14.8 MBq) and 1 mCi (37 MBq) as our case. The surgeon uses the probe to guide the dissection of the ‘hot’ node(s) and places the probe in the surgical bed after excision to confirm removal of the hot node(s). With the probe, the counts per unit of time are recorded, in the surgical field, on the node before excision (in vivo) and after excision (ex vivo). Background counts in tissue with the probe pointed away from the injection site, of ganglion activity, and the ratio of SN counts to background range from 10:1 to 20:1 are also recorded. After the SLN is identified and removed, the probe is used to measure residual counts in the surgical bed in order to identify and remove additional hot nodes.
Determining an adequate intraoperative assessment of the axilla with the gamma detection probe during breast cancer surgery is clearly related to the number of lymph nodes collected and meticulously explored, trying to identify all possible candidate sentinel nodes or lymph nodes will counts and at least 10% of the hottest SLN counts [34]. Martin et al reproduced the same results, demonstrating a false negative rate of 13.7% in patients who had only one SLN collected compared to 5.4% in patients who had two or more SLNs. harvested (P < 0.0001) such as our case with two hot lymph nodal collected [35]. SLN biopsy has a false negative rate (FNR) in surgical practice of 5.5-16.7%, that is, a low percentage of inability to identify a positive lymph node. The lowest data is achieved by using blue dye and radioactive tracer combined (6.7%). In a systematic review of large multifocal/multicentric tumors, it appears that the percentage of FNR is similar in small unifocal tumors [36, 37, 38].
There are a variety of methods used by pathologists, ranging from Histopathological examination to the use of immunohistochemistry (IHC) and even molecular biology studies such as polymerase chain reaction. The risk of false negatives is increased in those tissues with subtle metastases, which can easily go unnoticed if the resolution of the microscopic image is not high enough. In addition, the use of additional tools such as fast IHC is not standardized. But in general, a sensitivity of 73% (macrometastasis 94%; micro metastasis 40%) and a specificity of 100% (meta- analysis of 47 studies) are reported. The pathologist must be especially cautious when examining a slide with frozen tissue, in cases with metastatic lobular carcinoma, due to its soft cytological characteristics and infiltrative growth [39, 40, 41]. A modern approach is a technique known as single- step nucleic acid amplification (OSNA, Sysmex Corporation, Kobe, Japan). It is a molecular biology technique, which is developed intraoperative. It is based on the quantification of mRNA copies of cytokeratin 191 [42, 43, 44]. Studies with OSNA reported that pathological evaluation for the detection of breast cancer SLN metastases revealed that the former had a high specificity (94.8%), a high concordance rate (93.8%) and a value negative predictive (97.6%) [45].Multicenter prospective studies with a larger sample size are needed to definitively reveal the superiority of OSNA over pathological evaluation in predicting prognosis.
Conclusion
Each time that a new therapeutic tool is within reach of the oncologic patients, principally when his effectiveness have been demonstrated for a long time. Low incomes countries increase the challenge for her implementation. However, the multidisciplinary effort of the human resources and the help of the technology development of our institutions allow to jump the hard barrier that this entails, reaching a great achievement to the patients with breast cancer in our country. This first effort is not distant from the reported in the international literature.
Author Contribution
This first academic research in one more example that although our country with low economic resources, can make available to patients with early breast cancer a valuable tool that changes the traditional approach that until recently was performed in our country.
Declaration of Competing Interests
All authors have no conflict of interest to declare.
References
-
Robinson DS, Sample WF, Fee HJ, Holmes C, Morton DL, et al. (1977) Regional lymphatic drainage in primary malignant melanoma of the trunk determined by colloidal gold scanning. Surg Forum 28: 147-148.
-
Fee HJ, Robinson DS, Sample WF, Graham LS, Holmes EC, et al. (1978) The determination of lymph shed by colloidal gold scanning patients with malignant melanoma: a preliminary study. Surgery 84(5): 626-632.
-
Morton DL, Wen DR, Wong JH, Economou JS, Cagle LA, et al. (1992) Technical Details of Intraoperative Lymphatic Mapping for Early Stage Melanoma. Arch Surg 127(4): 392-399.
-
Krag DN, Weaver DL, Alex JC, Fairbank JT (1993) Surgical resection and radio localization of the sentinel lympho node in breast cancer using a gamma probe. Surg Oncol 2(6): 335-339.
-
Giuliano AE, Haigh PI, Brennan MB, Hansen NM, Kelley MC, et al. (2000) Prospective observational study of sentinel lymphadenectomy without further axillary dissection in patients with sentinel node-negative breast cancer. J Clin Oncol 18(13): 2553-2559.
-
Borgstein PJ, Pijpers R, Comans EF, van Diest PJ, Boom RP, et al. (1998) Sentinel lymph node biopsy in breast cancer: Guidelines and pitfalls of lymphoscintigraphy and gamma probe detection. J Am Coll Surg 186(3): 275- 283.
-
Sobin LH, Wittekind CH (2002) TNM Classification of Malignant Tumours. 6th(Edn), Wiley-Liss, New York, USA.
-
Chen SL, Iddings DM, Scheri RP, Bilchik AJ (2006) Lymphatic mapping and sentinel node analysis: current concepts and applications. CA Cancer J Clin 56(5): 292- 309.
-
Ross GL, Shoaib T, Soutar DS, MacDonald DG, Camilleri IG, et al. (2002) The first international conference of sentinel node biopsy in mucosal head and neck cancer and adoption of a multicenter trial protocol. Ann Surg Oncol 9(4): 406-410.
-
Ross GL, Soutar DS, Gordon MacDonald D, Shoaib T, Camilleri I, et al. (2004) Sentinel node biopsy in head and neck cancer: preliminary results of a multicenter trial. Ann Surg Oncol 11(7): 690-696.
-
Stoeckli SJ, Pfaltz M, Ross GL, Steinert HC, MacDonald DG, et al. (2005) The Second International Conference on Sentinel Node Biopsy in Mucosal Head and Neck Cancer . Ann Surg Oncol 12(11): 919-924.
-
Rao AA, Feneis J, Lalonde C, Ojeda-Fournier H (2016) A pictorial review of BI-RADS. Radiographics 36(3): 623- 639.
-
Bireley JD, Gospodarowicz MK (2017) TNM Clasification of Malignat Tumors. 8th(Edn), Wiley Blackwell, pp: 272.
-
WHO classification of Tumors (2019) Breast tumors. 5th(Edn), Vol. 2, France International agencies for research on cancer, Lyon, pp: 10.
-
Fitzgibbons P, Connolly J (2021) Template for reporting results of biomarker testing of specimens from patients with carcinoma of the breast. College of American pathologists.
-
Patterson HE, Hutton BF, Nair PG, Padhy AK (1999) Distance Assisted Training Program for Nuclear Medicine Technologists. J Nucl Med Technol 27(4): 318-320.
-
Heppner GH, Miller BE (1983) Tumors heterogeneity: biological implications and therapeutic consequence. Cancer Metastasis Rev 2(1): 5-23.
-
Fidler IJ, Kripke ML (1977) Metastasis results from preexisting variant cells within a malignal tumour. Science 197(4306): 893-895.
-
Sim FH, Taylor WF, Ivins JC, Pritchard DJ, Soule EH, et al. (1978) A prospective randomized study of the efficacy of routine elective lymphadenectomy in management of malignant melanoma: Preliminary results Cancer 41(3): 948-956.
-
Veronesi U, Adamus J, Bandiera DC, Brennhovd O, Caceres E, et al. (1982) Delayed regional lymph node dissection in stage I melanoma of the skin of the lower extremities. Cancer 49(11): 2420-2430.
-
Giuliano AE, Kirgan DM, Guenther JM, Morton DL (1994) Lymphatic mapping and sentinel lymphadenectomy for breast cancer. Ann Surg 391-398.
-
Veronesi U, Paganelli G, Galimberti V, Viale G, Zurrida S, et al. (1997) Sentinel-nodebiopsy to avoid axillary dissection in breast cancer with clinically negative lymph-nodes. Lancet 349(9069): 1864-1867.
-
Albertini JJ, Lyman GH, Cox C, Yeatman T, Balducci L, et al. (1996) Lymphatic mapping and sentinel node biopsy in the patient with breast cancer. JAMA 276(22): 1818- 1822.
-
Fein DA, Fowble BL, Hanlon AL, Hooks MA, Hoffman JP, et al. (1997) Identification of women with T1–T2 breast cancer at low risk of positive axillary nodes J Surg Oncol 65(1): 34-39.
-
Deckers PJ (1991) Axillary dissection in breast cancer: when, why, how much, and for how long? Another operation soon to be extinct? J Surg Oncol 48(4): 217- 219.
-
Mann RM, Hooley R, Barr RG, Moy L (2020) Novel Approaches to Screening for Breast Cancer. Radiology 297(2): 266-285.
-
Bahl M, Mercaldo S, Dang PA, McCarthy AM, Lowry KP, et al. (2020) Breast Cancer Screening with Digital Breast Tomosynthesis: Are Initial Benefits Sustained? Radiology 295(3): 529-539.
-
Rosen EL, Eubank WB, Mankoff DA (2007) FDG PET, PET/CT, and breast cancer imaging. Radiographics 27(Sup): S215-S229.
-
Kim GR, Choi JS, Han BK, Lee JE, Nam SJ, et al. (2018) Preoperative Axillary US in Early Stage Breast Cancer: Potential to Prevent Unnecessary Axillary Lymph Node Dissection. Radiology 288(1): 55-63.
-
Giuliano AE, Hunt KK, Ballman KV, Beitsch PD, Whitworth PW, et al. (2011) Axillary dissection vs no axillary dissection in women with invasive breast cancer and sentinel node metastasis: a randomized clinical trial. JAMA 305(6): 569-575.
-
Noguchi M, Tsugawa K, Miwa K, Yokoyama K, Nakajima KI, et al. (2000) Sentinel lymph node biopsy in breast cancer using blue dye with or without isotope localization. Breast Cancer 7(4): 287-296.
-
McCarter MD, Yeung H, Yeh S, Fey J, Borgen PI, et al. (2001) Localization of the sentinel node in breast cancer: identical results with same-day and day-before isotope injection. Ann Surg Oncol 8(8): 682-686.
-
Van der Ent FW, Kengen RA, van der Pol HA, Hoofwijk AG, (1999) Sentinel node biopsy in 70 unselected patients with breast cancer: increased feasibility by using 10 mCi radiocolloid in combination with a blue dye tracer. Eur J Surg Oncol 25(1): 24-29.
-
Povoski SP, Young DC, Walker MJ, Carson WE, Yee LD, et al. (2007) Re-emphasizing the concept of adequacy of intraoperative assessment of the axillary sentinel lymph nodes for identifying nodal positivity during breast cancer surgery. World J Surg Oncol 5: 18.
-
Cortés M, Bajén MT, Gil M, Benito E, Moreno A, et al. (2005) Simultaneous localization of non-palpable breast neoplasms and study of the sentinel lymph node (SN) using radio isotopic techniques. Rev Esp Med Nucl 24(2): 101-106.
-
Lyman GH, Somerfield MR, Bosserman LD, Perkins CL, Weaver DL, et al. (2014) American Society of Clinical Oncology Clinical Practice. Sentinel lymph node biopsy for patients with early-stage breast cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol 35(5): 561-564.
-
Krag DN, Anderson SJ, Julian TB, Brown AM, Harlow SP, et al. (2010) Sentinel-lymph-node resection compared with conventional axillary-lymph-node dissection in clinically node-negative patients with breast cancer: overall survival findings from the NSABP B-32 randomised phase 3 trial. Lancet Oncol 11(10): 927-933.
-
Spillane AJ, Brennan ME (2011) Accuracy of sentinel lymph node biopsy in large and multifocal/multicentric breast carcinoma--a systematic review. Eur J Surg Oncol 37(5): 371-385.
-
Kubikova E, Badidova J, Klein M, Beder I Jr, Benus R, et al. (2019) Sentinel lymph node- historical background and current views on its significance in complex management of breast cancer patients. Bratisl Lek Listy 120(6): 410- 416.
-
Liu LC, Lang JE, Lu Y, Roe D, Hwang SE, et al. (2011) Intraoperative frozen section analysis of sentinel lymph nodes in breast cancer patients: a meta-analysis and single-institution experience. Cancer 117(2): 250-258.
-
Layfield DM, Agrawal A, Roche H, Cutress RI (2011) Intraoperative assessment of sentinel lymph nodes in breast cancer. Br J Surg 98(1): 4-17.
-
Brambilla T, Fiamengo B, Tinterri C, Testori A, Grassi MM, et al. (One-Step Nucleic Acid Amplification in Breast Cancer Sentinel Lymph Node: A Single Institutional Experience and a Short Review. Front Med 2: 37.
-
Shiino S, Yoshida M, Jimbo K, Asaga S, Takayama S, et al. (2019) Two rare cases of endosalpingiosis in the axillary sentinel lymph nodes: evaluation of immunohistochemical staining and one-step nucleic acid amplifi cation (OSNA) assay in patients with breast cancer. Virchows Arch 474(5): 633-638.
-
Shimazu K, Miyake T, Okuno J, Naoi Y, Tanei T, et al. (2019) One-step Nucleic Acid Amplification Can Identify Sentinel Node-negative Breast Cancer Patients With Excellent Prognosis. Anticancer Res 39(3): 1447-1454.
-
Tamaki Y (2017) One-step nucleic acid amplification (OSNA): where do we go with it? Int J Clin Oncol 22(1): 3-10.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma