Flawed and Facsimile- Thoracic SMARCA4-Deficient Undifferentiated Tumour
Thoracic SMARCA4-deficient undifferentiated tumour emerges as a distinct, aggressive neoplasm of thoracic cavity delineating unique morphological, phenotypic and molecular features associated with rapid clinical progression and inferior overall survival. Tumefaction is associated with definitive molecular modifications confined to SMARCA4 gene, especially within ATPase subunits of SWI/SNF chromatin modifying complex. Neoplasm manifests as an enlarged tumefaction compressing adjacent thoracic viscera with frequent pulmonary and mediastina involvement. Cytological smears demonstrate cellular smears comprised of singular cells or clusters and sheets of non-cohesive Tumour cells configuring glandular structures or papillary articulations. Tumefaction is comprised of sheets of non-cohesive, monomorphic, spherical cells pervaded with variegated nuclei and prominent nucleoli. Thoracic SMARCA4-deficient undifferentiated tumour mandates discernment of cogent features as foci of rhomboid or poorly differentiated tumour cells, significant loss of expression of SMARCA4 and SMARCA2 and focal or diffuse immune reactivity to minimally two biomarkers as SOX2, CD34 or SALL4. Tumour cells appear immune reactive to synaptophysin, chromogranin and stem cell markers as CD34, SALL4 and SOX2. Tumefaction is immune non-reactive to cytokeratin, Claudin 4, POU2F3 and exhibits a concurrent loss of expression of BRG1 and BRM. Thoracic SMARCA4-deficient undifferentiated tumour requires demarcation from diverse vascular tumours, epithelioid angiosarcoma, epithelioid sarcoma, liposarcoma, gastrointestinal stromal tumour, malignant melanoma, NUT pulmonary carcinoma, malignant peripheral nerve sheath tumour, large cell lymphoma, germ cell tumours, rhabdomyosarcoma, Ewing’s sarcoma, CIC-DUX4 sarcoma, various undifferentiated sarcomas, mesothelioma and anaplastic or undifferentiated carcinomas devoid of keratin expression. Thoracic SMARCA4- deficient undifferentiated tumour may be challenging to alleviate as therapeutic targets appear difficult to obtain and neoplasm is associated with lymphatic dissemination.
Introduction
Thoracic SMARCA4-deficient undifferentiated tumour emerges as an aggressive neoplasm incriminating the thoracic cavity. Neoplasm configures a distinct entity delineating unique morphological, phenotypic and molecular features and expounds precise diagnostic immunohistochemistry.
Previously designated as SMARCA4-deficient thoracic sarcoma or SMARCA4-deficient thoracic sarcomatoid tumour, tumefaction demonstrates an aggressive clinical course with rapid progression and inferior overall survival. As clinical representation of SMARCA4-deficient undifferentiated tumour is ambiguous, an amalgamation of biochemical evaluation, histopathological assessment and molecular features is necessitated in order to appropriately categorize the neoplasm. Features such as concurrent immune reactivity to CD34, SALL4 and SOX2 in combination with lack of diffuse expression of epithelial markers appear indicative of the neoplasm. Tumefaction is associated with definitive molecular modifications confined to SMARCA4 gene, especially within ATPase subunits of SWI/SNF chromatin modifying complex. Genomic alterations within SWI/SNF complex may be accompanied by ‘rhabdoid’,’ dedifferentiated’ or ‘undifferentiated’ morphological subtypes wherein tumour may emerged within diverse sites. Tumefaction enunciates distinct molecular profile with SMARCA4 genetic mutations and RNA expression disparate from non-small cell pulmonary carcinoma [1, 2].
Tumour mutational burden of SMARCA4-deficient undifferentiated tumour is concordant with SMARCA4- deficient non-small cell carcinoma manifesting as clear cell adenocarcinoma or exceptionally as squamous cell carcinoma. Thus, distinction between aforesaid neoplasms may be challenging. Nevertheless, tumour magnitude of SMARCA4-deficient undifferentiated tumour is significantly enlarged, in contrast to SMARCA4-deficient non-small cell carcinoma. Tumefaction is associated with loss of or diffuse, severe decimated expression of BRG1 or SMARCA4 and loss of BRM or SMARCA2 expression [1, 2].
Tumefaction is commonly discerned within subjects with history of intense cigarette smoking. A male predilection is observed. Thoracic SMARCA4-deficient undifferentiated tumour manifests as an enlarged tumefaction compressing circumscribing thoracic viscera. Pulmonary and mediastinal involvement is frequently encountered. Cytological examination exhibits cellular smears comprised of singular cells or clusters and sheets of non-cohesive tumour cells with spaces between individual tumour cells. Neoplasm may configure glandular structures or papillary articulations. Focal keratinization or tumour necrosis may be encountered [2, 3].
Tumour cells appear as miniature, intermediate or enlarged cells with spherical, elliptical, polygonal, spindle shaped or irregular outline and are permeated with indistinct, pale or densely staining cytoplasm with micro- vacoules. Intracytoplasmic or intra-nuclear inclusions may be exemplified. Cellular perimeter may be distinct or indistinct. Tumour cell nuclei are pervaded with inconspicuous or prominent, centric or eccentric nucleoli. Miniature, intermediate or enlarged tumour cell nuclei configure as spherical, elliptical, polygonal or demonstrate irregular nuclear outline with nuclear moulding. Streaking artefact may be enunciated [2, 3]. Cellular pleomorphism may be absent to significant. Pleomorphic or multinucleated tumour cells may occur. Tumour cells with classic rhabdoid morphology are characteristically imbued with distinct, hyaline cytoplasmic inclusions. Nevertheless, rhabdoid cellular morphology may be absent, infrequent or demonstrate focal areas [2, 3]. Generally, singular cells or non-cohesive sheets of neoplastic cells are predominant and intermingled with focal, non-cohesive rhabdoid tumour cells and disseminated inflammatory cells. Focal tumour necrosis is discerned. Occasionally, mucin rich tumour cells imbued with intracytoplasmic mucin and eccentric nuclei may be delineated.
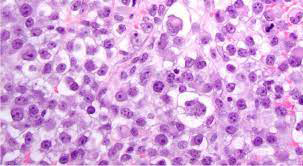
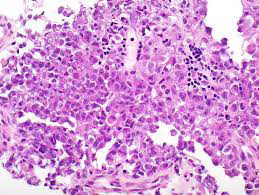
Features such as focal tumour necrosis and monomorphic tumour cells admixed with foci of pleomorphic tumour cells appear pathognomonic. Exceptionally, composite tumours with thoracic SMARCA4-deficient undifferentiated tumour admixed with non-small cell carcinoma may be encountered [3, 4]. Upon microscopy, neoplasm represents with a population of undifferentiated round cells. Typically, tumefaction is comprised of sheets of non-cohesive, monomorphic cells pervaded with variegated nuclei and prominent nucleoli [3, 4] (Figure 1). Thoracic SMARCA4- deficient undifferentiated tumour mandates discernment of cogent features as ~foci of rhomboid tumour cells or poorly differentiated tumour cell phenotype ~comprehensive or significant loss of expression of SMARCA4 and SMARCA2 ~focal or diffuse immune reactivity to minimally two biomarkers as SOX2, CD34 or SALL4 [3, 4]. Foci of rhomboid tumour cells are observed wherein rhomboid cells appear incorporated with distinct, hyaline cytoplasmic inclusions. Mitotic activity is significant. Tumour necrosis is exemplified (Figure 2). Composite tumours delineate a combined morphology of SMARCA4-deficient undifferentiated tumour admixed with conventional non-small cell carcinoma [3, 4].
Courtesy: Journal of thoracic oncology
Courtesy: Semantic scholar
Epithelial Tumours
Papilloma
Squamous cell papilloma NOS
Squamous cell papilloma, inverted
Glandular papilloma
Mixed squamous cell and glandular papilloma Adenoma
Sclerosing pneumocytoma
Alveolar adenoma
Papillary adenoma
Bronchiolar adenoma/ciliated muconodular papillary tumour
Mucinous cystadenoma
Mucous gland adenoma
Precursor glandular lesions
Atypical adenomatous hyperplasia
Adenocarcinoma in situ
Adenocarcinoma in situ, non-mucinous
Adenocarcinoma in situ, mucinous
Adenocarcinoma
Minimally invasive adenocarcinoma
Minimally invasive adenocarcinoma, non-mucinous
Minimally invasive adenocarcinoma, mucinous
Invasive non-mucinous adenocarcinoma
Lepidic adenocarcinoma
Acinar adenocarcinoma
Papillary adenocarcinoma
Micro-papillary adenocarcinoma
Solid adenocarcinoma
Invasive mucinous adenocarcinoma
Mixed invasive mucinous and non-mucinous adenocarcinoma Colloid adenocarcinoma Foetal adenocarcinoma Adenocarcinoma, enteric type Adenocarcinoma NOS Squamous precursor lesions Squamous cell carcinoma in situ Mild squamous dysplasia Moderate squamous dysplasia Severe squamous dysplasia Squamous cell carcinoma Squamous cell carcinoma NOS Squamous cell carcinoma, keratinizing Squamous cell carcinoma, non keratinizing Basaloid squamous cell carcinoma Lympho-epithelial carcinoma Large cell carcinoma Adenosquamous carcinoma Sarcomatoid carcinoma Pleomorphic carcinoma Giant cell carcinoma Spindle cell carcinoma Pulmonary blastoma Carcinosarcoma Other epithelial tumours NUT carcinoma Thoracic SMARCA4-deficient undifferentiated tumour Salivary gland-type tumours Pleomorphic adenoma Adenoid cystic carcinoma Epithelial-myoepithelial carcinoma Mucoepidermoid carcinoma Hyalinising clear cell carcinoma Myoepithelioma Myoepithelial carcinoma Neuroendocrine tumours of lung Precursor lesion Diffuse idiopathic neuroendocrine cell hyperplasia
Neuroendocrine tumours
Carcinoid tumour NOS/ neuroendocrine tumour NOS
Typical carcinoid/neuroendocrine tumour grade I
Atypical carcinoid/neuroendocrine tumour grade II
Neuroendocrine carcinomas
Small cell carcinoma
Combined small cell carcinoma
Large cell neuroendocrine carcinoma
Combined large cell neuroendocrine carcinoma
Tumours of ectopic tissue
Melanoma
Meningioma
Mesenchymal tumours specific to the lung Pulmonary hamartoma Chondroma
Diffuse lymphangiomatosis
Pleuropulmonary blastoma
Intimal sarcoma
Congenital peribronchial myofibroblastic tumour
Pulmonary myxoid sarcoma with EWSR1-CREB1 fusion PEComatous tumours Lymphangioleiomyomatosis PEComa benign PEComa malignant Haematolymphoid tumours MALT lymphoma Diffuse large B cell lymphoma NOS Lymphomatoid granulomatosis NOS Lymphomatoid granulomatosis, grade I Lymphomatoid granulomatosis, grade II Lymphomatoid granulomatosis, grade III Intravascular large B cell lymphoma Langerhans cell histiocytosis Erdheim-Chester disease Table1: Classification of Lung Tumours World Health Organization 2021[4].
Discussion
Tumour cells appear immune reactive to synaptophysin and chromogranin. Stem cell markers as CD34, SALL4 and SOX2 appear immune reactive. Tumefaction is immune non- reactive to cytokeratin and Claudin 4. Majority (~95%) of tumour cells appear immune non-reactive to Claudin 4 and exhibit a concurrent loss of expression of BRG1 and BRM, a feature which is pathognomonic of thoracic SMARCA4- deficient undifferentiated tumour. Neoplastic cells appear immune non-reactive to POU2F3 [5, 6]. Fine needle aspiration cytology (FNAC) or endobronchial ultrasound (EBUS) guided fine needle aspiration cytology may be optimally adopted to appropriately discern the predominantly central neoplasms. Morphological assessment of obtained surgical tissue samples is optimal and recommended [5, 6]. Evaluation of SMARCA4 genetic alteration by molecular assay may be beneficially adopted for categorizing thoracic SMARCA4- deficient undifferentiated tumour as well as non-small cell pulmonary carcinoma. Cogent genetic analysis may be contemplated for additional neoplastic categorization [5, 6].
Thoracic SMARCA4-deficient undifferentiated tumour requires segregation from high grade, undifferentiated neoplasms confined to pulmonary parenchyma or thoracic cavity demonstrating monomorphic, round cell morphology or neoplasms with rhabdoid morphology which are immune non-reactive to cytokeratin [5, 6]. Generally, demarcation is necessitated from lesions such as diverse vascular tumours, epithelioid angiosarcoma, epithelioid sarcoma, liposarcoma, gastrointestinal stromal tumour, malignant melanoma, NUT pulmonary carcinoma, malignant peripheral nerve sheath tumour, large cell lymphoma, germ cell tumours, rhabdomyosarcoma, Ewing’s sarcoma, CIC-DUX4 sarcoma, various undifferentiated sarcomas, mesothelioma and anaplastic or undifferentiated carcinomas devoid of keratin expression [5, 6]. Thoracic SMARCA4- deficient undifferentiated tumour may be challenging to alleviate as therapeutic targets appear difficult to obtain. However, possible adoption of precise targeted chemotherapy requires additional evaluation. Neoplasms of advanced grade appear unamenable to comprehensive surgical eradication. SMARCA4-deficient undifferentiated tumour may exhibit predilection for lymphatic dissemination, an exceptionally discerned feature of sarcomas [5, 6].
References
-
Jiang J, Chen Z, Gong J, Na Han, Hongyang Lu (2023) Thoracic SMARCA4-deficient undifferentiated tumor. Discov Oncol 14(1): 51.
-
Kezlarian B, Montecalvo J, Bodd FM, Chang JC, Riedel E, et al. (2023) Diagnosis of thoracic SMARCA4-deficient undifferentiated tumor in cytology. Cancer Cytopathol 131(8): 526-534.
-
Kito Y, Kawashima K, Saigo C, Hasegawa M, Nomura S, et al. (2022) Thoracic SMARCA4-deficient undifferentiated tumors with ganglioneuroma and enchondroma: implications for SLC7A11 and ARID1A expression: a case report. Diagn Pathol 17: 29.
-
Nicholson AG, Tsao MS, Beasley MB, Borczuk AC, Brambilla E, et al. (2022) The 2021 WHO Classification of Lung Tumors: Impact of Advances Since 2015. Journal of Thoracic Oncology 17(3): 362-387.
-
Perret R, Chalabreysse L, Watson S, Serre I, Garcia S, et al. (2019) SMARCA4-deficient thoracic sarcomas: clinicopathologic study of 30 cases with an emphasis on their nosology and differential diagnoses. Am J Surg Pathol 43(4): 455-465.
-
Rekhtman N, Montecalvo J, Chang JC, Alex D, Ptashkin RN, et al. (2019) Thoracic SMARCA4-deficient sarcomatoid tumors represent primarily smoking- related undifferentiated carcinomas rather than primary thoracic sarcomas. J Thorac Oncol 15(2): 231-247.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma