Idiosyncratic Reactions: Drugs Induced Steven Johnson‘s Syndrome
Stevens-Johnson syndrome (SJS) is a type of severe skin reaction. Together with toxic epidermal necrolysis (TEN) and Stevens-Johnson/toxic epidermal necrolysis (SJS/TEN), it forms a spectrum of disease, with SJS being less severe. Early symptoms of SJS include fever and flu-like symptoms. A few days later the skin begins to blister and peel forming painful raw areas. Mucous membranes such as the mouth are also typically involved. Complications include dehydration, sepsis, pneumonia, and multiple organ failure. Work was begun by taking oration from Nile College, and then was stamped in Ministry of Health for ethical clearance purposes. After the questionnaire paper were made ,we met in patients suffering from SJS and from their answers we made statements, and the rest of our work was by checklist method from hospital records which depended on patients files. All of the previous work was done under high privacy and after data collection we sent our data to analysis and were analyzed by SPSS23 method. Results were interpreted and recommendations were forwarded.
Introduction
Adverse drug reactions are a major complication of modern drug therapy, they are a considerable cause of patient morbidity and account for a significant number of patients death. Furthermore many serious adverse reactions occur in patients with diseases which in themselves are not necessarily life threatening, such as depression and epilepsy, but do require long term drug treatment. It is therefore essential that a better understanding of such reactions is obtained in order to assess more accurately the risk benefit ratio for the treatment of a patient with a particular drug [1].
Adverse Drug Reactions may be Classified as Follow
Type A: These reactions are predictable in terms of the primary and secondary pharmacology of the drug and are usually dose-dependent. Examples of this type of reaction include hypoglycemia with oral hypoglycemic and hypotension with antihypertensive. Such reactions should be anticipated, and can often be eliminated by dose reduction [2].
Type B (Idiosyncratic): This type of reaction is unpredictable from the knowledge of the basic pharmacology of the drug and do not show any simple dose-response relationship, i.e. there is a lack of correlation between the dose and risk of toxicity. These reactions occur in only a small percentage of the population, hence the term idiosyncratic reaction, but are often serious and account for many drug-induced [3]. Type C: Reactions associated with long-term drug therapy, examples of which include benzodiazepine dependence and analgesic nephropathy. These reactions are well-described and can be anticipated [4]. Type D: Delayed effects such as carcinogenicity and teratogenicity. It is thought that such toxicities are precluded by the extensive programmed of preclinical mutagenicity and carcinogenicity studies that a new chemical entity must undergo before a product license is granted [5].
In this study we will focus on type (B) reactions or idiosyncratic reactions, a term used to describe adverse reactions which occur in a small number of patients. These reactions are often serious and are a major cause of iatrogenic disease.
Materials and Methods
The work was based on hospital visits or rounds for data collection, and our method was questionnaire plus checklist. Study group is consisting of 118 patients; this group is divided into two parts. Hospitalized patients and
Age
41-60years 61-90years check list files from hospital records. They were grouped as 68 females, 17 males and 33 children. The study group ages ranges between 3 months and 90 years old. We started our collection by filling questionnaire forms from direct patients meeting or co patient's reports then after data collection we began to go through group's tests. After data collection we send our samples for statistical analysis and were done as SPSS23.
Results
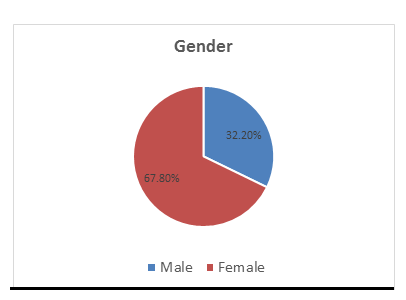
This result was obtained to know in which gender the higher percentage of patients.
Medani AB, et al. Idiosyncratic Reactions: Drugs Induced Steven Johnson‘s Syndrome. Adv Clin Toxicol 2018, 3(4): 000143.
0 0 Social Status
32.20%
77% single Married
This study was made to know the effect of social status on susceptibility.
Career
1st Qtr 2nd Qtr 3rd Qtr 4th Qtr
This survey evaluates the relation between patient's type of career and the susceptibility.
social support
50.00%
25.40% 35.60% 39%
0.00% No Moral Financial
This type of questionnaire showed the role of society with their SJS patient and the type of support if present.
Medani AB, et al. Idiosyncratic Reactions: Drugs Induced Steven Johnson‘s Syndrome. Adv Clin Toxicol 2018, 3(4): 000143.
Accompanying Social
Changes
5.10%
0 0
94.90% yes No
This study was done to find the social changes in patients and their interaction with their community.
Medical Insurance?
12.70% 0 0
87.30% yes No
This study was made forth purpose of knowledge of the patient can tolerance to treatment costs or he/she has insurance.
Discussion
From symptoms there is no difference between idiosyncratic reaction Steven Johnson's Syndrome and infective Steven Johnson's Syndrome till the laboratory findings or diagnosis assure the presence of causative organism [6]. When the illness was detected as result of drug reaction, the drug under the cause must be stopped then suitable care will take place. And if there is an organism associated with the case, antimicrobial therapy may take place in the treatment plan [7].
In Khartoum hospital for Dermatology and Venereology, Steven Johnson Syndrome was found to affect female more than male and has the higher percentage in the age group between 21-40 years' old people from both gender. Also Steven Johnson's Syndrome found mostly in housewife's between all careers in comparison. Community has different support for their Steven Johnson's Syndrome patients and the mostly available type of support is moral support. Also Steven Johnson Syndrome not affect sociality in changes words like divorce or isolation due to patients illness but there is small group their community isolate them as a result of perception of this case may be contagious. Most Steven Johnson's syndrome patients in Khartoum Hospital not have medical insurance. As treatment patients receive intravenous rehydration, analgesia with NSAIDs, antimicrobials like tetracycline , proto pump inhibitor like Omeprazole, topical corticosteroids ointments like Fusiderm (betamethasone + fusidic acid) and /or oral corticosteroids as emergency and sometimes there are additional drugs in the plan of therapy of severe patients. Most patients' answers about family history to the illness are NO history to it, but a few numbers show the answer of yes they show it in their relatives but with other causative agents. Symptoms of the recurrence are more severe than the first admission and the distribution throughout the body is in high percentage in comparison to the first illness evaluation.
As a Report
Steven Johnsons Syndrome does not totally associate with social status but in small scale it is. Because it is idiosyncratic reaction and there is no direct linkage between it and social status [8, 9, 10, 11].
Conclusion
Treatment of Steven Johnsons Syndrome is firstly by stopping the agent under the cause then begin with fluid resuscitation via IV rehydration plus NSAIDS, analgesics in most cases Paracetamol then addition of topical corticosteroid mostly fusidic acid with betamethasone plus oral corticosteroid the mostly used is Prednisolone tabs in it is different strengths plus proton pump inhibitor Omeprazole plus topical antibacterial Tetracycline [7].
References
-
Lerch M, Mainetti C, Beretta-Piccoli TB, Harr T (2017) Current Perspectives on Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis. Clinical Reviews in Allergy & Immunology 54(1): 147-176.
-
Brahma DK, Wahlang JB, Marak MD, Sangma M (2003) Adverse Drug Reactions, In the Elderly. J Pharmacol Pharmacother 4(2): 91-94.
-
Edwards IR, Aronson JK (2000) Adverse Drug Reactions, Definition, Diagnosis, and Management. Lancet 356(9237): 1255-1259.
-
Fabiano V, Mameli C, Zuccotti GV (2012) Adverse Drug Reactions. In Newborns, Infants, And Toddlers: Pediatric Pharmacovigilance Between Present and Future. Expert Opin Drug Saf 11(1): 95-105.
-
Pirmohamed M, Park BK (2003) Adverse Drug Reactions. Br Clinpharmmacol 12: 194-200.
-
Stein KM, Schlappner OLA, Heaton CL, Decherd JW (1972) Demonstration of Basal Cell Immunofluorescence in Drug Induced Toxic Epidermal TEN. Br J Dermal 86: 246-252.
-
Br J (1992) Idiosyncratic Reactions of Anti-biotic, Penicillin Induced Steven Johnsons Syndrome. Clin Pharmac 34: 377-395.
-
Turner S, Nunn AJ, Fielding K (1999) Adverse Drug Reactions. Acta Paediatr 88: 8-965.
-
Bond CA, Raehl CL (2006) Adverse Drug Reaction in United States Hospital. Pharmacotherapy 26(5): 601- 608.
-
Stern RS, Chal HL (1989) Usefulness of Case Report Literature in Determining Drugs Responsible For Toxic Epidermal Necrolysis. J AM Acad Dermatol 21(2): 317-322.
-
Uetrecht J (1990) Drug Metabolism by Leukocytes and its Role in Drug Induced Lupus and Other Idiosyncratic Drug Reaction. Crit Rev Toxicol 20(4): 213-235. Medani AB, et al. Idiosyncratic Reactions: Drugs Induced Steven Johnson‘s Syndrome. Adv Clin Toxicol 2018, 3(4): 000143.
- Pattern of Gonadal Hormones in Oral Testosterone-Supplimented Male Wistar Rats with Diabetes-Induced Hypogonadism
- Re-Evaluation of the Genotoxicity of Currently Used Food Dyes in Mouse Multiple Organs Via Continuous Administration by Drinking Using the Comet Assay
- Pharmacogenetics of Type 2 Diabetes Mellitus: Linking Genetic Variability to Drug Efficacy and its Cardiovascular Outcomes
- Exploratory Proteomic Profiling of SARS-CoV-2 Infected THP-1 Macrophages Reveals Alterations in Inflammatory Response and Cellular Metabolism
- Study of Genotoxicity of Hepatocarcinogens in Multiple Organs in Mice by Feeding and Drinking Using the Comet Assay
- Spirulina Polypeptides Inhibit the Growth of Human Lung Tumor (H460) Cells