Phenylenediamine Poisoning: Beyond the Respiratory Distress
<p>The paraphénylèdiamine or PPD is a black coloring agent entering the composition of hair colorings, essentially used in hairstyle as dye for hair, but also in the temporary tattoos, in association with the henna. It is mainly met in coloring them with bottoms (stockings), with shoe polishes, with rubbers, with shoes, with capillary dyes (not exhaustive list) The PPD, extremely sensitizing, can cause very significant allergic reactions that may develop life-threatening immediately by installing an acute respiratory distress, then the occurrence of rhabdomyolysis with risk of acute renal failure. These complications are two conventionally known by the clinician. Nevertheless, the occurrence of myocarditis, often overlooked, is a very serious complication, to raise with clinical signs of shock or in the presence of a rhythm disorder. We report the case of a 28 year old patient hospitalized for management of acute respiratory distress following the acquisition of PPD, whose evolution was marked by the occurrence of myocarditis confirmed by cardiac MRI.</p>
Introduction
The intoxication paraphenylène- diamine (PPD) is formidable even at very low doses, since it causes a high mortality [1, 2]. The initial clinical features were dominated by respiratory distress and the installation of acute renal failure by rhabdomyolysis, and rarely by myocarditis, which remains a serious complication, since it can put into life-threatening. This is the case of our patient who presented, in addition to acute renal insufficiency and acute respiratory distress, myocarditis.
A 28-year old woman, married with two children, hospitalized two hours after deliberate ingestion of PPD for care of acute respiratory distress with head and neck edema, having justified a emergency tracheotomy, given the impossibility of endotracheal intubation. Laboratory work found high creatine phosphokinase (CPK) [59850Ul/l]. The urinary pH was lower than 6. The rest of the biological assessment was without anomalies.
The téléthorax and ECG were no anomalies. The change was mainly marked by the appearance of acute renal failure, oliguric, with dark colored urine (Figure 1), having justified symptomatic treatment, based on abundant rehydration, on average 12 liters per day, alkaline. The objective is to obtain a urinary PH more than 6.5.

the diamine paraphenylène.
While the patient was asymptomatic, ECG done at J6 of
hospitalization was without defects, with dosage troponin
Tc, which were 50 times normal. The diagnosis of a toxic
myocarditis was strongly suspected, confirmed by
echocardiography, which objectified hypokinesia with a
lower dyskinesia anteroseptal without impaired left
$$ \text{ventricular function (ejection fraction} = 60\%) \text{ with} $$
pericardial separation, and confirmed by cardiac MRI ,
done three weeks later. The development, clinical and
biological (graph 1) was favorable, and the patient was in
décanulée 10èmejour successfully.
![Figure 2: Classical Appearance ECG myocarditis, simulating a myocardial infarction. This myocarditis often results in an overall collapse of hypokinesia with ejection fraction (EF) on echocardiography, which was not the case for our patient: EF = 60%. Cardiac MRI (Figure 3), baseline examination confirmed the diagnosis of myocarditis by late contrast enhancement in intra myocardial or epicardial under which is a different specific element of ischemic pathology [7-9]. Transthoracic echocardiography objective often a global hyperkinesia with collapse of the ejection fraction, which in our case was without defects. This is cardiac MRI confirms the diagnosis by late contrast enhancement in intra myocardial or sub epicardial [7-9], observed in our patient. In our patient, the diagnosis was suspected in a moderate bradycardia to 50 per minute with premature ventricular contractions, and elevated cardiac enzymes at 50 times the normal rate (troponin Ic), confirmed by cardiac MRI taken late by the contrast subepicardial (Figure 3).](/fulltextimages/251/fig_2.jpeg)
Graph 1: Evolution of CPK.
Discussion
The clinical picture of ingestion to PPD, the lethal dose in humans is estimated at 10 g, is initially dominated by respiratory signs, type of acute respiratory distress accompanied often with head and neck edema, one of the mechanisms would be an allergic component, which settled a few hours, 15-20 minutes to 2-6 hours (2 hours for our patient) after ingestion. This respiratory distress often arises indicating a rescue tracheotomy [3, 4], explained by the difficulty, see the impossibility of endotracheal intubation, which was the case in our patient. The respiratory impairment further comprises, rhabdomyolysis respiratory muscles, including the diaphragm, causing a superimposed respiratory exhaustion. Finally, acute respiratory distress syndrome (ARDS) remains possible with late onset, to the 4 -5th days [5]. The cardiac, typical myocardite, documented for the first time in 1995, was the object of recent publications which put the point on a new clinical aspect of these poisonings, and which seem to be bound (connected) to the dose of ingested PPD. It could be a direct attack of myocardial fiber membrane lipid peroxidation and calcium storage of inhibition by the sarcoplasmic reticulum to the origin of a calcium overload [6]. She must be suspected in case of state of shock, electric signs (ischemia-diffuse lesion, ventricular premature beats, tachycardia and ventricular fibrillation, or even a plus ST elevation mimicking a wave Pardee (Figure 2), and / or biological (increased troponin Ic rates, new increase of CPK).
![Figure 3: Cardiac MRI after injection of gadolinium, with contrast enhancement sub epicardial type of strip at the bottom wall (arrows). In the short term, myocarditis can compromise the prognosis for heart failure, refractory cardiogenic shock, ventricular arrhythmias see sudden death. Moreover, it can become chronic causing dilated cardiomyopathy [10- 11]. The evolution is favorable in most cases, with healing without sequelae, but the risk of dilated cardiomyopathy or sudden death should alert the clinician by early diagnosis and, consequently, a specialized care. The patient was put under antiplatelet agent and an ACE inhibitor, after consulting specializing in cardiology.](/fulltextimages/251/fig_3.png)
Figure 2: Classical Appearance ECG myocarditis, simulating a myocardial infarction. This myocarditis often results in an overall collapse of hypokinesia with ejection fraction (EF) on echocardiography, which was not the case for our patient: EF = 60%. Cardiac MRI (Figure 3), baseline examination confirmed the diagnosis of myocarditis by late contrast enhancement in intra myocardial or epicardial under which is a different specific element of ischemic pathology [7, 8, 9]. Transthoracic echocardiography objective often a global hyperkinesia with collapse of the ejection fraction, which in our case was without defects. This is cardiac MRI confirms the diagnosis by late contrast enhancement in intra myocardial or sub epicardial [7, 8, 9], observed in our patient. In our patient, the diagnosis was suspected in a moderate bradycardia to 50 per minute with premature ventricular contractions, and elevated cardiac enzymes at 50 times the normal rate (troponin Ic), confirmed by cardiac MRI taken late by the contrast subepicardial (Figure 3).
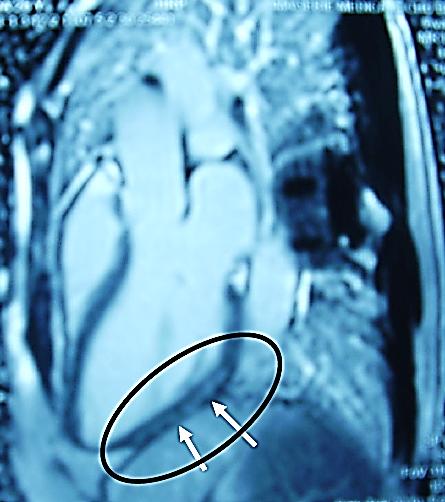
Figure 3: Cardiac MRI after injection of gadolinium, with contrast enhancement sub epicardial type of strip at the bottom wall (arrows). In the short term, myocarditis can compromise the prognosis for heart failure, refractory cardiogenic shock, ventricular arrhythmias see sudden death. Moreover, it can become chronic causing dilated cardiomyopathy [10, 11]. The evolution is favorable in most cases, with healing without sequelae, but the risk of dilated cardiomyopathy or sudden death should alert the clinician by early diagnosis and, consequently, a specialized care. The patient was put under antiplatelet agent and an ACE inhibitor, after consulting specializing in cardiology.
Conclusion
The severity of these poisonings encourages the clinician in-depth knowledge of this pathology. If respiratory distress is the most classic clinical form, the search for a cardiac complication, like myocarditis, must be systematic to reduce short-term morbidity and mortality, and long-term specialized monitoring, given the unpredictable evolution of this complication.
References
-
Moutaouakil S, Elmouknia M, Benslama A, Chara M, Menbhi L, et al. (1999) Intoxication à la paraphénylènediamine. Les cahiers du médecin 22: 10-13.
-
Adnet P, Travernier B, Haudecoeur G, Krivosic-Horber R (1994) Actualités en réanimation et urgences. In: Srlf (eds), Rhabdomyolyses : hypothèses physiopathologiques. Paris: Arnette pp. 235-248.
-
Squali J, Drissi R, Maazouzi KA (1991) Systemic toxicity of para-phenylenediamine. Apropos of a case. Cah Anesthesiol 39: 559-560.
-
SFMU (2008) l’intoxication à la paraphénylène- diamine au Maroc. Urgences, pp. 769.
-
Yabe K (1992) The effect of a p-phenylenediamine containing hair dye on the Ca2+ mobilization in the chemically skinned skeletal muscle of the rat. Nippon Hoigaku Zasshi 46(2): 132-140.
-
Abdel-Aty H, Boyé P, Zagrosek A, Wassmuth R, Kumar A, et al. (2005) Diagnostic performance of cardiovascular magnetic resonance in patients with suspected acute myocarditis: comparison of different approaches. J Am Coll Cardiol 45(11): 1815-1822.
-
Hunold P, Schlosser T, Vogt FM, Eggebrecht H, Schmermund A, et al. (2005) Myocardial late enhancement in contrast-enhanced cardiac MRI: distinction between infarction scar and non- infarction-related disease. AJR Am J Roentgenol 184(5): 1420-1426.
-
Mahrholdt H, Goedecke C, Wagner A, Meinhardt G, Athanasiadis A, et al. (2004) Cardiovascular magnetic resonance assessment of human myocarditis: acomparison to histology and molecularpathology. Circulation 109(10): 1250-1258.
-
Doolan A, Langlois N, Semsarian C (2004) Causes of sudden cardiac death in young Australians. Med J Aust 180(3): 110-112.
-
Phillips M, Robinowitz M, Higgins JR, Boran KJ, Reed T, et al. (1986) Sudden cardiac death in Air Force recruits. A 20-year review. JAMA 256(19): 2696- 2699.
-
Eckart RE, Scoville SL, Campbell CL, Shry EA, Stajduhar KC, et al. (2004) Sudden death in young adults: a 25-year review of autopsies in military recruits. Ann Intern Med 141(11): 829-834.
- Pattern of Gonadal Hormones in Oral Testosterone-Supplimented Male Wistar Rats with Diabetes-Induced Hypogonadism
- Re-Evaluation of the Genotoxicity of Currently Used Food Dyes in Mouse Multiple Organs Via Continuous Administration by Drinking Using the Comet Assay
- Pharmacogenetics of Type 2 Diabetes Mellitus: Linking Genetic Variability to Drug Efficacy and its Cardiovascular Outcomes
- Exploratory Proteomic Profiling of SARS-CoV-2 Infected THP-1 Macrophages Reveals Alterations in Inflammatory Response and Cellular Metabolism
- Study of Genotoxicity of Hepatocarcinogens in Multiple Organs in Mice by Feeding and Drinking Using the Comet Assay
- Spirulina Polypeptides Inhibit the Growth of Human Lung Tumor (H460) Cells