Stem Cell Dysfunction as a Key Point in Myelodysplastic Syndrome (MDS)
MDS microenvironment is complemented by non-cell autonomous alterations and autonomous expansion in some malignant clone as well which can state that the conceptualization of pre-leukemia has the complexity at the hematopoietic microenvironment in these patients. Moreover, the pre-leukemic/leukemic stem cell (LSC) model proposes a non-genetic mechanism in leukemic process which harmonized with the genetic model associated with epigenetic deregulation, contribute to leukemia heterogeneity. In addition, LSCs are different from leukemia initiating cells which are only defined by their abilities to initiate leukemia but with or without self-renewal ability. In fact our understanding of the complex pathobiology which now is recognized to arise from acquisition of sequential mutation in HSCs generally with non-genetic alterations that can give the impair normal leukocytes function and/or clonal gain additionally and go too fast to abnormality condition
Introduction
Myelodysplastic syndromes (MDSs) are clonal hematopoietic stem cell (HSC) malignancies that characterized by ineffective hematopoiesis. Some model suggest that genetic and/or epigenetic alterations that occur in HSC or HSC niche compromise HSC function, resulting in MDS, in other words, the niche or the HSC result in deregulated mi-RNAs which in turn induce aberrant expression of HSC intrinsic or extrinsic regulators, compromising HSC functions which all together leading HSC dysfunction, sever abnormalities in MDS hematopoietic microenvironment and so go to MDS development. In hematopoiesis the clonal dominance of a subset of HSCs and their progenitor cells as detectable by somatic mutations patterns is termed clonal hematopoiesis. So in cancer clonal evolution, cancer develops through the somatic mutations serial acquisition in an individual and its progeny. The mutations are usually acquired in a stepwise manner, such that each time a new driver mutation is acquired which can be seen as a cloning event.
Discussion
The mutation(s) associated with MDS (driver mutation) are often the same as normal elderly individuals or in hematopoietically, these individuals are normal and this clone should not be called pre-leukemic. But how? In response, after BMT, some patients with MDS , and patients with other leukemia like ALL may be cured, which means , initially, the BM and its hematopoietic microenvironment is malignant (Figures 1-3) but after BMT, HSC transplantation (HSCT) can repair the BM structure by HSCs maintenance chiefly and the other cells of BM niche as well (Figures 1-4) [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12]. The traditional concept of clonal dominance suggested the potent driver mutation(s) is needed to initiate the disease or transform it. Thus, there are some points on changing in malignant hematopoietic disease gradually such as MDS-IC cases as follows: a) in the BM microenvironment ( like leukemia) , b) in healthy HSCs suppression and go to clonal dominance effects which be acquired by HSCs and c) eventually contribute to the emergence of environmental perturbation and go to neoplastic clones evolution (Figure 1) [2, 5, 13, 14, 15, 16, 17, 18].
I-Hematopoietic Microenvironment Role in MDS
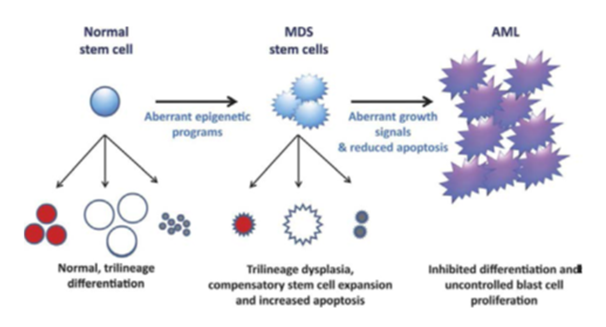
We know, in spite of MDS phenotypes variability, the patients share features with AML and other myeloid malignancies. Also, there are three fields in biology cancer including genetics, epigenetics and microenvironment are coming together to provide increasing clarity to the processes that determine stem-ness and in turn influence clinical outcome. Stem-ness is a central biological property or process upon which driver mutation(s) coalesce. Hence, mutation(s) can usually cause ineffective hematopoiesis as well as it can develop a major driver mutation like NMP1 or any fusion gene which resulting in frank AML with blast cells. Based on this information, the driver mutation(s) block differentiation providing these cells with a proliferative advantage to causing the peripheral blood cytopenias.
If AML reoccurs, the original clone or sub-clone of new blastic AML emerges from the pre-leukemic clone. Thus,1) the important point can be about HSCs, an accelerated HSC as well as a malignant stem cell and its microenvironment because of we follow the morphology report of BM cells and also PB during diagnosis till complete remission. That`s why timing will be critical because reports have found the pre-leukemic clone may be present for 8-10 years without relapsed blastic AML emergence. 2) Many of the random mutations that occur in these cells affect passenger genes or non-critical genes which means sometimes passenger mutation(s) can be important as a holder of vital role, namely bad luck happens when a mutation occurs in a gene that provides a proliferative advantage to the hematopietic cell. Actually, some true drivers may not make the cut which would be expected to cancer or any malignancy by chance, whilst some passengers may fortuitously do so. But what is the reason? In response, by understanding stem-ness properties within tumors which self- renewal capacity is typically deregulated in CSCs, namely we will be able to gain insight to the most important cells such as HSCs, committed stem cells or progenitor cells, etc. which make tumor microenvironment that can drive sequential rounds of tumor growth. In other words, identification of origin in MDS should facilitate a better understanding of MDS pathogenesis, because of to obtain the proof of leukemic clonal involvement of all blood cell lineages which not only promotes the development of the dominating leukemic lineage but also suppress the development of other lineages simultaneously that this position is confirmed for MDS cases and so HSCs are likely the more relevant population as compared with total BM cells when investigating the underlying defects in MDS. Therefore we have the reciprocal way that can embossed as a way of essential reacting and so change back to the between two conditions including MDS hematopoietic microenvironment (particularly HSCs) and genetic aberrations as well. In better expression, abnormalities of the BM stroma dominate in early MDS where there is disruption in interactions between the marrow stromal cell and MDS clones. Moreover , we know that normal interactions between HSCs and their niche are critical for the maintenance of HSC quiescence which can confirm an abnormal quiescence status of MDS HSC, that`s why the normal cell is selected by etiological events or exposures as the founder of malignant clone and its downstream, multiple sub-clones, so this is important point that indicate a normal stem cell (or a progenitor) can acquire a stem cell state as a consequence of the founder genetic lesion or local ecological stress or both of them which the final result of this situation is HSC dysfunction [1, 2, 3, 4, 5, 6, 7, 13, 19, 20].
![Figure 2: HSC dysfunction: In MDS pathogenesis, genetic and epigenetic abnormalities happen in HSCs and osteoblasts together that result in the deregulation of certain mi-RNAs in the cells which can follow by the subsequent HSC extrinsic regulators abnormal expression in osteoblasts or HSC intrinsic regulators in HSCs that can go to HSC dysfunction chiefly and MDS progression [1,16,21].](/fulltextimages/10872/fig_2.png)
Figure 2: HSC dysfunction: In MDS pathogenesis, genetic and epigenetic abnormalities happen in HSCs and osteoblasts together that result in the deregulation of certain mi-RNAs in the cells which can follow by the subsequent HSC extrinsic regulators abnormal expression in osteoblasts or HSC intrinsic regulators in HSCs that can go to HSC dysfunction chiefly and MDS progression [1, 16, 21].
Based on the information above, the beginning of stem cell dysfunction is happened, and also malignant stem cells provide a critical reservoir for MDS progression which can describe that there is a feedback mechanism between genetic alterations and MDS hematopoietic microenvironment in transferring process of information about the results of abnormal actions that the observations endorse on the view of malignant stem cells as the units of selection. So, in this context, the unit of selection is the cell but not any cell which means malignant stem cells originate from normal HSCs in the malignant cases, however to obtain the malignant clonal involvement proof of all blood cell lineages derived from multi-potent HSCs which the HSC not only promotes the dominating leukemic lineage development but also simultaneously suppress the other lineages development. In better expression, some properties of MDS cells are as follows: 1) Malignant stem cells have the essential properties required to function as the key units of selection, with respect to their proliferative potential specially and additionally long life. At last, these cells drive evolutionary progression of disease as well as provide reservoir for relapse or can go to drug resistance. 2) The lack of B-cell differentiation from MDS stem cells would mean that mature B-cells in peripheral blood may be derived from residual normal hematopoiesis because of the genetic and epigenetic abnormalities that occur in MDS HSCs make the cells deficient in the ability to differentiate to normal lymphocyte 3) Instead of lymphocyte efficient deletion, for lymphocyte production, there is an efficient compensatory mechanism by normal hematopoietic cells in the cases. 4) MDS is a clonal expansion of HSCs I which maturation is abnormal and cell production is ineffective resulting in cytopenia and anemia that is usually associated with low reticulocyte production inadequately and red cell distribution width reflecting anisocytosis increasingly which eventually the cells of PB and BM demonstrate dysplasia that involves one or more hematopoietic linages resulting MDS niche disruption in the disease [1, 5, 17, 22, 23].
MDS Morphologic Abnormalities Investigation
There is often considerable inter-observer variation where the dys-erythropoiesis or granulocytic hypo- granularity is subtle, but better consistency should be among observers in identifying cells.
So in BM and peripheral blood (PB) overview, we have anemia, thrombocytopenia or leukopenia. Moreover, in the erythrocyte precursors comprise nuclear & cytoplasmic abnormalities, such as inter-nuclear bridging, fragmentation, budding, more than one nucleus per cell, megaloblastic changes and abnormal granulopoiesis including nuclear hyper-segmentation or hypo-segmentation, dense chromatin clumping, pseudo Pelger-Huet cells, etc. Lastly, MDS describes a diverse clonal disorders group of HSCs or other progenitor cells with ineffective erythropoiesis, abnormal dysplastic cells as well as clonal evolution potential. Additionally, the cells in PB and BM demonstrate dysplasia that involves one or more hematopoietic lineages. Erythrocytes may show macrocytosis, anisocytosis, basophilic stippling and pappenheimer bodies. MDS diagnosis depend on the presence of cytopenia(s) and morphologic dysplasia, also it can present in a variety of neoplastic and non-neoplastic conditions (Figures 1-3). Told all, MDS subtypes are still defined by the dysplasia degree and blast count mostly which there are some challenges in distinguishing MDS from idiopathic cytopenia of undetermined significance( ICUS) and clonal hematopoiesis of indeterminate potential(CHIP) [8, 10, 11, 12, 13, 14, 15, 24] On the other hand, we can show the eliminating MDS HSCs in MDS curing as follows in the (Figure 4).
![Figure 3: In MDS, dysplasia may involve one or more hematopoietic series that means HSCs clonal expansion. The maturation is abnormal (dysplastic) and production ineffective resulting in many cells being ruined before the cells reach to the systemic circulation [22-26].](/fulltextimages/10872/fig_3.png)
![Figure 4: In evolution of MDS in the figure, after secondary AML the remission is happened [1,2] and the patient is cured, but why and how?](/fulltextimages/10872/fig_4.png)
We know, over the years, some studies have found that the alteration in the BM microenvironment can lead to hematological malignancies. For example, also, in murine models, activation of the normal HSC niche improves recovery from radiation and chemotherapy injury and suppresses CML disease progression, impairing LSC maintenance in a syngeneic model. Furthermore, MDS can be cured by allogeneic HSC transplantation and stromal cells remain of patient origin after this procedure, it has been postulated that alterations in MDS stroma must be secondary to interactions with clonal MDS cells and reversible upon their eradication. Regarding this point, hematopoiesis depends on critical interactions that occur between stem cells and their microenvironment [12, 25, 26, 27, 28].
Some alterations in the normal activity of MSCs and their osteoblastic lineage cell (OBC) derivatives, leading to a major remodeling of the endosteal BM niche in the development of myeloproliferative neoplasm (MPN), which mainly affects normal HSCs, with minimal effects on transformed LSCs. The main fact that LSC maintenance is unaffected by the remodeled OBCs could be, in large part, due to their different requirement in adhesion molecules for homing and retention in the BM compared to normal HSCs. Also, in the clonal origins of MDS, MSCs have been questioned. MDS cases derived MSCs seem to have reduced clonogenicity, increased senescence and additionally defect in adipogenic and osteogenic differentiation potential, particularly in high risk categories like refractory anemia with excess blasts.
Actually, in nature evolution creates biodiversity and this in turn makes an entire ecosystem robust. In this case, acquired additional mutation(s) evolve and develop gradually to AML, viz. In the malignant disease , the diversity within these cells at the genetic and functional level together with their co-existence in the malignant microenvironment ,also increases the fitness of malignancy, allowing these cells go to more imbalance status and also to more progression wholly [1, 2, 3, 4, 5, 6, 12, 13, 17, 25].
II-Genetic Aberrations in MDS
The mutation(s) associated with MDS (driver mutation) are often the same as normal elderly individuals or in hematopoietically, these individuals are normal and this clone should not be called pre-leukemic. But how? In response, after BMT, some patients with MDS , and patients with other leukemia like ALL may be cured, which means , initially, the BM and its hematopoietic microenvironment is malignant but after BMT, HSC transplantation (HSCT) can repair the BM structure by HSCs maintenance chiefly and the other cells of BM niche as well (Figures 5 & 6) [2, 3, 4, 5, 6, 7, 8, 10, 11, 12].
![Figure 5: Diagnostic findings in 5q- syndrome: A) Hypo-lobulated megakaryocytes B) Note loss of material from chromosome 5 long arm [22,28].](/fulltextimages/10872/fig_5.png)
The 5-A of abnormal cell morphology is not specific for MDS and it can also occur in some leukemia, like CML (but in the case we have not 5q-). In addition, the genetic aberration (5q-) is the commonest cytogenetic abnormality in MDS (Figure 5B).
![Figure 6: Statistical evaluation of MDS clonal cytogenetic abnormalities. The aberrations occur in about 50% of cases with MDS [27].](/fulltextimages/10872/fig_6.png)
The detection of these abnormalities are MDS presumptive which accompanied by refractory cytopenias , even in the morphological dysplasia absence. Some reports stated that we have complex karyotype in primary MDS till 20% and also in therapy related MDS till 90% [28]. But why is the rate elevated, particularly in primary MDS? It is noticeable that in MDS epigenomic alterations- global aberrations in histone and chromatin modification are common. As well, MDS represent different routes to acquiring the mutation(s) necessary for AML development (Figures 3-4) vs. There are some normal karyotypes or no genetic aberrations in some MDS cases interestingly (Figure 6) which can be embossed [27]. In addition, Moreover based on our knowledge, we have some problems as follows: 1. In some studies that used BM cells from patients and healthy controls little overlap is seen in the deregulated mi-RNAs. 2. Some researchers reported that the differences in mi- RNA expression were shown among early and advanced MDS, in cases with CD34+ cells which particularly is not similar between RAEB-I and RAEB-II cases in the matter.
At last, MDS diagnosis made by excluding other non MDS causes of cytopenias with some combination of severe dysplastic cell morphology typically, increased marrow blasts and usually an abnormality of karyotype. But PB and BM abnormality is a reflection of ruined hematopoietic microenvironment in MDS, notably, in some cases, which the cytogenetic and molecular genetic tests may be normal (Figures 1-4,6) [11, 14, 15, 16, 17, 18, 21, 29, 30].
Conclusion
The environmental factors is embossed which can be actual and very effective in MDS hematopoietic microenvironment and its phenotype. Overall, these studies define bone marrow not only as a HSCs reservoir, their progeny and other niche cells, but rather as the active complex reactions organ, where HSC is prominent that can be capable of adapting the demand signals to hematopoiesis in response to hemato-immunological signals and maintain themselves in a steady state as well. In general, these studies have led that MDS is a transformed HSCs disease (Figure 7) with can go to the stem cell dysfunction gradually or in other words MDS conceptualization is as a stem cell disorder.
![Figure 7: Stem cell dysfunction: In myelodysplastic syndrome pathogenesis, the stem cell dysfunction play a key role in center of the clonal hematopoietic stem cell disorder [30].](/fulltextimages/10872/fig_7.png)
References
-
Gibson JG, Steensma DP (2023) Myelodysplastic syndromes. In Hoffman R, et al. Hematology Basic Principles and Practice 61(2): 977-1000.
-
Koeffler HP, Leong G (2017) Pre-leukemia: one name, many meanings. Leukemia 31(3): 534-542.
-
Natarejan P, Jaiswal S, Kathiresan S (2018) Clonal hematopoiesis, somatic mutations in blood cells and atherosclerosis. Circ Genom Precis Med 11(7): e001926.
-
Balderman SR, Calvi LM (2014) Biology of BM failure syndromes: role of microenvironment and niches. Hematology Am Soc Hematol Educ Program 2014(1): 71-76.
-
Hutchison RE (2017) Leukocytic disorders. In: Mc pherson RA, et al. (Eds,). Henry’s Clinical Diagnosis and management by laboratory methods. 23rd (Edn.), Elsevier, pp: 606-658.
-
Dander E, Palmi C, D’Amico G, Cazzaniga G (2021) The bone marrow niche in B-cell acute lymphoblastic leukemia: the role of microenvironment from pre- leukemia to overt leukemia. Int J Mol Sci 22(9): 4426.
-
Lucas D (2017) The bone marrow microenvironment for hematopoietic stem cells. Adv Exp Med Biol 1041: 5-18.
-
Yao Y, Li F, Huang J, Jin J, Wang H (2021) Leukemia stem cell bone marrow microenvironment interplay in acute myeloid leukemia development. Exp Hematol Oncol 10(1): 39.
-
Walter MJ, Shenn D, Shao J, Ding L, White BS, et al. (2013) Clonal diversity of recurrently mutated genes in myelodysplastic syndromes. Leukemia 27(6): 1275- 1282.
-
Asada S, Kitamura T (2021) Clonal hematopoiesis and associated diseases: A review of recent findings. Cancer Sci 112(10): 3962-3971.
-
Chotinantakul K, Leeanansaksiri W (2012) Hematopoietic stem cell development, niches and signaling pathways. Bone Marrow Res 2012: 270425.
-
Grassinger J, Mueller G, Zaiss M, Kunz-Schughart LA, Andreesen R, et al. (2006) Differentiation of hematopoietic progenitor cells towards the myeloid and B- lymphoid lineage by hepatocyte growth factor (HGF) and thrombopoietin (TPO) together withearly acting cytokines. Eur J Hematol 77(2): 134-44.
-
Mian SA, Bonnet D (2021) Nature or Nurture? Role of the bone marrow microenvironment in the genesis and maintenance of myelodysplastic syndromes. Cancers 13(16): 4116.
-
Weissman IL (2015) Stem cells are units of natural selection for tissue formation, for germline development, and in cancer development. Proc Natl Acad Sci USA 112(29): 8922-8928.
-
Greaves M (2013) Cancer stem cells as a unit selection. Evo Appl 6(1): 102-108.
-
Li J (2012) Myelodysplastic syndrome hematopoietic stem cell. Int J Cancer 133(3): 525-533.
-
Delforge M (2003) Understanding the pathogenesis of myelodysplastic syndromes. Hematol J 4(5): 303-309.
-
Greaves M (2009) Darwin and evolutionary tales in leukemia. Hematology, The Ham-Wasserman lecture. Hematology Am Soc Hematol Educ Program pp: 3-12.
-
Bydlowski SP, Janz FDL (2012) Hematopoietic stem cell in acute myeloid leukemia development. In Pelayo R, et al. Advances in hematopoietic stem cell research. In Tech Europe pp: 261-276.
-
Bonin MV, Jambor HK, Teipel R, Stolzel F, Thiede C, et al. (2021) Clonal hematopoiesis and its emerging effects on cellular therapies. Leukemia 35: 2752- 2758.
-
Issa JPJ (2013) The myelodysplastic syndrome as a prototypical epigenetic disease. Blood 121(19): 3811- 3817.
-
Pozdynyakova O, Hasserjian RP (2018) Myelodysplstic syndrome. In: Weksler BB, et al. (Eds.), Wintrobe`s Atlas of Clinical Hematology 7: 276-294.
-
Tkachuk DC (2007) Myelodysplastic syndromes. In: Tkachuk DC, et al. (Eds.), Wintrobe’s, Atlas of Clinical Hematology 3: 94-104.
-
Kim JA, Jae-Seung S, Ga-Young L, Yim HW, Tae-Min K, et al. (2015) Micro-environmental remodeling as a parameter and prognostic factor of heterogeneous leukemogenesis in acute myelogenous leukemia. Cancer Res 75(11): 2222-2231.
-
Zhao LP, Schell B, Sebert M, Kim R, Lemaire P, et al. (2021) Prevalence of UBA1 mutations in MDS/CMML patients with systemic inflammatory and auto-immune disease. Leukemia 35(9): 2731-2733.
-
Vardiman JW (2001) Myelodysplastic Syndrome: Myelodysplastic syndrome associated with isolated del (5q) chromosome abnormality (5q- Syndrome), – 5. ASH Image Bank.
-
Nybakken GE, Bagg A (2014) The genetic basis and expanding role of molecular analysis in the diagnosis, prognosis, and therapeutic design for myelodysplastic syndromes. The J Mol Diagn 16(2): 145-158.
-
Raj K, Mufti GJ (2016) The myelodysplastic syndromes. In: Hoffbrand AV, et al. (Eds.), Postgraduate Hematology 7th (Edn.), 25: 438- 473.
-
Bolli N, Vassiliou G (2016) The molecular basis of hematological malignancies. In: Hoffbrand AV, et al. (Eds,). Postgraduate Hematology 7th (Edn.), 18: 314-331.
-
Platzbecker U, Meredyth-Stewart M, Ehninger G (2007) The pathogenesis of myelodysplastic syndrome (MDS). Cancer Treatment Reviews 33(1): S53-S58.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma